Please wait as we load hundreds of rigorously documented facts for you.
Please wait as we load hundreds of rigorously documented facts for you.
For example:

Because word choices can influence people’s opinions about abortion and other issues,[1] [2] [3] Just Facts adheres to Standards of Credibility requiring language that is straightforward and accurate.
One of the most-debated aspects of abortion terminology is the label applied to what or who is being aborted. Those who think abortion should be generally illegal often use the terms “unborn child” and “unborn baby.” According to Webster’s College Dictionary and Black’s Medical Dictionary, the word “child” can apply prior to birth,[4] [5] but both dictionaries employ the word “baby” only from the point of birth onwards.[6] [7]
In contrast, those who think abortion should be generally legal often use the word “fetus,” a clinical term derived from a Latin word meaning “offspring” or “newly delivered.”[8] As explained by Dorland’s Illustrated Medical Dictionary, a fetus is:
Simply put, when referring to humans, the words “fetus” and “fetal” apply from nine weeks after fertilization until birth.[10] [11] Yet, numerous major news organizations have misapplied these terms to both before and after this period.[12] [13] [14] [15] [16] [17]
Journalism guidelines disparage the use of medical jargon,[18] [19] [20] [21] but media outlets selectively employ it in their coverage of this issue. For example, journalists frequently use the clinical term “fetus” when reporting on abortion, but they use the word “mother” to refer to a pregnant woman instead of the clinical term, “gravida.”[22] [23] Conversely, when the topic is not abortion, reporters often shun the word “fetus” and use “baby” or “child” to describe humans in the womb.[24] [25] [26] [27] [28]
In accord with the common journalism standard to “never use … a scientific word or a jargon word if you can think of an everyday English equivalent,”[29] Just Facts uses the term “pre-birth human” to describe the object of an abortion. This conveys reality in plain and scientifically accurate language, as shown by:
Furthermore, it would be unscientific and contradictory to recognize that a child born at 24 weeks after fertilization is a human but claim that one in the womb at 32 weeks is not.
Unless otherwise stated, this research uses the word “abortion” in the sense of an induced abortion—not a spontaneous one, which is also called a miscarriage.[38]
* The average length of a full-term pregnancy is 38 weeks. Obstetricians normally use a figure of 40 weeks, but this is actually the time between the first day of the last menstrual period (LMP) and childbirth. On average, the first day of the LMP occurs 2 weeks before fertilization.[39] [40] [41]
Fertilization (2 Weeks Post-LMP)
* Fertilization normally takes place within one day of intercourse but can occur up to six days later.[42] [43]
* During fertilization, the genetic composition of humans is formed.[44] This genetic information determines sex, eye color, hair color, and facial features. It also influences characteristics such as intelligence and personality.[45]
* The four defining characteristics of life are present during or soon after fertilization:[46]
* Fertilization produces a new, biologically unique human:
3 Weeks After Fertilization (5 Weeks Post-LMP)
* The eyes and spinal cord are visible and the developing brain has two lobes.[64] [65]
4 Weeks After Fertilization (6 Weeks Post-LMP)
* The heart is beating and a circulatory system is in place.[66] [67] [68] [69] [70] [71] [72] [73]
* Specific brain components and internal organs such as the lungs are beginning to develop and can be identified.[74]
7 Weeks After Fertilization (9 Weeks Post-LMP)
* The cerebrum, or largest part of the brain, has divided into hemispheres.[75] [76]
* Muscles and nerves begin working together. When the upper lip is tickled, the arms move backwards.[77]

9 Weeks After Fertilization (11 Weeks Post-LMP)
* More than 90% of the body structures found in a full-grown human are present. The medical classification changes from an embryo to a fetus. This dividing line was chosen by embryologists because from this point forward, most development involves growth in existing body structures instead of the formation of new ones.[79] [80]
* Pre-birth humans move body parts without any outside stimulation.[81]
10 Weeks After Fertilization (12 Weeks Post-LMP)
* All parts of the brain and spinal cord are formed. The heart pumps blood to every part of the body.[82]
* The whole body is sensitive to touch except for portions of the head. Facial expressions become evident.[83]
11 Weeks After Fertilization (13 Weeks Post-LMP)

12 Weeks After Fertilization (14 Weeks Post-LMP)
* Electrical signals from the nervous system are measurable. After an abortion, efforts to suckle are sometimes observed.[85] [86]
* Conscious “motor planning” and “social behavior” begin.[87]
13 Weeks After Fertilization (15 Weeks Post-LMP)
14 Weeks After Fertilization (16 Weeks Post-LMP)
* Coordinated movements of the arms and legs occur.[89]
16 Weeks After Fertilization (18 Weeks Post-LMP)
* Eye movements begin.[90]

18 Weeks After Fertilization (20 Weeks Post-LMP)
* The portion of the brain responsible for functions such as reasoning, memory and language (the cerebral cortex) has the same number of nerve cells as a full-grown adult. Pain sensory receptors have spread to all portions of the skin and mucous membranes.[92] [93]
20 Weeks After Fertilization (22 Weeks Post-LMP)
* Pre-birth humans sleep, awake, and can hear sounds.[95]

* For comprehensive facts about the capacity of humans to feel pain at this stage of development, read Just Facts’ article, “When Do Humans Begin to Feel Pain?“
* Up through approximately this stage of pregnancy, U.S. Supreme Court decisions in Roe v. Wade and Planned Parenthood v. Casey prohibited states from banning abortions for any reason.[98] [99] [100] [101] [102] These rulings were overturned in 2022.
24 Weeks After Fertilization (26 Weeks Post-LMP)
* The blink-startle reflex and taste buds are functional. Pre-birth humans swallow more amniotic fluid if a sweetener is added to it.[103] [104]
* The grip is strong enough to hold onto an object that is moving up and down.[105]
* If born and given specialized care, the survival rate is more than 80%.[106]
28 Weeks after Fertilization (30 weeks Post-LMP)
* If exposed to an 85 decibel noise while sleeping (about as loud as a blender), pre-birth humans exhibit the “motor behaviors that accompany the crying state.”[107] [108]
* Premature infants born at this time are more sensitive to pain than infants who are born at 38 weeks, and infants who are born at 38 weeks are more sensitive to pain than infants at 3–12 months after birth.[109] [110]
* If born and given specialized care, the survival rate is more than 95%.[111]
32 Weeks After Fertilization (34 Weeks Post-LMP)

* Pre-birth humans react with facial expressions to the flavors of different foods eaten by their mothers.[113]
38 Weeks After Fertilization (40 Weeks Post-LMP)
* Average point in time when humans are born. At birth, the medical classification changes from a fetus to a neonate.[114] [115]
* The Supreme Court’s rulings in Roe v. Wade and Planned Parenthood v. Casey prohibited states from banning abortion up until birth unless the ban contained an exception for the “health of the mother.” Under these rulings (which were overturned in 2022):
* In 2005, the Guttmacher Institute—a research organization whose “Guiding Principles” include support for legalized abortion[121] [122]—published a survey of 1,209 women who obtained abortions at 11 U.S. clinics. The survey was “not strictly nationally representative,” but the “social and demographic characteristics of respondents were similar to those of two nationally representative surveys.” When these women were asked to list all reasons why they were getting an abortion:
* When these same women were asked to list the “most important” reason they were getting an abortion:
* The margin of sampling error for the results of this survey is ± 3 percentage points with at least 95% confidence.[126]
* The same study found:
* In 2017, the journal Contraception published an analysis of studies in 14 countries that examined reasons why women get abortions. This analysis was limited to nationally representative studies of women who had abortions at clinics. Based on such studies from Asia, Africa, Latin America, and North America, the authors found:
* Planned Parenthood has claimed:
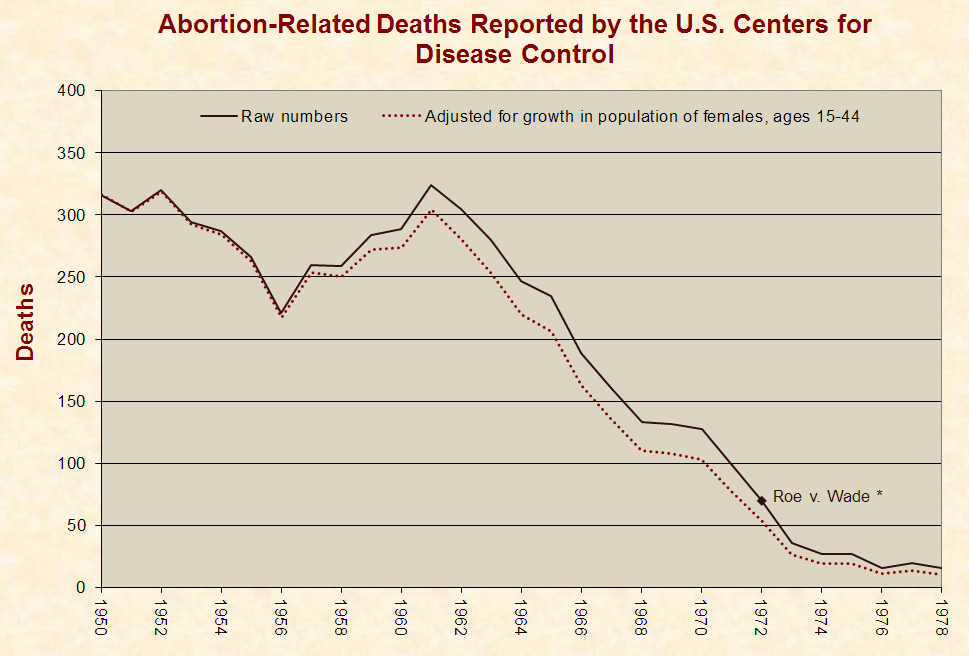
* Planned Parenthood cited no sources for the statements above. According to the U.S. Centers for Disease Control (CDC), whose death statistics from legal abortions have been accepted and used by Planned Parenthood:[130] [131] [132]
* In the years surrounding Roe v. Wade, abortion deaths reported by the CDC varied as follows:
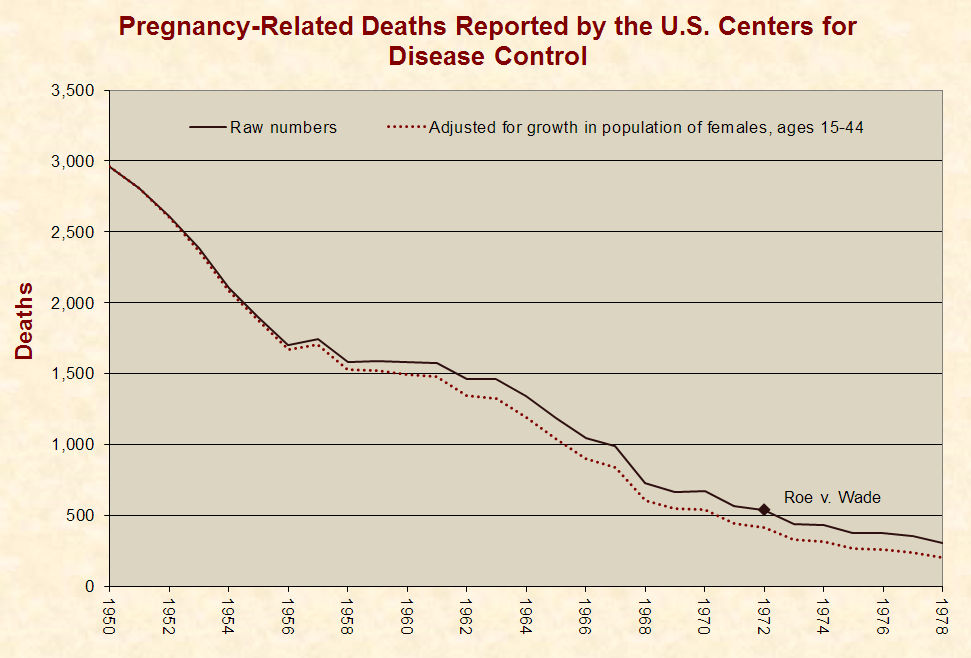
* Per the CDC, the coding system used to classify pregnancy-related deaths “precludes a determination of the real causes of maternal death.”[135] In the years surrounding Roe v. Wade, pregnancy-related deaths reported by the CDC varied as follows:
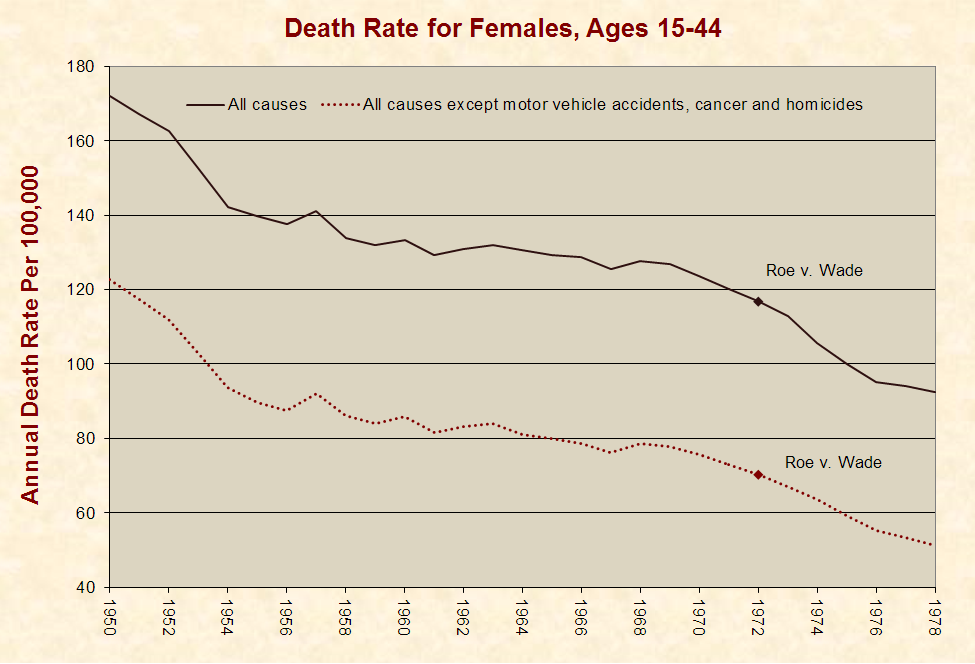
* Per the CDC, the coding system used to classify deaths in general is inadequate because only a single code is assigned to each death, but “several factors may contribute to a death.”[137] In the years surrounding Roe v. Wade, the death rate for females during their primary reproductive years varied as follows:
* A “fact sheet” published by Planned Parenthood claims that:
* “Christiansen & Collins, 2006” contains no information about the risk of death associated with abortion or childbirth. It contains figures for the risk of death “once a woman has become pregnant” as compared to the number of live childbirths in the U.S. These figures are not broken down to show abortion or childbirth-related deaths.[140]
* Citing data from the CDC, a previous version of the same Planned Parenthood fact sheet states that the “risk of death associated with childbirth is about 10 times as high as that associated with abortion.”[141] [142] [143]
* The CDC has reported the following information about the data it provides for pregnancy-related deaths:
* A 2002 national survey of physicians found that 98% think the reporting of medical practice errors is obstructed due to fear of lawsuits.[155]
* From 1989 through 1992, the CDC’s National Center for Health Statistics reported zero abortion-related deaths in the state of Maryland.[156] [157] [158] [159]
* During 1989 in the state of Maryland:
* In 1987, the New York City Commissioner of Health wrote a letter to abortion clinics warning them to be careful about using too much anesthesia. The letter stated:
* For the same time period, the CDC’s Division of Reproductive Health reported a total of 42 legal abortion-related deaths in the United States.[176]
* If both of these numbers are accurate, it would mean that 71% of the legal abortion-related deaths in the United States occurred in one city where about 3% of the population lived.[177]
* An “Abortion Services” page on Planned Parenthood’s website has claimed:
* A 2007 paper in the Journal of Reproductive Medicine cites 59 studies that exhibit a statistically significant association between abortion and the risk of premature births in subsequent pregnancies. In five of the largest and more recent of these studies, all found increases in premature births before 32 weeks gestation in women who had an abortion. All of these studies also found that this risk escalated when more than one abortion was performed.[179] Children born before 32 weeks are at increased risks for early death, cerebral palsy, blindness, deafness and other health complications.[180]
* Various pages on the website of Planned Parenthood have claimed:
* The country of Finland has socialized medicine and keeps detailed health records of its citizens.[185] A search of these records over the years 1987–1994 found that 1,347 women of reproductive age (15–49 years old) committed suicide. A 1996 study of this data found that women who had an abortion were about 5.9 times more likely to commit suicide in the year following this event than women who delivered a child:
|
Events Within the Last Year of the Woman’s Life |
Annual Suicide Rate Per 100,000 |
|
Delivered a child |
5.9 |
|
Had an abortion |
34.7 |
* The State of California pays the costs of childbirths and abortions for low income women. A study of 173,279 California women who had a state-funded childbirth or abortion in 1989 found that 53 of them committed suicide within eight years of their childbirth or abortion. A 2002 study of this data found that women who had an abortion were about 2.5 times more likely to commit suicide in the eight years following this event than women who delivered a child:
|
Events in Woman’s Life From 1989 to 1997 |
8-Year Suicide Rate Per 100,000 |
|
Delivered a child |
24.9 |
|
Had an abortion |
62.8 |
* In 2008, the Los Angeles Times reported:
* The California study cited above controlled for mental disorders by eliminating those women who had been treated for a psychiatric problem in the year prior to their childbirth or abortion. Correcting for this, women who had an abortion were about 3.3 times more likely to commit suicide in the eight years following this event than women who delivered a child:
|
Events in Woman’s Life From 1989 to 1997 |
8-Year Suicide Rate Per 100,000 |
|
Delivered a child |
19.1 |
|
Had an abortion |
63.0 |
* In 2013, the journal Psychiatry and Clinical Neurosciences published an analysis of 30 scientific studies examining abortion and subsequent mental health. Reporting “a general convergence of the data,” the authors found that among studies comparing:
* In 2019, the Journal of Psychiatric Research published the results of a 10-year study in Germany on the mental health outcomes of 35,162 women who recently experienced their first live childbirth or abortion and had never been diagnosed with four major “psychiatric disorders” that “are frequently triggered by stressful life events.”[191] By comparing women with the same gynecologists and ages, the study found that women who had an abortion were:
* Limitations of the German study (and others about this topic) include the following:
* Medical journals, abortion clinics, and media outlets have used the term “late-term abortion” to describe those that are performed:
– Journal of Pregnancy[201]
* A 2013 paper in the journal Perspectives on Sexual and Reproductive Health estimates that “more than 15,000” abortions are performed each year in the U.S. “at 21 weeks or later.”[220] This paper:
* After fertilization, these human developmental milestones occur:
– New England Journal of Medicine[226]
– Encyclopedia of Human Biology[227]
– Encyclopedia of Human Biology[228]
– PLoS ONE[229]
– Before We Are Born: Essentials of Embryology and Birth Defects[230]
– Fetal Diagnosis and Therapy[231]
– New England Journal of Medicine[232]
– Anesthesiology[233]
– American Medical Association Complete Medical Encyclopedia[234]
* At 20 weeks after fertilization, pre-birth humans look like this:
* The Supreme Court’s rulings in Roe v. Wade and Planned Parenthood v. Casey prohibited states from banning abortion up until birth unless the ban contained an exception for the “health of the mother.” Under these rulings (which were overturned in 2022):
* Before Roe was overturned, at least 24 states enacted laws that banned late-term abortions without the broad “health” exceptions required by Roe.[241] Proponents of legalized abortion decided not to challenge these laws in the U.S. Supreme Court. Per Yale Law School fellow Emily Bazelon, abortion advocates were “wise to avoid” suing states that prohibit “abortion after 20 or 22 weeks of pregnancy” because:
* As described by the Washington Post, a “dismemberment dilation and evacuation” abortion is a “late-term procedure” in which “the fetal limbs are pulled off the body in utero, sometimes while the fetus is still alive.”[243] [244] [245] [246] [247] [248]
* Dismemberment abortions are the most common type of late-term abortion.[249] [250] [251]
* As detailed in a 2003 Supreme Court ruling, dismemberment abortions are performed in the following manner:
* The procedure used for dismemberment abortions is illegal for slaughtering livestock because federal humane law requires that all livestock be killed in a manner that renders them immediately unconscious.[253] [254]
* The procedure used for dismemberment abortions is illegal for killing “living non-human mammals, birds, reptiles, or amphibians” because the “Preventing Animal Cruelty and Torture Act” bans purposely crushing or mutilating such animals.[255] [256] [257]
* The states of Illinois and Oregon have laws against dismembering a dead human but allow the dismemberment of living pre-birth humans.[258] [259] [260] [261]
* As of January 2023, 13 states had enacted bans on dismemberment abortions, but 6 of these laws were not in effect due to court rulings.[262]
* Before Roe v. Wade and Planned Parenthood v. Casey were overturned in 2022, those rulings were used to block laws that prohibit dismemberment abortions.[263] [264] [265] [266]
* As described by American Medical News (a publication of the American Medical Association[267]) and other medical literature, a “partial-birth” abortion is a “late-term procedure” that involves:
* In 1995, Republican Congressman Charles Canady of Florida sponsored a bill to ban the use of partial-birth abortions on live pre-birth humans except if “necessary to save the life of a mother.”[272] It was cosponsored by 19 Democrats and 96 Republicans.[273] This bill passed Congress with 90% of Republicans voting for it and 62% of Democrats voting against it. It was vetoed by Democratic President Bill Clinton. A vote to override the veto passed in the House and failed in the Senate by 8 votes.[274] [275] [276]
* In 1997, Republican Congressman Gerald Solomon of New York sponsored a bill to ban the use of partial-birth abortions on live pre-birth humans except if “necessary to save the life of a mother.”[277] It passed Congress with 95% of Republicans voting for it and 62% of Democrats voting against it. It was vetoed by Democratic President Bill Clinton. A vote to override the veto passed in the House and failed in the Senate by 3 votes.[278] [279] [280]
* In 2003, Republican Senator Rick Santorum of Pennsylvania sponsored a bill to ban the use of partial-birth abortions on live pre-birth humans except if “necessary to save the life of a mother.”[281] It was cosponsored by 2 Democrats and 43 Republicans.[282] Congress passed this bill with 95% of Republicans voting for it and 62% of Democrats voting against it. Republican President George W. Bush then signed it into law.[283] [284]
* The enacted law does not ban late-term abortions, only the partial-birth procedure.[285] It does not prohibit giving a lethal injection to a pre-birth human and performing a partial-birth abortion afterwards.[286]
* After this law was enacted, several abortion providers challenged it in court.[287] In 2007, the U.S. Supreme Court upheld the constitutionality of the law in a 5–4 vote.[288] Of the five Supreme Court justices who ruled to uphold the law, Barack Obama voted against the nomination of two of them and identified two of the others as judges he would not have nominated.[289] [290] [291]
* The day after the Supreme Court ruling was issued, 13 Democrats in the U.S. Senate and 57 in the House of Representatives introduced legislation that would overturn the ban on partial-birth abortions.[292] [293] [294] [295] In 2007, Barack Obama stated that the “first thing” he would do as President is sign this bill into law.[296] In 2009, he stated that this bill “is not my highest legislative priority.”[297]
* During the debates over partial-birth abortion in the 1990s:
* After the facts above were revealed, the New York Times reported in 2003 that “one aspect” of the partial-birth abortion debate “has changed”:
* Nine years later, the New York Times editorial board claimed without evidence that abortions after 20 weeks “mostly often involve severely troubled pregnancies that pose risks to a woman’s health or life.”[315]
* Since then, the following have claimed or reported without evidence that late-term abortions are mostly or only done for severe medical reasons:
* During the debates over partial-birth abortion in the 1990s:
* In 2000, two registered nurses who worked in the maternity unit of an Illinois hospital testified before a U.S. Congressional subcommittee that they personally witnessed babies who were born alive after an abortion and left to die without any care or comfort provided.[339] [340] A spokesman for the hospital’s parent corporation estimated that 10% to 20% of the abortions it performs for genetic reasons result in live births for short periods of time.[341]
* A study published by the British Journal of Obstetrics and Gynaecology in 2007 found that 3.2% of abortions done based on diagnoses for conditions like Down’s Syndrome, heart defects, and kidney problems, resulted in live births. These infants lived for a median time of 80 minutes after birth, 36% of them for an hour or less, and 6% for six hours or more.[342]
* A study conducted in Denmark’s second largest maternity clinic from 2011 to 2012 found that 16% of abortions performed between 12 and 22 weeks resulted in live births.[343]
* In 2016, the U.S. Centers for Disease Control and Prevention reported that at least 143 live births after abortions were recorded on death certificates in the U.S. from 2003 to 2014. Among these infants:
* The Encyclopedia of Human Biology states:
* In 2002, a child was born in Britain at 24 weeks gestation following three abortion procedures. As of 2005, he was healthy and was the “first long-term abortion survivor” to be born this prematurely.[346] [347]
* In 2007, twin brothers Ieuan and Gabriel Jones were born at 31 weeks gestation. Eleven weeks before this, doctors discovered that Gabriel was underweight and his heart was three times the normal size. They thought he would die and suggested an abortion to protect the life of his twin. During the abortion, the doctors attempted to sever his umbilical cord but were unable to cut through it. Subsequently, they cut the mother’s placenta in half to isolate the twins from one another. The boys were delivered via caesarian section, and as of November 2007, were seven months old and both healthy.[348] (Click for photos.)
* In 2007, Finly Crampton was born three weeks prematurely after an attempted abortion at eight weeks. His mother previously gave birth to two boys with kidney disorders, one of whom died after 20 minutes, and another who was born with one kidney. She was on the birth control pill when she became pregnant and decided to abort because she “couldn’t cope with the anguish of losing another baby.” At 19 weeks, she discovered the abortion was not successful and decided to carry to term. As of June 2008, Finley was 6 months old, had “minor kidney damage,” and was “expected to lead a normal life.”[349] (Click for photo.)
* Gianna Jessen was born in 1977 after surviving an abortion at seven-and-a-half months gestation. She has cerebral palsy as a result of the procedure but has run marathons and traveled “the world to campaign against abortion.”[350] [351] [352] [353]

* In 2002, the U.S. House of Representatives passed by a voice vote, the U.S. Senate passed by unanimous consent, and President Bush signed a bill stating that anyone “born alive at any stage of development” is considered a “person” under federal law including those born as a result of “abortion.” This law does not specify penalties for breaking it and does not require medical treatment for children who are born alive after an abortion.[354] [355] [356]
* In 2019, Republican Congresswoman Ann Wagner of Michigan and Republican Senator Ben Sasse of Nebraska introduced identical bills in the House and Senate that would:
* In February 2019, the Senate voted 53–44 in favor of this bill, with 94% of Republicans voting for it and 93% of Democrats voting against it. However, the bill did not pass because it was blocked by a filibuster conducted by 42 Democrats and 2 Independents, including Cory Booker (NJ), Kamala Harris (CA), Kirsten Gillibrand (NY), and Bernie Sanders (VT).[359]
* As of October 2023:
* In 2001 and 2002, lawmakers introduced two identical bills in the Illinois legislature with three paragraphs of operative text stating that anyone “born alive at any stage of development” is considered a “person” under Illinois state law including those born as a result of “abortion.”[363] [364] Barack Obama, as an Illinois state senator, voted against both of these bills.[365] [366]
* In 2002, the U.S. House of Representatives passed by a voice vote, the U.S. Senate passed by unanimous consent, and President Bush signed a bill stating that anyone “born alive at any stage of development” is considered a “person” under federal law including those born as a result of “abortion.”[367] [368] [369] This bill contained the same operative language as the Illinois bill except for the following paragraph.
Federal bill:
Illinois Bill:
* At a debate in 2004, Barack Obama was criticized for voting against the Illinois bills and replied:
* In 2003, an amendment was proposed to an Illinois bill to make the operative language the same as the federal bill that Obama said he would have voted for.[371] [372] The amendment was referred to a committee chaired by Obama, where it was unanimously passed. The bill was then voted down by Obama and five other Democrats on the committee.[373] [374] [375] [376]
* In 2020, Republican President Donald Trump issued an executive order to provide protection to “every infant born alive, no matter the circumstances of his or her birth.” The order directed the Secretary of Health and Human services to ensure that federally funded hospitals provide the appropriate:
* As of September 1, 2023:
* In the state of:
* In Washington, California, New Jersey, and Connecticut, it is legal for a girl of any age to get an abortion without her parent’s consent or knowledge.[388]
* In briefs submitted to the United States Supreme Court regarding a Minnesota parental consent law,[389] the American Psychological Association asserted that the law should be struck down because:
* In a brief submitted to the United States Supreme Court regarding a death penalty sentence in Missouri for a person who committed a capital murder at the age of 17,[393] the American Psychological Association asserted that crimes committed by minors should never be subject to the death penalty because:
* Five Gallup polls conducted from 1992 through 2011 found that 69% to 74% of Americans favor “a law requiring women under 18 to get parental consent for any abortion.” Opposition to this view ranged from 23% to 28%.[395]
* A 2005 CBS poll found 80% support for requiring that “at least one parent be told before a girl under 18 years of age could have an abortion.” Opposition to this view was 17%.[396]
* A 2009 Pew poll found 76% support for “requiring that women under the age of 18 get the consent of at least one parent before they are allowed to have an abortion.” Opposition to this view was 19%.[397]
* The 2020 Democratic Party Platform makes no explicit reference to parental consent or notification laws.[398]
* The Republicans did not adopt a new platform in 2020.[399] The 2016 Republican Party Platform supports parental consent and notification laws.[400]
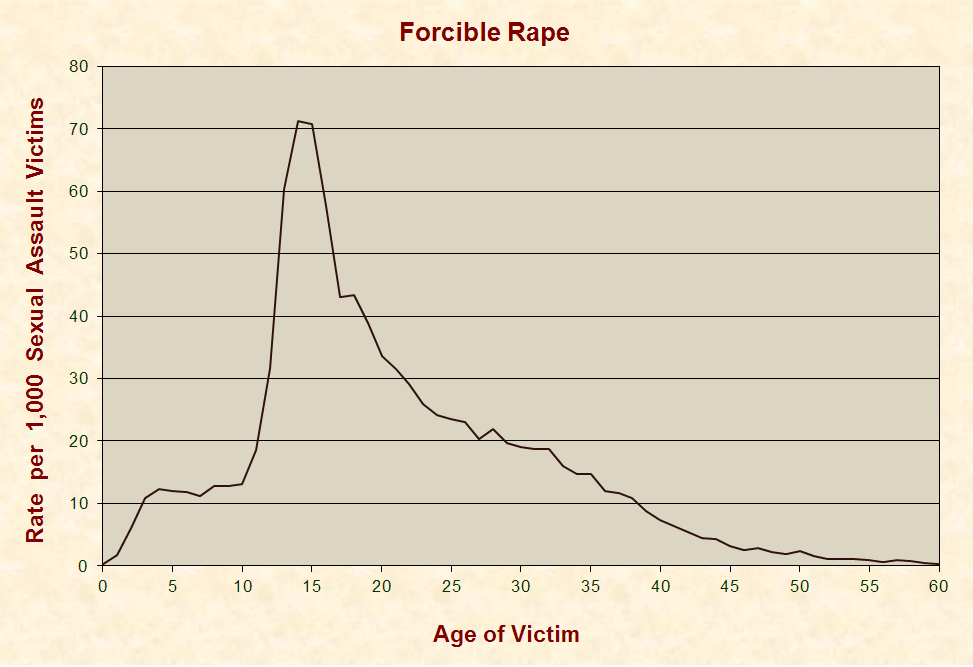
* A 2000 U.S. Department of Justice study of crimes reported to law enforcement in 12 states from 1991 to 1996 found that the incidence of forcible rape peaked at the ages of 14 and 15 years old:
* A scientific survey of U.S. women aged 18–22 conducted in 1987 found that 74% of them who had intercourse before the age of 14 had been forced to have sex against their will at least once. For those who had sex before the age of:
* A scientific survey of U.S. women aged 18 and older conducted in 1995–1996 found that about 54% of female forcible rape victims were raped before the age of 18.[406] [407]
* A scientific survey of U.S. women aged 18 and older conducted in 2011 by the U.S. Centers for Disease Control and Prevention found that about 40% of female rape victims were raped before the age of 18.[408] [409]
* Since 2005, Arkansas law has required written consent from a parent (not a step-parent) before an abortion is performed upon a female who is less than 18 years of age.[410] [411] [412] In 2006, a 15-year-old Arkansas girl accused her 41-year-old stepfather of raping her, getting her pregnant, forcing her to have an abortion in Illinois (where there was no parental consent or notification law in effect at the time), and continuing to rape her afterwards.[413] [414] [415] [416]
* The girl’s claim that she was taken to an abortion clinic in Granite City, Illinois was corroborated by a photo of her stepfather’s car at this facility.[417] He was arrested, was facing a dozen counts of rape, and committed suicide before trial.[418] [419]
* In 2006, the U.S. House of Representatives passed a bill that would have made it illegal to take a child across state lines to perform an abortion without her parent’s knowledge or consent. The bill:
* In 2002, a sexual relationship between a 22-year-old man and a 13-year-old girl was illegal in all 50 states and the District of Columbia.[423] All states had laws that required healthcare and other workers who interacted with children in a professional capacity to report suspected cases of child abuse, which in 29 states and the District of Columbia, explicitly included a sexual relationship between a 22-year-old man and a 13-year-old girl.[424]
* In 2002, Life Dynamics, an organization dedicated to ending legal abortion,[425] phoned more than 800 Planned Parenthood and National Abortion Federation abortion clinics and offices. In these calls, a woman from Life Dynamics told workers at these facilities that she was 13 years old, had been impregnated by her 22-year-old boyfriend, and wanted to get an abortion to hide the situation from her parents.[426]
* In more than 90% of the phone calls, the Planned Parenthood and National Abortion Federation workers did not act to report the matter.[427]
* Some of these clinic workers encouraged the caller to come in for the abortion and lie about the age of the person who impregnated her.[428]
* Some of the workers told the caller that they were required to report the situation but weren’t going to do so.[429]
* In states that have parental notification laws, some workers told the caller to find a person who was old enough to impersonate one of her parents and have them sign the required paperwork. In one state that requires a notarized signature from a parent, a worker told the caller that the facility had a notary public who would notarize a fraudulent signature for her.[430]
* After Life Dynamics released the recordings, Planned Parenthood issued the following statement:
* A Connecticut TV station (WTIC – Fox 61) scrutinized the recordings of the phone calls to the abortion clinics in Connecticut and found that:
* To argue against laws that require parental consent for abortions, people have cited the death of a girl named Becky Bell in venues like:
* On September 16, 1988, 17-year-old Rebecca Suzanne Bell of Indianapolis, Indiana was admitted to a hospital with pneumonia and suffered a fatal cardiopulmonary arrest that night.[446]
* During Becky’s autopsy, “evidence of recent pregnancy with recent partial abortion” was discovered. The “cause of death” listed on the autopsy report is “Septic Abortion with Pneumonia,” and the “manner of death” is listed as “Undetermined.”[447]
* Per Merriam-Webster’s Medical Dictionary, a “septic abortion” is a “spontaneous or induced abortion associated with bacterial infection” and pneumonia is “a disease of the lungs … that is caused especially by infection.”[448] [449]
* Indiana had a parental consent law in effect at the time of Becky’s death (and still does).[450] [451]
* According to a receipt from a local Planned Parenthood and the testimony of Becky’s friend Heather Clark, the two of them visited a Planned Parenthood office in Indiana, and a worker suggested that Becky travel 100 miles to Kentucky to circumvent the Indiana law.[452] [453]
* Heather stated that Becky chose not to tell her parents about the pregnancy because she was recently hospitalized with a drug problem and thought that they would kick her out of the house if they knew she was pregnant.[454] [455] Heather also stated that after she and Becky went to Planned Parenthood, Becky wavered about having an abortion and considered running away and putting the baby up for adoption.[456] [457]
* After Becky’s death, Dennis Nicholas—a county coroner who did not perform the autopsy—told Becky’s parents that:
* These claims led Becky’s parents to blame her death on Indiana’s parental consent law and embark on a speaking tour of 23 states with an advocacy group to lobby against parental involvement laws.[462] [463] [464] [465] When a parental notification law was put on the ballot in Oregon in 1990, polls found opposition to it at 22%. After Becky’s parents toured the state appearing at rallies and on television and talk shows, the measure was defeated with 52% voting against it.[466]
* While Becky’s parents were traveling the nation and receiving coverage from major media outlets,[467] [468] James A. Miller, the research director of an organization with a mission to “promote and defend the sanctity of life,”[469] [470] corresponded several times with Dr. Jesse Giles, the author of the autopsy report and one of two pathologists who signed it.[471] In a press release and a commentary published in the Baltimore Evening Sun, Miller reported that Giles stated:
* In 2008, Just Facts:
* Dr. Pless supervised the autopsy of Becky Bell because Dr. Giles was a fellow in training at the time.[479] A 1990 newspaper article quoted Pless as stating:
* Becky’s autopsy report contains no mention of an infection in her reproductive system and states that “there are no areas of perforation or pus in or around the uterus.”[481]
* Pless confirmed to Just Facts his view that the infection began in Becky’s reproductive system. As evidence of this, he said that the “same micro-organism” that caused the pneumonia “was cultured in the uterus and the lung.”[482]
* When Just Facts pointed out to Pless that the autopsy report’s list of “Specimens for Culture” does not include the uterus,[483] Pless said his memory may be faulty, but “the only possible source of the infection was the uterus” because there “was no upper airway disease—so the only possibility was spread from the uterus.”[484] [485]
* Just Facts replied that:
* Pless responded:
* The HBO movie about Becky Bell shows her going with a friend to obtain an illegal abortion.[492] [493] None of the primary sources examined by Just Facts contain testimony or documentation of such an event. This includes:
* As documented in the coroner’s report, autopsy report, Becky’s mother’s written account, and the Cleveland Plain Dealer, the following timeline of events occurred in the week prior to Becky’s death:
|
Sunday, 12:45 AM |
Becky comes home from a party and says she thinks someone put cocaine or speed in her drink and feels like she’s “got the flu, like Dad.”[498] [499] |
|
Tuesday |
Becky faints.[500] |
|
Wednesday |
Becky stays home from school and develops a 104 degree fever. Her parents try to take her to the doctor, but Becky resists and they relent.[501] [502] [503] |
|
Thursday PM |
Heather visits Becky, and Becky asks her to schedule an abortion in Kentucky on Saturday.[504] |
|
Friday |
Becky starts bleeding and tells her mom. Becky agrees to go a doctor, who diagnoses her with pneumonia and sends her to the hospital. She arrives there at 4 PM.[505] [506] [507] |
|
Friday PM |
The doctor says to Becky’s family: “We don’t know if we can save the baby.”[508] |
|
Friday, 11:29 PM |
Becky passes on.[509] |
* In 1989, six months after Becky Bell’s death, 16-year-old Erica Kae Richardson of Cheltenham, Maryland was assisted by her aunt in obtaining an abortion without her mother’s consent or knowledge. Erica’s aunt, a registered nurse, first took her to Washington Hospital Center, which would not perform the abortion because the pregnancy was 19 weeks along. She then took her to the Metropolitan Women’s Center in Laurel, where Dr. Gene Crawford carried out the abortion, puncturing her uterus in the process. Erica died several hours later from “rupture of [her] lower uterus and cervix with complications, including hemorrhage into the pelvic cavity surrounding the uterus and air embolism.”[510] [511] [512] [513]
* A 2023 Google search for the abortion-caused death of Erica Kae Richardson produced no results from any major media outlet or any of the other sources that covered the death of Becky Bell.[514]
* The current Maryland notification law allows abortion providers to bypass notifying a parent if, in their opinion, the minor is “capable of giving informed consent to an abortion.” The law also stipulates that abortion providers cannot be prosecuted or sued for failing to notify a girl’s parents.[515]
* In 1996, Barack Obama’s Illinois Senate campaign completed a candidate questionnaire and then resubmitted it with amended answers on the following day. In response to the question, “Do you support parental consent/notification for minors seeking abortions?” the answers were:
* When these questionnaires were published by Politico.com during the 2008 presidential race, Obama’s campaign asserted that a staffer filled them out and that some of the responses did not reflect Obama’s views.[518] [519]
* An investigation by Politico found that one of the questionnaires contains written notes that appear to be in Obama’s hand, and the other questionnaire has a cover sheet indicating that Obama supplied the answers in a face-to-face interview at the house of a board member of the organization that issued the questionnaire. The board member has confirmed that Obama personally sat for this interview. In response to these revelations, Obama’s presidential campaign wrote:
* On a 2001 vote in the Illinois Senate for a parental notification bill, Barack Obama voted “Present.”[523] [524]
* Illinois Senate rules state that “a majority of those elected” (30 Senators) must vote in favor of a bill for it to pass. Thus, a vote of “Present” has the same result as a vote of “No.”[525]
* With regard to Obama voting “Present” on this and other abortion-related bills, Pam Sutherland, the president and CEO of the Illinois Planned Parenthood Council stated:
* In response to a 2004 candidate questionnaire that asked, “Do you support parental … notification or consent to obtain an abortion?” Barack Obama’s U.S. Senate campaign answered:
* The 2001 parental notification bill on which Obama voted “Present” had bypass provisions for “sexual abuse,” “neglect,” “physical abuse,” and cases where notification “would not be in the best interests of the minor.”[529] [530]
* In response to a 2007 candidate questionnaire asking if minors should “be required to seek their parents’ ” consent before having an abortion, Barack Obama’s presidential campaign did not explicitly answer the question and stated that:
* As of 2008, all of the 35 states with a parental consent or notification law in effect had a bypass provision that permits exceptions in various circumstances such as when notifying a parent not be in a “minor’s best interests.” This was also the case with a Congressional bill that Obama filibustered. Six of the seven states with a parental consent or notification law blocked by a court order or ruling have similar bypass provisions. The one exception was New Mexico, which has a 1969 law on its books that the state attorney general ruled unenforceable in 1990.[532] [533] [534] [535]
* In 1970, a pregnant woman named Norma McCorvey sued the state of Texas to challenge the constitutionality of a state law that prohibited abortion except to save the life of the mother. McCorvey wanted to keep her identity secret and assumed the fictitious name Jane Roe. The name of the Dallas County district attorney responsible for enforcing the law was Henry Wade. Thus, the case was entitled Roe v. Wade.[536] [537] [538]
* Before the United States Supreme Court, the attorney for Roe argued that the Texas law was unconstitutional because it violated the Ninth and Fourteenth Amendments.[539] The Ninth Amendment reads:
* The clause of the Fourteenth Amendment relevant to the argument reads:
* In support of this view, the attorney for Roe stated that “liberty to these women would mean liberty from being forced to continue the unwanted pregnancy.”[542]
* During oral arguments, one of the judges asked the attorney for Roe if her case was dependent on the assertion that pre-birth humans have no constitutional rights. The attorney for Roe responded:
* After some back and forth, another judge said to Roe’s attorney:
* The attorney for Roe responded:
* At this point, the Chief Justice cut her off and started to ask another question. He then interrupted himself and asked:
* The attorney for Roe stated:
* The attorney for the State of Texas argued that pre-birth humans are protected under the Fifth Amendment.[548] The portion relevant to the argument states:
* During oral arguments, one of the judges contested this viewpoint by asserting that the Fourteenth Amendment defined what the term “person” meant, and that it did not include pre-birth humans.[550] The relevant clause reads:
* After some back and forth, the judge retreated from this position and said:
* The attorney for the State of Texas responded that the only way to understand what the Constitution means by the word “person” was to go to “the teachings at the time the Constitution was framed.” He then quoted from William Blackstone, who is described in Simon & Shuster’s New Millennium Encyclopedia as a “British jurist and legal scholar, whose work Commentaries on the Laws of England was used for more than a century as the foundation of all legal education in Great Britain and the U.S.”[553] [554] [555] In this work, Blackstone wrote that life is a “right” that:
* To further support his position, the attorney for the state of Texas appealed to the Declaration of Independence and started to quote the following sentence from it, but he was cut off by one of judges:[559]
* On January 22, 1973, the Supreme Court released its ruling. Seven of the judges ruled in favor of Roe and two of the judges opposed the ruling. The ruling overturned the laws of 30 states that generally prohibited abortion except to save the life of the mother.[562] Six of the seven justices appointed by Republicans and one of the two justices appointed by Democrats ruled in favor of Roe.[563]
* The majority ruled these laws unconstitutional on the basis that they violated the Fourteenth Amendment, stating that it protects “the right to privacy,” and that this includes “a woman’s qualified right to terminate her pregnancy.”[564] The relevant portion of the Fourteenth Amendment reads:
* The Fourteenth Amendment does not contain the word “privacy” or any synonym for it.[566] [567] It was adopted in 1868 to address a number of issues relevant to the Civil War, such as ensuring constitutional rights for black people.[568] [569] [570]
* The majority wrote that they were “not in a position to speculate” as to “when life begins” and criticized the State of Texas for “adopting one theory of life,” namely, that life begins at conception.[571]
* The majority also:
* After listing these examples and others, the majority wrote that this portion of their ruling does not permit abortions “at whatever time, in whatever way, and for whatever reason” a woman chooses.[581] They repeated this assertion four times using varying words but listed no example of a circumstance where abortion could be prohibited.[582]
* In the 2022 ruling of Dobbs v. Jackson Women’s Health, the Supreme Court overturned Roe v. Wade and Planned Parenthood v. Casey.
* On the same day that the Supreme Court released Roe v. Wade, it issued another ruling in a case entitled Doe v. Bolton. The same seven judges who ruled in favor of Roe also ruled in favor of Doe, and the same two judges opposed the ruling.[583] The majority wrote that this ruling and Roe v. Wade “are to be read together.”[584]
* In this case, the State of Georgia had a law prohibiting abortions unless the pregnancy would “seriously and permanently” injure the health of the mother.[585] A lower court struck down this law and the majority of the Supreme Court agreed. The ruling stated that abortion laws with exceptions for the health of the mother must allow for factors such as emotional health, psychological health, familial concerns, and the woman’s age.[586]
* The Georgia law also required that the doctor who would perform the abortion, two other doctors, and a committee of the medical staff at the hospital where the abortion was to be done needed to agree that the abortion was necessary to preserve the health of the mother.[587] The lower court upheld this law and the Supreme Court struck it down. The majority ruled that only the doctor who would perform the abortion needs to determine that the abortion is necessary to preserve the health of the mother. Any abortion provider could make this decision based solely on their “best clinical judgment.”[588]
* Dr. Warren Hern is a late-term abortion practitioner, author of “the nation’s most widely used textbook on abortion standards and procedures,” a participant in crafting “the first version of the National Abortion Federation Program Standards for Abortion Services,” and “one of the experts in late abortion sought out by the national media….”[589] [590] In 1997, he stated:
* In 1992, the Supreme Court decided a case entitled Planned Parenthood v. Casey. In this case, the majority reaffirmed the central element of Roe v. Wade but did away with the “rigid trimester framework.”[593]
* As in Roe v. Wade, the majority ruled that states cannot prohibit abortions prior to viability, and laws that prohibit abortion after viability must include an exception for the “health of the mother.”[594] (With regard to viability, as of 2020, the youngest premature baby to survive was born at 19 weeks after fertilization, or 21 weeks post-last menstrual period.[595] [596] [597])
* Contrary to Roe v. Wade, the majority ruled that states could enact laws that regulated abortion throughout pregnancy, as long as they did not create a substantial obstacle to obtaining an abortion. An example of what would be acceptable is a law requiring that doctors provide women with certain information before they perform abortions.[598]
* In the 2022 ruling of Dobbs v. Jackson Women’s Health, the Supreme Court overturned Roe v. Wade and Planned Parenthood v. Casey.
* Defying prior U.S. Supreme Court rulings in Roe v. Wade and Planned Parenthood v. Casey, the State of Mississippi passed a law in 2018 which banned abortions after 15 weeks except “in a medical emergency or in the case of a severe fetal abnormality.”[599]
* After the Mississippi law was enacted:
* During the Supreme Court hearings, Mississippi Solicitor General Scott G. Stewart stated that Mississippi has an interest in preventing “the purposeful termination of a human life,” but Justice Sonia Sotomayor challenged him and declared:[602]
* The sciences of genetics, microbiology, and embryology show that the four defining characteristics of life are present during or soon after fertilization:[604]
* Clinical literature documents that every new human life begins at fertilization:
* On June 24, 2022, the Supreme Court released its decision in Dobbs v. Jackson Women’s Health, addressing the “critical question” of “whether the Constitution, properly understood, confers a right to obtain an abortion.”[617]
* Six of the nine justices ruled that the Mississippi law does not violate the Constitution, with three justices dissenting. Five justices also ruled to overturn the prior Supreme Court rulings in both Roe and Casey.[618]
* The five-justice majority held that the Constitution “does not confer a right to abortion” and returned the “authority to regulate abortion” back to the individual states. Their ruling states that Roe and Casey were an “error that cannot be allowed to stand” because:[619]
* Summarizing the facts above, the majority concluded that Casey “perpetuated” Roe’s “egregious” errors, and hence, neither ruling should be viewed as binding precedent.[631]
* In 2023, Democratic Congresswoman Judy Chu of California and Democratic Senator Tammy Baldwin of Wisconsin introduced bills in the House and Senate that would:[632] [633]
* As of October 2023, the House bill is cosponsored by 212 Democrats and 0 Republicans. The Senate bill is cosponsored by 45 Democrats, 3 Independents who caucus with the Democrats, and 0 Republicans.[642] [643] [644]
* In 2022, Republican Senator Lindsey Graham of South Carolina introduced legislation that would criminalize abortions after 15 weeks, except for those “necessary to save the life” of the mother, or in pregnancies that resulted from rape or incest.[645] The bill was cosponsored by 9 Republicans and 0 Democrats.[646]
* In 2019, Republican Congresswoman Ann Wagner of Michigan and Republican Senator Ben Sasse of Nebraska introduced identical bills in the House and Senate that would:
* In February 2019, the Senate voted 53–44 in favor of this bill, with 94% of Republicans voting for it and 93% of Democrats voting against it. However, the bill did not pass because it was blocked by a filibuster conducted by 42 Democrats and 2 Independents, including Cory Booker (NJ), Kamala Harris (CA), Kirsten Gillibrand (NY), and Bernie Sanders (VT).[649]
* As of October 2023:
* The Democratic Party platform states that abortion should be generally legal and supports the use of taxpayer funding to perform abortions. The platform also states that the Democratic Party:
* The Republicans did not adopt a new platform in 2020.[654]
* The 2016 Republican Party platform states that abortion should be generally illegal and supports a Constitutional Amendment that would assure pre-birth humans the right to life. It opposes “the use of public funds to perform or promote abortion” and states:
* The Libertarian Party platform does not mention abortion.[656] [657]
* The Green Party platform states that abortion should be legal and “available on demand.” It also supports using taxpayer funding to perform abortions.[658]
* The Fourteenth Amendment to the U.S. Constitution states:
* Since 1989, several Democrats including Jim Oberstar of Minnesota have sponsored at least 12 resolutions proposing a Constitutional Amendment that would guarantee pre-birth humans the right to life, all of them containing an exception to protect the life of the mother.[660]
* Since 1989, several Republicans including Ann Emerson of Missouri have sponsored at least 22 resolutions proposing a Constitutional Amendment that would guarantee pre-birth humans the right to life, all of them containing an exception to protect the life of the mother. Six of these resolutions also include exceptions for cases of rape and incest.[661]
* In the 2020 U.S. presidential race, the National Right to Life Political Action Committee endorsed Donald Trump for President and stated that Joe Biden “wants abortion at any time, anywhere, and under any circumstances.”[662] [663]
* In the 2020 U.S. presidential race, the Political Action Committee of Reproductive Freedom for All (formerly NARAL Pro-Choice America[664]) endorsed Joe Biden for President and stated that his commitment to “expand access to abortion” was “critical given the threat Donald Trump poses to our fundamental rights….”[665]
* The President of the United States appoints judges to the Supreme Court. These appointments must be approved by a majority of the Senate.[666]
* Once seated, federal judges serve for life unless they voluntarily resign or are removed through impeachment, which requires a majority vote of the House of Representatives and two-thirds of the Senate.[667]
* For more implications relating to the appointment and approval of judges, see the section on Constitution & Law.
* From at least 1973 through 2018, Democrat Joe Biden opposed federal taxpayer funding for abortions.[668] [669] [670] [671] In a 1994 letter to a constituent, he wrote:
* In 2019 while pursuing the Democratic Party’s nomination to be president of the United States, Biden changed his position on taxpayer funding for abortions with the following statements:
* Biden’s 2020 presidential campaign website stated that “Biden will work to codify Roe v. Wade, and his Justice Department will do everything in its power to stop the rash of state laws that so blatantly violate Roe v. Wade.”[678]
* Under the Supreme Court’s 1973 ruling in Roe v. Wade:
* Biden’s 2020 presidential campaign website stated that he will overturn state laws that require parental notification before a minor can have an abortion.[684]
* As a U.S. Senator, Biden participated in a filibuster to block a bill that would have made it illegal to take a child across state lines to perform an abortion without her parent’s knowledge or consent.[685] The bill:
* In 2021, President Biden revoked the “Mexico City Policy,” which directed the Secretary of State “to ensure that U.S. taxpayer dollars do not fund organizations or programs that support or participate in the management of a program of coercive abortion or involuntary sterilization.”[688] [689] This was originally a Reagan policy that Trump reinstated in 2017.[690]
* Click here for an article by Just Facts about how five prominent “fact checkers” have falsely claimed that Joe Biden and Kamala Harris don’t support legalizing abortion up to birth.
* In 1999, during an interview announcing he would be leaving the Republican Party for the Reform Party, Donald Trump stated on NBC’s Meet the Press, “I am very pro-choice.”[691]
* In his 2000 book, The America We Deserve, Trump wrote that he “would support a ban” on partial birth abortion.[692]
* In 2011, speaking before the Conservative Political Action Conference, Trump stated, “I’m pro-life.”[693]
* During a 2015 Republican Party primary debate, moderator Megyn Kelly asked Trump about his change of position, and he replied: “I’ve evolved on many issues over the years. … I am very, very proud to say that I am pro-life.”[694]
* In 2015, Chuck Todd of NBC’s Meet the Press questioned Trump on abortion:
* In 2016, Chris Matthews of MSNBC asked Trump if there should be a punishment for women who have an abortion. He replied, “The answer is that there has to be some form of punishment. … I have not determined what the punishment would be.”[696] Later on the same day, Trump clarified that “the doctor or any other person performing this illegal act upon a woman would be held legally responsible, not the woman.”[697]
* During the final 2016 U.S. Presidential debate, moderator Chris Wallace asked Trump if he would like “to see the court overturn Roe v. Wade.” Trump replied that overturning Roe v. Wade will “happen automatically, in my opinion, because I am putting pro-life justices on the court.”[698] Following the election, Trump said that if Roe v. Wade “ever were overturned, it would go back to the states.”[699]
* In 2017, Trump reinstated Ronald Reagan’s “Mexico City Policy.” This policy directs the Secretary of State “to ensure that U.S. taxpayer dollars do not fund organizations or programs that support or participate in the management of a program of coercive abortion or involuntary sterilization.”[700] [701]
* In 2020, Trump issued an executive order that granted protection to “every infant born alive, no matter the circumstances of his or her birth.” The order directed the Secretary of Health and Human services to ensure that federally funded hospitals provide the appropriate:
* In 2020, Donald Trump appointed Amy Coney Barrett to the U.S. Supreme Court.[703] Four years earlier, when she was asked about the future of abortion laws, she stated:
* During her confirmation hearing in 2020, Barrett was asked if she believed Roe v. Wade is a “super precedent,” and she replied:
* In 2019, Kamala Harris and 42 other Democrats in the U.S. Senate sponsored the “Women’s Health Protection Act.”[706] If enacted, this law:
* The Supreme Court’s rulings in Roe v. Wade, Doe v. Bolton, and Planned Parenthood v. Casey defined the “health of the mother” to include factors like the “stigma of unwed motherhood,” the work of “child care,” and “the distress, for all concerned, associated with the unwanted child.”[710] [711] [712]
* When asked in 2019 “if there was a point at which” abortion “would be considered immoral,” Harris did not identify one.[713]
* In 2019, Harris was among a group of Democrats who blocked a bill that would have criminalized failure to care for children born alive after an abortion.[714] [715]
* Harris’ 2020 presidential campaign website stated that she “will require, for the first time, that states and localities with a history of violating Roe v. Wade obtain approval from her Department of Justice before any abortion law or practice can take effect.”[716]
* Click here for an article by Just Facts about how five prominent “fact checkers” have falsely claimed that Joe Biden and Kamala Harris don’t support legalizing abortion up to birth.
* While Mike Pence was a U.S. congressman, he:
* As the governor of Indiana and as a U.S. congressman, Pence sponsored, cosponsored, and signed numerous other acts to limit abortion and its consequences.[730] [731] [732] [733] [734] [735] [736] [737] [738] [739] [740] [741] [742] [743] [744] [745] [746] [747] [748] [749] [750] [751] [752]
* In 2019, Democratic Senator Elizabeth Warren called on Congress to pass federal legislation that would:
* In 2019, Warren was among a group of Democrats who blocked a bill that would have criminalized failure to care for children born alive after an abortion.[761] [762]
* As a U.S. congressman, Bernie Sanders, an independent who caucuses with Democrats,[763] voted on at least three occasions against banning partial-birth abortions.[764] [765] [766]
* In 2007, Sanders, who was by then a U.S. Senator, co-sponsored the Freedom of Choice Act.[767] This would have invalidated all federal, state, and local laws that interfere with abortion.[768]
* In 2007, Sanders voted against a bill to prevent taxpayer funding of foreign “organizations with ties to coercive abortions and forced sterilizations.”[769] [770]
* In 2019, Sanders joined a group of Democrats in blocking a bill that would have criminalized failure to care for children born alive after an abortion.[771] [772]
* In 2019, when asked “Do you believe there should be any restrictions on abortion in law?” Sanders did not identify any.[773]
* At a Democratic Candidates “Compassion Forum” held in 2008, Barack Obama was asked, “Do you personally believe that life begins at conception, and if not, when does it begin?” Obama replied in part:
* Four months later in an interview, Obama was asked, “At what point does a baby get human rights?” He responded in part:
* Barack Obama has voiced support for Roe v. Wade and stated that this would be reflected in his appointments to the Supreme Court.[776] [777] He has also stated that he supports a ban on late-term abortions but only with an exception for the “health” of the mother.[778]
* In a 2008 interview, Obama was asked to clarify his position on late-term abortions, and he stated:
* Four days later, a reporter asked for clarification of these remarks, and Obama responded that late-term abortion bans must have an exception for “serious clinical mental health diseases,” but this does not mean that “if a woman just doesn’t feel good then that is an exception. That’s never been the case.” He also stated:
* The Roe v. Wade verdict provided several examples of what may constitute a risk the health of the mother. These included the “stigma of unwed motherhood” and “the distress, for all concerned, associated with the unwanted child.” Roe v. Wade and Doe v. Bolton, which were issued by the Supreme Court on the same day with the order that they “are to be read together,” mandated that abortion be legal up until the point of birth if any one physician willing to perform an abortion says it is necessary to preserve a mother’s health.[781] [782]
* Speaking before a Planned Parenthood national conference in 2007, Obama stated: “I put Roe at the center of my lesson plan on reproductive freedom when I taught Constitutional Law. … On this fundamental issue, I will not yield and Planned Parenthood will not yield.”[783] [784] When asked what he would do to “ensure access to abortion” and make certain his judicial nominees are “true to the core tenets of Roe v. Wade,” he stated:
* The Freedom of Choice Act was introduced in the U.S. Senate in 2007 by 13 Democrats including Barbara Boxer (California), Frank Lautenberg (New Jersey) and Max Baucus (Montana).[786] [787] One month later, Barack Obama signed on as a cosponsor.[788] Its stated objective is to “protect, consistent with Roe v. Wade, a woman’s freedom to choose to bear a child or terminate a pregnancy….” It would invalidate “every Federal, State, and local statute, ordinance, regulation, administrative order, decision, policy, practice” that interferes with the termination of any “pregnancy prior to viability” and any pregnancy “after viability where termination is necessary to protect the life or health of the woman.”[789]
* On the same day this bill was introduced in the Senate, a bill with the same name and parallel verbiage was introduced in the House of Representatives.[790] It gained 109 sponsors (108 Democrats and one Republican) but was not voted upon.[791] [792] [793] The Senate bill gained 20 sponsors (19 Democrats and one Independent) but was not voted upon.[794] [795]
* In 2008, Howard Dean, the chairman of the Democratic National Committee, stated that the Democratic Party “believes that we ought to significantly reduce the number of abortions in this country.” A reporter asked Dean how he could reconcile this assertion with the party’s support for taxpayer funding of abortions. Dean replied it is “total nonsense” that public funding of abortions increases the abortion rate.[796]
* According to the Guttmacher Institute, an organization whose “Guiding Principles” include support for legalized abortion:[797]
* The American Civil Liberties Union (ACLU) supports the use of taxpayer funding to perform abortions. In making its case for this position, the ACLU poses the following rhetorical question:
And answers:
* The ACLU is opposed to taxpayer funded school choice programs. One of its arguments for this stance is:
* In 2001, the Society of Professional Journalists, “the nation’s most broad-based journalism organization,”[801] adopted “diversity guidelines” reaffirming “their commitment” to use “language that is informative and not inflammatory.” These guidelines state that it is “misleading” to use “word combinations” such as “Islamic terrorist” or “Muslim extremist” “because they link whole religions to criminal activity.” The same document states:
* In 2007 at a Republican “Unity Dinner” in Iowa, John McCain stated:
* At the same event, Mike Huckabee stated:
* In a New York Times article about this event, reporter Adam Nagourney wrote that John McCain and Mike Huckabee “presented themselves as lifelong opponents of abortion rights.” Four times in this article, Nagourney characterized the speakers as opponents of abortion rights and never as supporters of rights for the unborn.[805]
* Over decades, the following major media outlets characterized people as “opponents” of various “rights” as follows:
|
“opponent(s) of … |
Number of Times Phrase Was Used |
||
|
New York Times (1981–2021) |
Washington Post (1987–2021) |
Associated Press (1982–2008) |
|
|
abortion rights”[806] |
280 |
64 |
61 |
|
gun rights”[807] |
2 |
0 |
1 |
|
property rights”[808] |
0 |
0 |
0 |
|
parental rights”[809] |
0 |
0 |
0 |
|
individual rights”[810] |
0 |
0 |
1 |
|
states’ rights”[811] |
0 |
0 |
0 |
|
religious rights”[812] |
0 |
0 |
0 |
* Melloni’s Illustrated Medical Dictionary defines “partial-birth abortion” as a:
* The American Medical Association has adopted a policy that states:
* The American Medical Association’s Manual of Style states:
* On the television show NOW with Bill Moyers, PBS journalist Brenda Breslauer stated:
* The book English for Journalists states that medical literature is a “common source” of jargon and:
* A 2005 house editorial in the Chicago Tribune uses the term “intact dilation and extraction” to identify “certain late-term abortions.” It does not contain the term “partial-birth” and provides no description of the procedure.[819]
* The New York Public Library Writer’s Guide to Style and Usage states:
* Before Roe v. Wade and Planned Parenthood v. Casey were overturned in 2022, they mandated that abortion be legal up until birth if any one physician willing to perform an abortion said it was necessary to preserve a mother’s health.[822] [823] [824]
* In 2002, the Gallup polling organization reported:
* From 2002 until Roe and Casey were overturned:
* Before Roe and Casey were overturned in 2022, they prohibited states from banning abortion up until birth unless the ban contained an exception for the “health of the mother.” Under these rulings, the “health of the mother” included factors like:
* While Roe and Casey were still in effect, the following commentators and media outlets did not convey what “health” actually meant in the context of abortion when:
* In 1987, Republican President Ronald Reagan asked his Surgeon General, Dr. C. Everett Koop, to prepare a “comprehensive report” concerning “the health effects of abortion on women.”[839]
* In 1989, Koop wrote a letter to Reagan stating that he and the staff in several public health agencies reviewed almost 250 studies and found that each had flaws which prevented them from drawing “scientifically sound conclusions.”[840]
* That evening:
* Koop’s letter did not say what Jennings, Rather, or Brokaw reported. Instead, it stated:
* In 1985, the Los Angeles Times polled 3,165 newspaper reporters and editors working at 621 newspapers. It found that approximately 85% were in favor of abortion being generally legal. The same poll found that 51% of the general public were in favor of abortion being generally legal.[842]
* In 2001, Hal Bruno, the former political director of ABC News, was asked what percentage of people at ABC News were “pro-choice.” He replied:
* Below are the results of a Gallup poll conducted 6 months before the interview:
|
Statement |
Women Who Agree |
Men Who Agree |
|
Abortion should be legal under any circumstances |
28% |
23% |
|
Abortion should be legal in most circumstances |
14% |
15% |
|
Abortion should be legal in only a few circumstances |
40% |
43% |
|
Abortion should be illegal in all circumstances |
15% |
16% |
* A Zogby poll conducted about a year before the interview asked people if they agreed with the following statements:
|
Statement |
Women Who Agree |
Men Who Agree |
|
Abortion destroys a human life and is manslaughter |
51% |
51% |
|
Abortion does not destroy a life and is not manslaughter |
33% |
37% |
* In the same interview, Bruno stated:
* Four months prior to the interview, Gallup conducted a poll which found:
[1] Article: “Abortion Poll: Not Clear-Cut; Wording of a Question Makes a Big Difference.” By E.J. Dionne, Jr. New York Times, August 18, 1980. Page A15. <www.nytimes.com>
What do the American people think about abortion? It depends on how you ask them the question. …
Do you think there should be an amendment to the Constitution prohibiting abortions, or shouldn’t there be such an amendment? … Yes [=] 29% … No [=] 67% …
Do you believe there should be an amendment to the constitution protecting the life of the unborn child, or shouldn’t there be such an amendment? Yes [=] 50% … No [=] 39% …
For facts about what constitutes a scientific survey and the factors that affect their accuracy, visit Just Facts’ research on this topic.
[2] Book: The Practice of Statistics (4th edition). By Daren S. Starnes, Daniel S. Yates, and David S. Moore. W. H. Freeman and Company, 2010.
Page 224:
The wording of questions is the most important influence on the answers given to a sample survey. Confusing or leading questions can introduce strong bias, and changes in wording can greatly affect a survey’s outcome. …
Don’t trust the results of a sample survey until you have read the exact questions asked. The amount of nonresponse and the date of the survey are also important. Good statistical design is part, but only a part, of a trustworthy survey.
[3] Article: “Erase the Words, Change the Language and You Can Control the Debate and Rewrite History.” By Evie Loveband. Idiom, 2012. Pages 44–45. <search.informit.com.au>
Abstract:
Language is power; power for influencing society, shifting reality, rewriting history, undermining perspectives and establishing solidarity. One can manipulate language for the purpose of gaining and maintaining authority or employ disguising and distorting expressions to veil the truth. Nonetheless, language too can be utilised as a tool to promote equality, to build allegiance and to endorse unity in our society. With careful selection of and modification to language, any one user has the power to control the debate and rewrite history.
[4] Entry: “child.” Merriam-Webster. Accessed September 9, 2023 at <www.merriam-webster.com>
Definition 3a: “an unborn or recently born person.”
[5] Entry: “fetus.” Black’s Medical Dictionary (41st edition). Scarecrow Press, 2006. Pages 269–270.
Page 269: “The name given to the unborn child after the eighth week of development.”
[6] Entry: “baby.” Merriam-Webster. Accessed September 9, 2023 at <www.merriam-webster.com>
Definition 1a: “an extremely young child; especially: infant.”
[7] Entry: “neonatal intensive care.” Black’s Medical Dictionary (41st edition). Scarecrow Press, 2006.
Page 487: “The provision of a dedicated unit with special facilities, including one-to-one nursing and appropriate technology, for caring for premature and seriously ill newborn babies.”
[8] Entry: “fetus.” Merriam-Webster’s Collegiate Dictionary, Encyclopædia Britannica Ultimate Reference Suite, 2004.
The etymology of this word is: “Middle English, from Latin, act of bearing young, offspring; akin to Latin fetus newly delivered, fruitful—more at feminine.”
[9] Entry: “fetus.” Dorland’s Illustrated Medical Dictionary (29th edition). W. B. Saunders Company, 2000.
Page 661: “the unborn offspring in the postembryonic period, after major structures have been outlined, in humans from nine weeks after fertilization until birth.”
[10] Entry: “fetal.” Dorland’s Illustrated Medical Dictionary (29th edition). W. B. Saunders Company, 2000.
Page 661: “of or pertaining to a fetus; pertaining to in utero development after the embryonic period.”
[11] Textbook: Langman’s Medical Embryology (9th edition). By T. W. Sadler. Lippincott Williams & Wilkins, 2004.
Page 117: “The period from the beginning of the ninth week to birth is known as the fetal period.”
[12] For example, in April of 2001, the U.S. House of Representatives passed the “Unborn Victims of Violence Act.” This bill would have made it a crime for people to harm a “child in utero” except for an abortion done with the consent of the mother. The bill defines a child in utero as “a member of the species homo sapiens, at any stage of development, who is carried in the womb.” In their coverage of this vote, CNN, Reuters, the New York Times, the Washington Post, ABC, USA Today, MSNBC, and CBS all used the word “fetus” or “fetal” as a blanket phrase for humans at any stage prior to birth. As shown by Black’s Medical Dictionary, this term applies only “after the eighth week of development.”
[13] Commentary: “Where’s the Baby? The AP Misses the Point.” By Kathryn Jean Lopez. National Review, March 13, 2002. <www.nationalreview.com>
NOTE: This column criticizes the Associated Press for misapplying the word “fetus” to humans who are born alive after an abortion. As shown by Black’s Medical Dictionary and the Royal College of Obstetricians and Gynaecologists, this term does not apply after birth.
[14] Article: “Obama’s View on Abortion May Divide Catholics.” By John M. Broder. New York Times, August 6, 2008. <www.nytimes.com>
“Republicans are gearing up campaigns to depict Mr. Obama as a radical on the question of abortion, because as a state senator in Illinois he opposed a ban on the killing of fetuses born alive.”
NOTE: As shown by Black’s Medical Dictionary and the Royal College of Obstetricians and Gynaecologists, this term does not apply after birth.
[15] Commentary: “Fetus or Baby?” By Christine Chinlund. Boston Globe, February 17, 2003. <www.boston.com>
“Some pretty impartial sources, from the American College of Obstetricians and Gynecologists to Webster’s Dictionary, say that any unborn child is considered a fetus.”
NOTE: Later in the column, the author quotes the following definition of “fetus” from Webster’s, which does not support the assertion she made: “An unborn offspring, especially in its later stages and specifically in humans, from about the eighth week after conception until birth.” The author did not attempt to substantiate the claim about the American College of Obstetricians and Gynecologists, and Just Facts could find no such information on their website.
[16] Press release: “States May Provide SCHIP [State Children’s Health Insurance Program] Coverage for Prenatal Care.” United States Department of Health and Human Services, September 27, 2002. <wayback.archive-it.org>
“The final regulation, which will be published in the Federal Register on Wednesday, October 2, allows states to file a state plan amendment to use existing SCHIP funding for coverage for children from conception to birth and up to age 19.”
NOTE: As the quote above explains, the regulation is applicable from the point of conception onwards, yet the following articles use the word “fetus” to describe the beneficiaries:
[17] Press release: “RCOG [Royal College of Obstetricians and Gynaecologists] Statement on the Article ‘One Baby in 30 Left Alive After Medical Termination’ (London Daily Mail, 20 April 2007).” Royal College of Obstetricians and Gynaecologists, April 20, 2007. <www.rcog.org.uk>
“If the fetus has had a lethal injection, it will normally die. However, there are some instances when there are signs of life at birth. All babies must be treated with dignity and respect. Palliative care should be provided till the baby dies where relevant.”
NOTE: Observe how the Royal College of Obstetricians and Gynaecologists accurately uses the word “baby” after birth.
[18] Book: English for Journalists (2nd edition). By Wynford Hicks. Routledge, 1998.
Page 73: “Jargon is specialized vocabulary, familiar to the members of a group, trade or profession. If you write for a newspaper or general magazine you should try to translate jargon into ordinary English whenever you can. … A common source of jargon is scientific, medical, government and legal handouts.”
[19] Book: Writing for Journalists. By Wynford Hicks, Sally Adams & Harriet Gilbert. Routledge, 1999.
Page 125:
This emphasis on plainness and simplicity has been repeated by those who lay down the law about journalistic style. The Economist Pocket Style Book, first published in the 1980s, quotes George Orwell’s “six elementary rules” from his famous essay, “Politics and the English Language”, written in 1946. … 5. Never use a foreign phrase, a scientific word or a jargon word if you can think of an everyday English equivalent.
[20] Book: The New Oxford Guide to Writing. By Thomas S. Kane. Oxford University Press, 1988.
Page 199: “Jargon is technical language misused. Technical language, the precise diction demanded by any specialized trade or profession, is necessary when experts communicate with one another. It becomes jargon when it is applied outside the limits of technical discourse.”
[21] Book: The New York Public Library Writer’s Guide to Style and Usage. Edited by Andrea J. Sutcliffe. Stonesong Press/Harper Collins, 1994.
Page 586: “When writing for a specialized audience—one familiar with the topic or field—a writer must use jargon; it is the common idiom. When writing for a lay audience or the general public, a writer should use jargon only when necessary and define it carefully. Where plain English serves equally well, it should be used instead.”
[22] Entry: “gravida.” Dorland’s Illustrated Medical Dictionary (29th edition). W.B. Saunders Company, 2000.
Page 770: “a pregnant woman”
[23] For example, the following searches performed on October 2, 2020 yielded thousands of results for “fetus” and one result for “gravida” that refers to a pregnant woman:
|
Organization |
Search Results |
Notes |
||
|
“fetus” |
“abortion” AND “mother” AND “fetus” |
“gravida” |
||
|
7,210 |
1,980 |
7 † |
All available |
|
|
4,010 |
1,550 |
1 ‡ |
All available |
|
|
6,090 |
2,060 |
0 |
All available |
|
|
1,460 |
330 |
1 ‡ |
All available |
|
NOTES:
[24] Article: “A Woman Married a Paroled Murderer. Years Later, He Killed All Her Children.” By Kristine Phillips. Washington Post, March 8, 2017. <www.washingtonpost.com>
“In 1991, Michigan man Gregory Green stabbed his wife in the face and chest, killing her and their unborn child.”
[25] Article: “Parents of Slain Pregnant Woman Forgive Suspect.” By Dan Nephin. Associated Press, July 25, 2008. <usatoday30.usatoday.com>
“The parents of a slain pregnant woman said Friday they have forgiven the suspect charged with killing their daughter and cutting her baby out of the womb.”
[26] Article: “Fetus or Baby?” By Christine Chinlund (Ombudsman). Washington Post, February 17, 2003. Page A13. <www.boston.com>
The Globe was technically correct when it referred to the youngest shooting victim in the Feb. 5 MBTA [Massachusetts Bay Transportation Authority] Orange Line tragedy as a “fetus.” But sometimes you can be technically correct and wrong at the same time. This was one of those times.
The facts: On the night of Feb. 5, Hawa Adama Barry, in the ninth month of pregnancy, was shot in the abdomen during a stand-off between two groups of young men on the T.
Early reports from authorities suggested that the baby died in the womb. Thus, the Globe’s headline the next day read: “Passenger shot, her fetus dies as men clash on T.” Other media outlets had similar accounts but used “unborn baby” rather than “fetus.”
Readers were quick to object to “fetus.” A few echoed the abortion-related debate about when life begins, but most argued that the use of such a clinical word to describe an almost full-term baby made the Globe look silly and insensitive.
“I thought it truly dehumanized the tragic murder, especially for the mother but also for those who have children and recognize that a parent refers to a baby weeks from birth as just that—a baby,” wrote one reader who, with his wife, had suffered lost pregnancies. “This has nothing to do with the abortion debate—though I can hear the ‘prolife’ people now. It has everything to do with the death of a child.”
Kerri Bean from Milton called to say the Globe’s word choice so “horrified” several of her friends that they wanted to cancel the paper. “This is not a matter of being prochoice or not,” she said. “It’s a matter of being a mother.”
Wrote another subscriber: “Those criminals on the train committed murder, not abortion”—and indeed several readers pointed out that police hope to bring murder charges against the shooter. Yet another reader, noting that “Every other news channel, TV, and newspaper called it a baby,” demanded to know how the Globe came to use “fetus.” He added: “I’m sure there’s some sort of angle here.”
[27] Article: “Baby Saved as Heroes Lift Bus Off Crushed Mom.” Associated Press, August 15, 2008. <www.nbcnews.com>
“Dozens of strangers converged from all directions to lift a 5-ton bus off the body of a pregnant woman—a heroic effort that managed to save the life of her child but was too late for her.”
[28] Paper: “Fetal and Maternal Analgesia/Anesthesia for Fetal Procedures.” By Marc Van de Velde and Frederik De Buck. Fetal Diagnosis and Therapy, April 25, 2012. Pages 201–209. <www.karger.com>
Page 201: “At present, the unborn child is increasingly being treated as a patient in its own right.”
[29] Book: Writing for Journalists. By Wynford Hicks, Sally Adams & Harriet Gilbert. Routledge, 1999.
Page 125:
This emphasis on plainness and simplicity has been repeated by those who lay down the law about journalistic style. The Economist Pocket Style Book, first published in the 1980s, quotes George Orwell’s “six elementary rules” from his famous essay, “Politics and the English Language”, written in 1946. … 5. Never use a foreign phrase, a scientific word or a jargon word if you can think of an everyday English equivalent.
[30] Book: Exploring Emergent Brain Dynamics: Prebirth to Adolescence. Edited by April A. Benasich and Urs Ribary. MIT Press, 2018.
Chapter 1: “Exploring Emergent Brain Dynamics.” By April A. Benasich and Urs Ribary. Pages 1–14.
Page 4:
Prior to birth, the brain undergoes a substantive degree of development and many of these early steps lay the foundation for later maturation. Studying the developing brain in human embryos and fetuses is laden with challenges. In his review, Alain Chédotal (Chapter 3) examines the role of axon guidance molecules in the regulation of cell—cell interactions during normative and atypical development. He points out that although various methods exist to study axon guidance in animals, technical and ethical issues pose significant challenges in the developing human. To visualize and track neuronal connectivity successfully in pre-birth humans, Chédotal stresses the need for improved noninvasive imaging methods (e.g., 3D and 4D obstetrical ultrasonography, 3D power Doppler ultrasound, in utero MRI [magnetic resonance imaging], and diffusion tensor imaging tractography) and recommends development of novel methods.
[31] Webpage: “Emergent Brain Dynamics.” MIT Press. Accessed August 28, 2019 at <mitpress.mit.edu>
Summary
Experts explore the maturation of nonlinear brain dynamics from a developmental perspective and consider the relationship of neurodevelopmental disorders to early disruption in dynamic coordination.
This volume in the Strüngmann Forum Reports series explores the complex mechanisms that accompany the dynamic processes by which the brain evolves and matures. Integrating perspectives from multiple disciplines, the book identifies knowledge gaps and proposes innovative ways forward for this emerging area of cross-disciplinary study. The contributors examine maturation of nonlinear brain dynamics across systems from a developmental perspective and relate these organizing networks to the establishment of normative cognition and pathology seen in many neurodevelopmental disorders. …
Endorsement
This volume of edited chapters by many leaders in this important field of study, is the product of one of the remarkable meetings organized by the Ernst Strungmann Forum, based on an in-depth symposium examining and debating the details of the fundamentally important question, ‘how do early experiences influence brain development to determine who we become?’ Much important information is provided by this influential volume, and essential unresolved questions, problems, and concerns are elucidated, making this an important read for experts and for those newly introduced to the issues raised therein.
– Fred H. Gage, Adler Professor, Laboratory of Genetics, Salk Institute for Biological Studies
[32] Textbook: Pediatric Toxicology: Diagnosis and Management of the Poisoned Child. By Timothy B. Erickson and others. McGraw-Hill, 2005.
Page 46: “The categories of human in utero exposure consist of maternal drugs of abuse, maternal environmental exposure, and maternal prescription drug use.”
[33] Textbook: Review of Medical Physiology (22nd edition). By William F. Ganong. McGraw Hill, 2005.
Page 259: “Exposure of human females to androgen in utero does not change the cyclic pattern….”
[34] Textbook: Before We Are Born: Essentials of Embryology and Birth Defects (5th edition). By Keith L. Moore & T.V.N. Persaud. W.B. Saunders Company, 1998.
Page 500: “The zygote and early embryo are living human organisms.”
NOTE: Entry: “organism.” American Heritage Dictionary of Science. Edited by Robert K. Barnhart. Houghton Mifflin, 1986. Page 456: “a living body made up of separate parts, such as ribosomes, vacuoles, cells, tissues, and organs, which work together to carry on the various processes of life”
[35] Textbook: The Developing Human: Clinically Oriented Embryology (7th edition). By Keith L. Moore & T. V. N. Persaud. Saunders, 2003.
Page 2: “Zygote. This cell results from the union of an oocyte and a sperm during fertilization. A zygote is the beginning of a new human being (i.e., an embryo).”
[36] Book: An Atlas of the Human Embryo and Fetus: A Photographic Review of Human Prenatal Development. By Jan E. Jirásek (MD, DSc, Laboratory of Reproductive Embryology, Institute for the Care of Mother and Child, Prague, Czech Republic). Parthenon Publishing Group, 2001.
Page 21: “A human being originates from two living cells: the oocyte (female germ cell) and the spermatozoon (male germ cell), transmitting the torch of life to the next generation.”
[37] Textbook: Human Life Before Birth. By Frank J. Dye. Harwood Academic Publishers, 2000.
[38] Entry: “abortion.” American Heritage Dictionary of Science. Houghton Mifflin, 1986.
Page 2: “a birth that occurs before the embryo or fetus develops enough to live on its own, usually during the first twelve weeks of pregnancy (spontaneous abortion) … SYN: miscarriage.”
Pages ix–xi:
The expert help of the Editorial Committee [of Contributing Scientists] has enabled us to formulate definitions and explanations that correspond to recent findings of scientists working in their various disciplines. Precise editorial review in the offices of the publisher has contributed to a standard of excellence.
This is a dictionary of the basic terms of the physical and the biological sciences. …
The compiling of a specialized dictionary is, perhaps more than in most other reference books, the result of many scholars and editors working together. We are fortunate to have an outstanding group of active scientists, who read, commented upon and corrected the entire manuscript, and we are indented to them for their thorough work.
[39] Textbook: Before We Are Born: Essentials of Embryology and Birth Defects (5th edition). By Keith L. Moore & T.V.N. Persaud. W.B. Saunders Company, 1998.
Page 109: “The expected date of delivery (EDD) of a fetus is 266 days, or 38 weeks, after fertilization; that is, 280 days, or 40 weeks, after LNMP [last normal menstrual period] (Table 7-1).”
[40] Book: Color Atlas of Life Before Birth. By Marjorie A. England. Year Book Medical Publishers, 1983.
Page 12: “Most clinicians do not know the fertilization date; the only date available to them is the first day of the last menstrual period. They use this date to define a menstrual age stretching from time 0, which is usually 14 days before fertilization….”
[41] Book: How Life Begins. By Christopher Vaughn. Random House, 1996.
Page 8: “In other words, most obstetricians figures are based on a forty-week pregnancy when you’re actually pregnant for only thirty-eight weeks.”
[42] Book: Color Atlas of Physiology (5th edition). By Agamemnon Despopoulos & Stefan Silbernagl. Thieme, 2003.
Page 308: “Fertilization usually takes place on the first day after intercourse….”
[43] Textbook: Langman’s Medical Embryology (9th edition). By T. W. Sadler. Lippincott Williams & Wilkins, 2004.
Page 122: “The oocyte is normally fertilized within 12 hours of ovulation. However, sperm deposited in the reproductive tract up to 6 days prior to ovulation can survive to fertilize oocytes. Thus, most pregnancies occur when sexual intercourse occurs within a 6-day period that ends on the day of ovulation.”
[44] Book: Psychological Development and Early Childhood. By John Oates, Clare Wood & Andrew Grayson. Blackwell, 2005.
Page 217: “Genotype: The complete set of genes present in an individual. The genotype is determined at fertilization when genetic information from the egg and sperm is combined.”
[45] Book: Mayo Clinic Guide to a Healthy Pregnancy. By the Mayo Clinic. Collins, 2004.
Page 45 (section on fertilization): “This genetic material will determine your baby’s sex, eye color, hair color, body size, facial features and—at least to some extent—intelligence and personality. … Your baby’s sex is determined at the moment he or she is conceived.”
[46] Entry: “life.” American Heritage Dictionary of Science. Houghton Mifflin, 1986.
Page 359: “the form of existence that organisms like animals and plants have and that inorganic objects or organic dead bodies lack; animate existence, characterized by growth, reproduction, metabolism, and response to stimuli.”
Pages ix–xi:
The expert help of the Editorial Committee [of Contributing Scientists] has enabled us to formulate definitions and explanations that correspond to recent findings of scientists working in their various disciplines. Precise editorial review in the offices of the publisher has contributed to a standard of excellence.
This is a dictionary of the basic terms of the physical and the biological sciences. …
The compiling of a specialized dictionary is, perhaps more than in most other reference books, the result of many scholars and editors working together. We are fortunate to have an outstanding group of active scientists, who read, commented upon and corrected the entire manuscript, and we are indented to them for their thorough work.
[47] Textbook: Essentials of Human Development: A Life-Span View (6th edition). By Robert Kail and John Cavanaugh. Cengage Learning, 2013.
Page 42:
Period of the Zygote (Weeks 1 and 2) …
Fertilization begins the period of the zygote, the technical term for the fertilized egg. This period ends when the zygote implants itself in the wall of the uterus (see Figure 2.4). During these two weeks, the zygote grows rapidly though cell division (see Figure 2.4). The zygote travels down the Fallopian tube toward the uterus and divides for the first time; it then continues to do so every 12 hours.
[48] Article: “Zygote.” Encyclopaedia Britannica. Accessed March 14, 2018 at <www.britannica.com>
“The joining of haploid gametes to produce a diploid zygote is a common feature in the sexual reproduction of all organisms except bacteria.”
[49] Paper: “The Marks, Mechanisms and Memory of Epigenetic States in Mammals.” By Vardhman K. Rakyan & others. Biochemical Journal, May 15, 2001. <portlandpress.com>
“Sexual reproduction in mammals results in the formation of a zygote, a single cell which contains all the necessary information to produce an entire organism comprised of billions of cells grouped into multitudinous cell types.”
[50] Book: Human Gametes and Preimplantation Embryos: Assessment and Diagnosis. Edited by David K. Gardner, Denny Sakkas, Emre Seli, and Dagan Wells. Springer, 2013.
Chapter 23: “Carbohydrate Analysis and Embryo Viability.” By Michelle Lane and David K. Gardner. Pages 259–266.
Page 260:
Concomitantly with the distinct changes in physiology that occur during development from the zygote to the blastocyst stage are dynamic changes in the metabolism of the embryo. At the zygote stage, the embryo is initially quiescent with a low metabolic and biosynthetic activity. At these early stages, the embryo predominantly uses the carboxylic acids pyruvate and lactate as its preferred energy substrates.14–16 Therefore, at these early stages of development the embryo is completely reliant on mitochondrial-based metabolism for ATP [Adenosine triphosphate] generation. However, the embryo does take up low levels of glucose,14, 15 which are likely metabolized by the pentose-phosphate pathway for the maintenance of reducing power in the cell particularly in the production of reduced glutathione for protection against oxidative stress. Furthermore, there is a recent understanding that the metabolism of glucose by the hexosamine biosynthesis pathway in the early embryo may be important in establishing O-linked glycosylation that is important for later stage development.17, 18 Therefore, it may be that this metabolism of glucose, although at a low level during the early stages of pre-implantation development, is essential for setting the subsequent metabolic program.
[51] Entry: “stimulus.” Oxford Dictionary of Biochemistry and Molecular Biology. Oxford University Press, 1997.
Page 619: “any event or phenomenon, such as radiation, electrical potential, or addition of molecules that leads to excitation of a tissue or cell.”
[52] Entry: “stimulus.” Collins English Dictionary (12th edition). HarperCollins, 2014.
“(Physiology) any drug, agent, electrical impulse, or other factor able to cause a response in an organism.”
[53] Paper: “The Role of PAF in Embryo Physiology.” By Chris O’Neill. Human Reproduction Update, May 2005. Pages 215–228. <humupd.oxfordjournals.org>
Page 215:
Embryo-derived paf [platelet-activating factor] … is produced by de novo synthesis. This synthesis commences soon after fertilization and persists throughout the preimplantation phase. … Paf also acts in an autocrine fashion as a trophic/survival factor for the early embryo. In vitro, supplementation of culture media with paf improves embryo development. …
Paf was the first mediator released by the preimplantation embryo to be identified (O’Neill, 1985a,b). It was subsequently shown that paf stimulated embryo metabolism (Ryan and others, 1989), cell-cycle progression (Roberts and others, 1993) and embryo viability (Spinks and O’Neill, 1988; Ryan and others, 1990b; Spinks and others, 1990) providing evidence for an autocrine loop in the early embryo. Insulin (Wales and others, 1985) also exerts trophic effects on the early embryo, the early embryo expresses a functional receptor for insulin (Harvey and Kaye, 1988; Heyner and others, 1989), but not insulin itself, suggesting that potential endocrine stimulation of embryo development also occurred. The possibility that a range of trophic factors may act on the early embryo was suggested by the detection of mRNA for a range of peptide growth factor ligands and their corresponding receptors (Rappolee and others, 1988). Since these observations, many putative autocrine, paracrine and endocrine factors have been implicated in supporting preimplantation embryo development (Kane and others, 1997; Kaye, 1997; Hardy and Spanos, 2002).
[54] Entry: “fertilization.” Encyclopedia & Dictionary of Medicine, Nursing & Allied Health (7th edition). Edited by Benjamin Frank Miller. W. B. Saunders, 2003.
“in human reproduction, the process by which the male’s sperm unites with the female’s oocyte, creating a new life.”
[55] Entry: “embryo.” Van Nostrand’s Scientific Encyclopedia. Edited by Douglas M. Considine. Springer, 2013.
Page 1142: “At the moment the sperm cell of the human male meets the ovum of the female and the union results in a fertilized ovum (zygote), a new life has begun.”
[56] Textbook: Excellence in Biology: Teacher’s Guide. By Jane Avis, Bridget Farham, and Karoline Hanks. Cambridge University Press, 2016. <www.cambridge.org>
Page 20: “fertilisation – in human reproduction, the process by which the male’s sperm unites with the female’s oocyte, creating a new life”
[57] Textbook: The Developing Human: Clinically Oriented Embryology (7th edition). By Keith L. Moore & T. V. N. Persaud. Saunders, 2003.
Page 2: “Zygote. This cell results from the union of an oocyte and a sperm during fertilization. A zygote is the beginning of a new human being (i.e., an embryo).”
Page 33: “The zygote is genetically unique because half of its chromosomes come from the mother and half from the father. The zygote contains a new combination of chromosomes that is different from that in the cells of either of the parents. This mechanism forms the basis of biparental inheritance and variation of the human species.”
[58] Book: An Atlas of the Human Embryo and Fetus: A Photographic Review of Human Prenatal Development. By Jan E. Jirásek (MD, DSc, Laboratory of Reproductive Embryology, Institute for the Care of Mother and Child, Prague, Czech Republic). Parthenon Publishing Group, 2001.
Page 21: “A human being originates from two living cells: the oocyte (female germ cell) and the spermatozoon (male germ cell), transmitting the torch of life to the next generation.”
[59] Teaching guide: “Human Genetic Variation.” U.S. Department of Health and Human Services, National Institutes of Health, National Human Genome Research Institute, 2007. <www.ncbi.nlm.nih.gov>
“The human genome comprises about 3 × 109 base pairs of DNA, and the extent of human genetic variation is such that no two humans, save identical twins, ever have been or will be genetically identical.”
[60] Calculated with data from:
a) Textbook: The Developing Human: Clinically Oriented Embryology (7th edition). By Keith L. Moore & T. V. N. Persaud. Saunders, 2003.
Page 16: “Human development begins at fertilization when a male gamete or sperm (spermatozoa) unites with a female gamete or oocyte (ovum) to form a single cell—a zygote.”
Page 33: “The zygote is genetically unique because half of its chromosomes come from the mother and half from the father. The zygote contains a new combination of chromosomes that is different from that in the cells of either of the parents. This mechanism forms the basis of biparental inheritance and variation of the human species.”
b) Book: Population and Evolutionary Genetics: A Primer. By Francisco J. Ayala. Benjamin Cummings Publishing Company, 1982.
Page 53: “Considerable genetic variation exists in most natural populations. … Consider humans with a 6.7% heterozygosity detectable by electrophoresis. If we assume there are 30,000 structural gene loci in a human being, which may be an underestimate, a person will be heterozygous at 30,000 X 0.067 = 2010 loci. Such an individual can theoretically produce 22010 ≈ 10605 different kinds of gametes [reproductive cells].”
c) Book: Human Reproductive Biology (3rd edition). By Richard E. Jones & Kristen H. Lopez. Academic Press, 2006.
Page 46: “Hunter-gatherer women experience about 160 lifetime ovulation cycles (menstrual cycles) as compared to 450 in women living in developed countries.”
CALCULATION: 10605 possible genetically unique reproductive cells per woman / 450 ovulation cycles = 2.2X10602
NOTE: The above calculation only accounts for the genetic variation of the female. Therefore, the odds against a woman conceiving the same pre-birth human twice (with or without the same mate) are actually much higher than this.
[61] Determined with data from:
a) Textbook: Foundations of Modern Cosmology. By John F. Hawley & Katherine A. Holcomb. Oxford University Press, 1998.
Page 454: “There are perhaps 1080 baryons in our visible universe, and about 109 photons per baryon.”
b) Book: The Inflationary Universe. By Alan Guth. Helix Books, 1997.
Page 108: “Since we believe that the observed universe has a baryon number of 1078, the conservation of baryon number would imply that it always had a baryon number of 1078.”
c) Book: Six Easy Pieces: Essentials of Physics Explained By Its Most Brilliant Teacher. By Richard Feynman. Basic Books, 1996.
Page 85: “There are a number of strange particles, a neutron and a proton are examples, which are called baryons.”
d) Article: “Atom.” World Book Encyclopedia, 2007 Deluxe Edition.
“Tiny as atoms are, they consist of even more minute particles. The three basic types are protons, neutrons, and electrons. Each atom has a definite number of these subatomic particles.”
NOTE: As shown above, all atoms contain at least one baryon, and thus 1080 represents a rough maximum for the number of atoms in the visible universe.
[62] Book: Genetic Destinies. By Peter Little. Oxford University Press, 2002.
Page 34: “Identical twins have exactly the same DNA and it so follows that any feature that is defined by gene differences should be identical between them.”
[63] Paper: “The Marks, Mechanisms and Memory of Epigenetic States in Mammals.” By Vardhman K. Rakyan & others. Biochemical Journal, May 2001. Pages 1–10. <portlandpress.com>
Page 1: “These modifications interfere with the DNA–protein interactions that facilitate transcription, resulting in transcriptional silencing of the epigenetically modified allele. Epigenetic modifications can, therefore, cause phenotypic variation in the absence of genetic differences.”
[64] Book: The First Nine Months of Life (2nd edition). By Geraldine Lux Flanagan. Simon & Shuster, 1982.
Page 35: “In the third week the body unfolds. It is one-tenth of an inch long; the heart begins to beat; the brain has two lobes; the early spinal cord is bordered by the future vertebrae and muscle segments.”
[65] Book: Gray’s Anatomy: The Anatomical Basis of Medicine and Surgery. Churchill Livingstone, 1989.
Page 261: “By Stage 9 (twentieth to twenty-second days) the neural groove is deepening and the first somites begin to appear about midway along it. The cranial half of the groove, representing developing brain, begins to develop a cephalic flexure, optic primordia become visible and early head and tail folds have appeared, as Stage 10 is approached.”
[66] Textbook: Biology: Investigating Life on Earth (2nd edition). By Vernon L. Avila. Jones and Bartlett, 1995.
Page 693: “First, the embryo has its own circulatory system, complete with a heart that started beating only 24 days after conception….”
[67] Webpage: “Merck Manual: Development of the Embryo.” By Raul Artal-Mittelmark. Merck, May 2021. Modified 9/2022. <www.merckmanuals.com>
Most organs begin to form about 3 weeks after fertilization, which equals 5 weeks of pregnancy (because doctors date pregnancy from the first day of the woman’s last menstrual period, which is typically 2 weeks before fertilization). At this time, the embryo elongates, first suggesting a human shape. Shortly thereafter, the area that will become the brain and spinal cord (neural tube) begins to develop. The heart and major blood vessels begin to develop earlier—by about day 16. The heart begins to pump fluid through blood vessels by day 20, and the first red blood cells appear the next day.
[68] Webpage: “The First Trimester.” Johns Hopkins Medicine. Accessed September 21, 2023 at <www.hopkinsmedicine.org>
“First Trimester Fetal Growth and Development Benchmarks … By the end of four weeks … The neural tube (which becomes the brain and spinal cord), the digestive system, and the heart and circulatory system begin to form. … The heart is beating.”
[69] Textbook: The Developing Human: Clinically Oriented Embryology (11th edition). By Keith L. Moore, T.V.N. Persaud, and Mark G. Torchia. Elsevier, 2020.
Page 59: “By the end of the third week, the blood is circulating, and the heart begins to beat at approximately day 22. The cardiovascular system is the first organ system to reach a functional state. The embryonic heartbeat can be detected using Doppler ultrasonography during the fourth week, approximately six weeks after the last normal menstrual period….”
[70] Paper: “The Transitional Heart: From Early Embryonic and Fetal Development to Neonatal Life.” By Cheryl Mei Jun Tan and Adam James Lewandowski. Fetal Diagnosis and Therapy, May 2020. Pages 373–386. <karger.com>
Pages 373–374:
The human heart is one of the first organs to form and function during embryogenesis1, 2. By the end of gestational week 3, passive oxygen diffusion becomes insufficient to support metabolism of the developing embryo3–5, and thus the fetal heart becomes vital for oxygen and nutrient distribution2. The initiation of the first heart beat via the primitive heart tube begins at gestational day 22, followed by active fetal blood circulation by the end of week 41, 3–5. The start of early heart development involves several types of progenitor cells that are derived from the mesoderm, proepicardium, and neural crest. This eventually leads to the formation of the 4-chambered heart by gestational week 7 via heart looping and complex cellular interactions in utero2.
[71] Article: “Embryology, Heart Tube.” By Kristen L. Farraj and Roman Zeltser. StatPearls Publishing 2023. <www.ncbi.nlm.nih.gov>
“The heart is the first functional organ that develops in humans and all other vertebrate embryos. The heart first begins to beat by week 4 of development. During the beginning stages of development, the embryo forms a trilaminar disc that matures into the looped heart along with its 5 regions. … On day 23 of development, the heart finally begins to pump.”
[72] Webpage: “Embryology: Cardiovascular System – Heart Development.” By M.A. Hill. University of New South Wales Embryology. Accessed September 22, 2023 at <embryology.med.unsw.edu.au>
“In human embryos the heart begins to beat at about 22–23 days, with blood flow beginning in the 4th week. The heart is therefore one of the earliest differentiating and functioning organs.”
[73] Textbook: Anatomy & Physiology. By Lindsay M. Biga and others. OpenStax, 2019. <open.oregonstate.education>
Chapter 19: “The Cardiovascular System: The Heart.” Pages 1173–1262.
Pages 1255–1256:
The human heart is the first functional organ to develop. It begins beating and pumping blood around day 21 or 22, a mere three weeks after fertilization. This emphasizes the critical nature of the heart in distributing blood through the vessels and the vital exchange of nutrients, oxygen, and wastes both to and from the developing baby. The critical early development of the heart is reflected by the prominent heart bulge that appears on the anterior surface of the embryo.
The heart forms from an embryonic tissue called mesoderm around 18 to 19 days after fertilization. Mesoderm is one of the three primary germ layers that differentiates early in development that collectively gives rise to all subsequent tissues and organs. The heart begins to develop near the head of the embryo in a region known as the cardiogenic area. Following chemical signals called factors from the underlying endoderm (another of the three primary germ layers), the cardiogenic area begins to form two strands called the cardiogenic cords. As the cardiogenic cords develop, a lumen rapidly develops within them. At this point, they are referred to as endocardial tubes (Figure 19.5.1). The two tubes migrate together and fuse to form a single primitive heart tube. The primitive heart tube quickly forms five distinct regions. …
The five regions of the primitive heart tube develop into recognizable structures in a fully developed heart.
[74] Book: Gray’s Anatomy: The Anatomical Basis of Medicine and Surgery. Churchill Livingstone, 1995.
Page 329: “Stages 10 to 12. Occupying days 21–23, 23–25, 25–27 respectively, … primary cerebral vesicles appear. … Rudimentary limb buds appear and the heart tubes fuse into a common loop in which contractile activity commences. The primordia of the thyroid gland, lungs, liver, pancreas, and mesonephric tubules are all identifiable.”
[75] Book: Gray’s Anatomy: The Anatomical Basis of Medicine and Surgery. Churchill Livingstone, 1995.
Page 329: “Stages 16 to 20. Roughly equivalent to the 6th and 7th weeks…. The pontine flexure, cerebral hemispheres and cerebellum are developing.”
[76] Article: “Brain.” New Millennium Encyclopedia. Simon and Shuster, 1999.
“The cerebrum is the largest part of the human brain, making up approximately 85 percent of the brain’s weight; its large surface area (cortex) and intricate development account for the superior intelligence of humans, compared with other animals. … A large part of the human cortex, the frontal area, is used for awareness, intelligence, and memory.”
[77] Book: The First Nine Months of Life (2nd edition). By Geraldine Lux Flanagan. Simon & Shuster, 1982.
Page 52:
In the sixth and seventh weeks, nerves and muscles work together for the first time. If the area of the lips, the first to become sensitive to touch, is gently stroked, the baby, who then is still an embryo, responds by bending the upper body to one side and making a quick backward motion with the arms. This is called a “total pattern” response because it involves most of the body rather than the approximate local part.
NOTE: The details above are documented by photos. Page 52: “All of the photographs in this book that show the movement of the baby are taken from” films made by Davenport Hooker at the University of Pittsburgh.
[78] Intrauterine picture taken at seven weeks after fertilization under the direction of Professor Andrzej Skawina of Collegium Medicum Jagiellonian University (Krakow, Poland) and Antoni Marsinek of the Czerwiakowski Gynecological and Obstetrics Hospital (Krakow, Poland); Photographers: Andrzej Zachwieja and Jan Walczewski. Copyright: Life Issues.
NOTE: A number of different photographers have published intrauterine photos. Just Facts asked several of these individuals for permission to reproduce their pictures, and Life Issues was the only one who consented. The pictures from Life Issues look similar to those taken by the other photographers.
[79] Book: Gray’s Anatomy: The Anatomical Basis of Medicine and Surgery. Churchill Livingstone, 1995.
Page 95: “When mammalian embryos reach a certain size, growth rather than morphogenesis occurs. The embryo is referred to as a fetus; this occurs at 56–57 postovulatory days in humans when the onset of bone marrow formation in the humerus can be seen (Streeter 1949); at this stage more than 90% of the named structures of the adult body have appeared.”
[80] Book: The First Nine Months of Life (2nd edition). By Geraldine Lux Flanagan. Simon & Shuster, 1962.
Page 48: “The appearance of the first bone cells marks the end of the embryonic period. This criterion was chosen by embryologists because the beginning bone formation coincides with the essential completion of the body.”
[81] Book: The First Nine Months of Life (2nd edition). By Geraldine Lux Flanagan. Simon & Shuster, 1962.
Pages 52–53: “By the beginning of this third month the baby moves spontaneously, without being touched, for the first time.”
[82] Article: “Fetus.” By Frank D. Allan. Encyclopedia of Human Biology (Volume 3). Academic Press, 1997.
Pages 954–955:
B. Early Fetal Period (Third Month) …
Division of the heart into chambers is complete, and a definitive vascular system carries blood to and from all body parts. …
All components of the brain and the spinal cord are formed, and nerves link the stem of the brain and the spinal cord to all tissues and organs of the body.
[83] Book: The First Nine Months of Life (2nd edition). By Geraldine Lux Flanagan. Simon & Shuster, 1962.
Pages 53–54: “In the ninth and tenth weeks, if the baby’s forehead is touched, he may turn his head away and pucker up his brow and frown. … [T]he entire body becomes sensitive to touch with a notable exception: the sides, back and top of the head.”
[84] Intrauterine picture taken at 11 weeks after fertilization under the direction of Professor Andrzej Skawina of Collegium Medicum Jagiellonian University (Krakow, Poland) and Antoni Marsinek of the Czerwiakowski Gynecological and Obstetrics Hospital (Krakow, Poland); Photographers: Andrzej Zachwieja and Jan Walczewski. Copyright: Life Issues.
NOTE: A number of different photographers have published intrauterine photos. Just Facts asked several of these individuals for permission to reproduce their pictures, and Life Issues was the only one who consented. The pictures from Life Issues look similar to those taken by the other photographers.
[85] Article: “Fetus.” By Frank D. Allan. Encyclopedia of Human Biology (Volume 3). Academic Press, 1997.
Page 962:
Attempts to suckle have been seen in utero and in aborted fetuses of 3 months. …
Reflexes that develop during the third month involve the mouth and the head…. Electrical activity of the nervous system is discernible at the same time, but periods of electrical silence can occur up to midterm.
[86] Textbook: Human Genetics: Concepts and Applications (3rd edition). By Ricki Lewis. McGraw Hill, 1998.
Page 56: “By week 12, the fetus sucks its thumb, kicks, makes fists and faces, and has the beginnings of baby teeth.”
[87] Article: “Wired to Be Social: The Ontogeny of Human Interaction.” By Umberto Castiello and others. PLoS ONE, October 7, 2010. <journals.plos.org>
Page 2: “The results showed that the spatial and temporal characteristics of foetal movements were by no means uncoordinated, but depended on the goal of the different motor acts, suggesting a surprisingly advanced level of motor planning.”
Page 3:
Each woman was identified by the prenatal sonologist during her first visit at the 12th week of pregnancy and foetal age was calculated comparing the mother’s last menstruation date and the measurements of the foetus (Crown Rump Length) taken during the ultrasound examination.
Page 9:
Twin pregnancies constitute an experiment of nature which offers the unique opportunity to explore social behaviour before birth. By investigating kinematic profiles of movements in five pairs of twin foetuses, we demonstrated that, by the 14th week of gestation, twin foetuses not only display movements directed towards the uterine wall and self-directed movements, but also movements specifically aimed at the co-twin. …
Analysis of the kinematic profiles for the different categories of movements corroborates our main hypothesis that these early contacts do not occur accidentally, but reflect motor planning.
Page 10:
In this article we describe changes in the kinematic profiles of movement in twin foetuses probing the social dimension of motor planning and control. The central advance of this study is the demonstration that ‘social actions’ are already performed in the second trimester of gestation. Starting from the 14th week of gestation twin foetuses plan and execute movements specifically aimed at the co-twin. These findings force us to predate the emergence of social behaviour: when the context enables it, as in the case of twin foetuses, other-directed actions are not only possible but predominant over self-directed actions.
NOTE: This article uses the obstetric method of counting from the last menstrual period as evidenced by the statement that “foetal age was calculated” based on the “mother’s last menstruation date.” Thus, two weeks must be subtracted to provide the actual time since fertilization.
[88] Ultrasound taken on November 25, 1997. Gestational age (GA) is 14 weeks and 4 days counted from the LMP. This falls under the category of 15 weeks after LMP and 13 weeks after fertilization.
[89] Textbook: Before We Are Born: Essentials of Embryology and Birth Defects (5th edition). By Keith L. Moore & T.V.N. Persaud. W.B. Saunders Company, 1998.
Page 106: “Limb movements, which occur at the end of the embryonic period (8 weeks), become coordinated by the 14th week, but are too slight to be felt by the mother.”
[90] Book: Embryology: Board Review Series (2nd edition). By Ronald W. Dudek & James D. Fix. Lippincott Williams & Wilkins, 1998.
Page 246:
B. Fourth month (weeks 13–16)
[91] Intrauterine picture taken at 16 weeks after fertilization under the direction of Professor Andrzej Skawina of Collegium Medicum Jagiellonian University (Krakow, Poland) and Antoni Marsinek of the Czerwiakowski Gynecological and Obstetrics Hospital (Krakow, Poland); Photographers: Andrzej Zachwieja and Jan Walczewski. Copyright: Life Issues.
NOTE: A number of different photographers have published intrauterine photos. Just Facts asked several of these individuals for permission to reproduce their pictures, and Life Issues was the only one who consented. The pictures from Life Issues look similar to those taken by the other photographers.
[92] Paper: “Pain and its Effects in the Human Neonate and Fetus.” By K.J.S. Anand & P.R. Hickey. New England Journal of Medicine, November 19, 1987. Pages 1321–1329. <www.nejm.org>
Page 1322:
Cutaneous sensory receptors appear in the perioral [mouth] area of the human fetus in the 7th week of gestation; they spread to the rest of the face, the palms of the hands and the soles of the feet by the 11th week, to the trunk and proximal parts of the arms and legs by the 15th week, and to all cutaneous and mucous surfaces by the 20th week. …
Development of the fetal neocortex begins at 8 weeks of gestation, and by 20 weeks each cortex has a full complement of 109 neurons.
NOTE: This article uses the obstetric method of counting from the last menstrual period as evidenced by the chart on page 1322, which uses a gestation of 40 weeks for pregnancy. Two weeks must be subtracted to provide the actual time since fertilization.
[93] Article: “Brain.” New Millennium Encyclopedia. Simon and Shuster, 1999.
“The cerebrum is the largest part of the human brain, making up approximately 85 percent of the brain’s weight; its large surface area (cortex) and intricate development account for the superior intelligence of humans, compared with other animals. … A large part of the human cortex, the frontal area, is used for awareness, intelligence, and memory.”
[94] Ultrasound taken on December 24, 1997. Gestational age (GA) is 19 weeks and 4 days counted from the last menstrual period. This falls under the category of 20 weeks after LMP and 18 weeks after fertilization.
[95] Article: “Fetus.” American Medical Association Complete Medical Encyclopedia. Random House, 2003.
Page 558: “At 20 weeks, the fetus is 10 inches long and about 11 ounces. The limbs have lengthened, and teeth and hair are beginning to form. The fetus now sleeps and wakes and hears sounds.”
[96] Intrauterine picture taken at 20 weeks after fertilization under the direction of Professor Andrzej Skawina of Collegium Medicum Jagiellonian University (Krakow, Poland) and Antoni Marsinek of the Czerwiakowski Gynecological and Obstetrics Hospital (Krakow, Poland); Photographers: Andrzej Zachwieja and Jan Walczewski. Copyright: Life Issues.
NOTE: A number of different photographers have published intrauterine photos. Just Facts asked several of these individuals for permission to reproduce their pictures, and Life Issues was the only one who consented. The pictures from Life Issues look similar to those taken by the other photographers.
[97] Ultrasound taken on May 31, 1999. Gestational age (GA) is 21 weeks and 5 days counted from the last menstrual period. This falls under the category of 22 weeks after LMP and 20 weeks after fertilization.
[98] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] XI:
(a) For the stage prior to approximately the end of the first trimester, the abortion decision and its effectuation must be left to the medical judgment of the pregnant woman’s attending physician.
(b) For the stage subsequent to approximately the end of the first trimester, the State, in promoting its interest in the health of the mother, may, if it chooses, regulate the abortion procedure in ways that are reasonably related to maternal health.
(c) For the stage subsequent to viability, the State in promoting its interest in the potentiality of human life may, if it chooses, regulate, and even proscribe, abortion except where it is necessary, in appropriate medical judgment, for the preservation of the life or health of the mother.
[99] Ruling: Planned Parenthood of Southeastern PA v. Casey. United States Supreme Court. June 29, 1992. <caselaw.findlaw.com>
Majority:
[T]he State may take measures to ensure that the woman’s choice is informed, and measures designed to advance this interest will not be invalidated as long as their purpose is to persuade the woman to choose childbirth over abortion. These measures must not be an undue burden on the right.
As with any medical procedure, the State may enact regulations to further the health or safety of a woman seeking an abortion. Unnecessary health regulations that have the purpose or effect of presenting a substantial obstacle to a woman seeking an abortion impose an undue burden on the right. [505 U.S. 833, 879]
Our adoption of the undue burden analysis does not disturb the central holding of Roe v. Wade, and we reaffirm that holding. Regardless of whether exceptions are made for particular circumstances, a State may not prohibit any woman from making the ultimate decision to terminate her pregnancy before viability.
NOTE: The next three footnotes provides facts about when viability occurs.
[100] Report: “Two-Year Neurodevelopmental Outcome of an Infant Born at 21 Weeks’ 4 Days’ Gestation.” By Kaashif A. Ahmad and others. Pediatrics, December 2017. <www.ncbi.nlm.nih.gov>
Page 1:
Recent literature confirms that, at the lower limit of extrauterine survival, substantial intercenter variability exists in resuscitation practice. The reasons for this variability are unclear, but may be related to disagreement on how to apply the best interests standard to extremely premature infants. Currently, both obstetric and pediatric societies recommend against assessing for viability or attempting resuscitation before 22 weeks’ gestation. In this context, we report the unimpaired 2-year outcome of a female infant resuscitated after delivery at 21 weeks’ 4 days’ gestation and 410 g birth weight. She may be the most premature known survivor to date.
Page 2: “We ascertained maturity by last menstrual period dating of 21 weeks 4 days, consistent with 9-week ultrasound dating of 21 weeks 2 days.”
NOTE: A “last menstrual period dating of 21 weeks 4 days” corresponds to 19 weeks and 4 days weeks after fertilization, or about 20 weeks. [Book: Color Atlas of Life Before Birth. By Marjorie A. England. Year Book Medical Publishers, 1983. Page 12: “Most clinicians do not know the fertilization date; the only date available to them is the first day of the last menstrual period. They use this date to define a menstrual age stretching from time 0, which is usually 14 days before fertilization….”]
[101] Article: “Extreme Preemie Born at 21 Weeks Young at Emory Decatur Hospital.” By George Franco. FOX 5 Atlanta News, December 26, 2019. <www.fox29.com>
Jemarius Jachin Harbor … emerged into the world at only 21 weeks young, weighing only 13 ounces, smaller than the size of a hand on Friday December 20. …
Gina Phillips, Director of Medical Services, with Pregnancy Aid Clinics, which helps at risk mothers said premature babies born at 23 weeks are considered the limit of viability.
“At 22 weeks some are surviving but 21 weeks is a very rarity it would be short of a miracle,” said Phillips.
She said the typical survival rate for a baby born at 21 weeks is less than four percent. …
She remains optimistic because in medicine and technology have improved survival chances of extreme preemie babies. “They did have a 21-week-old and four-day baby girl survived in Europe and without any complications, she’s several years old now,” said Phillips.
NOTE: “Gestation is the period of time between conception and birth. During this time, the baby grows and develops inside the mother’s womb. Gestational age is the common term used during pregnancy to describe how far along the pregnancy is. It is measured in weeks, from the first day of the woman’s last menstrual cycle to the current date.” [Webpage: “Gestational Age.” U.S. National Library of Medicine, National Institutes of Health. Last updated October 8, 2020. <medlineplus.gov>]
[102] Article: “Extreme Preemie, ‘About the Size of a Hand,’ Goes Home in Georgia.” FOX6 Milwaukee News, July 1, 2020. <www.fox6now.com>
Born at just 21 weeks old, Jemarius Harbor’s parents say the chances of him surviving were slim.
“He was about the size of a hand,” Jessica McPherson, Harbor’s mom said. “He had a lot of things that weren’t fully developed.” Harbor weighed 13 ounces when he was born back in December. …
For the past six months, Harbor’s parents have gone back and forth from their Jonesboro home to Emory Decatur Hospital. …
At nine pounds four ounces and about a month after his original due date in May, Harbor went home for the first time on Father’s Day.
[103] Book: Embryology: Board Review Series (2nd edition). By Ronald W. Dudek & James D. Fix. Lippincott Williams & Wilkins, 1998.
Page 247:
D. Sixth month (weeks 21–24)
[104] Article: “Fetus.” By Frank D. Allan. Encyclopedia of Human Biology (Volume 3). Academic Press, 1997.
Page 962: “Taste buds are functional at 6 months, and the modality for sweetness is well differentiated. Increased ‘drinking’ of the amniotic fluid is effected when sweet substances are introduced.”
[105] Book: The First Nine Months of Life (2nd edition). By Geraldine Lux Flanagan. Simon & Shuster, 1962.
Page 71: “In the fifth and sixth months the grip becomes strong. This baby is holding a rod and moves his arm up and down as the rod is moved.”
NOTE: The statement above is documented with a photo.
Page 52: “All of the photographs in this book that show the movement of the baby are taken from” films made by Davenport Hooker at the University of Pittsburgh.
[106] Paper: “Very Low Birth Weight Outcomes of the National Institute of Child Health and Human Development Neonatal Research Network, January 1995 Through December 1996.” By James A. Lemons, Avroy A. Fanaroff, and others. Pediatrics, January 2001. <pediatrics.aappublications.org>
Page 4:
Fig. 3. Mortality Before Discharge by Gestational Age as Estimated by Best Obstetrical Estimate Among Infants Born in NICHD [National Institute of Child Health and Human Development] Neonatal Research Network Centers Between January 1, 1995 and December 31, 1996. Data expressed as percentage died and 95% confidence intervals for each gestational age group.
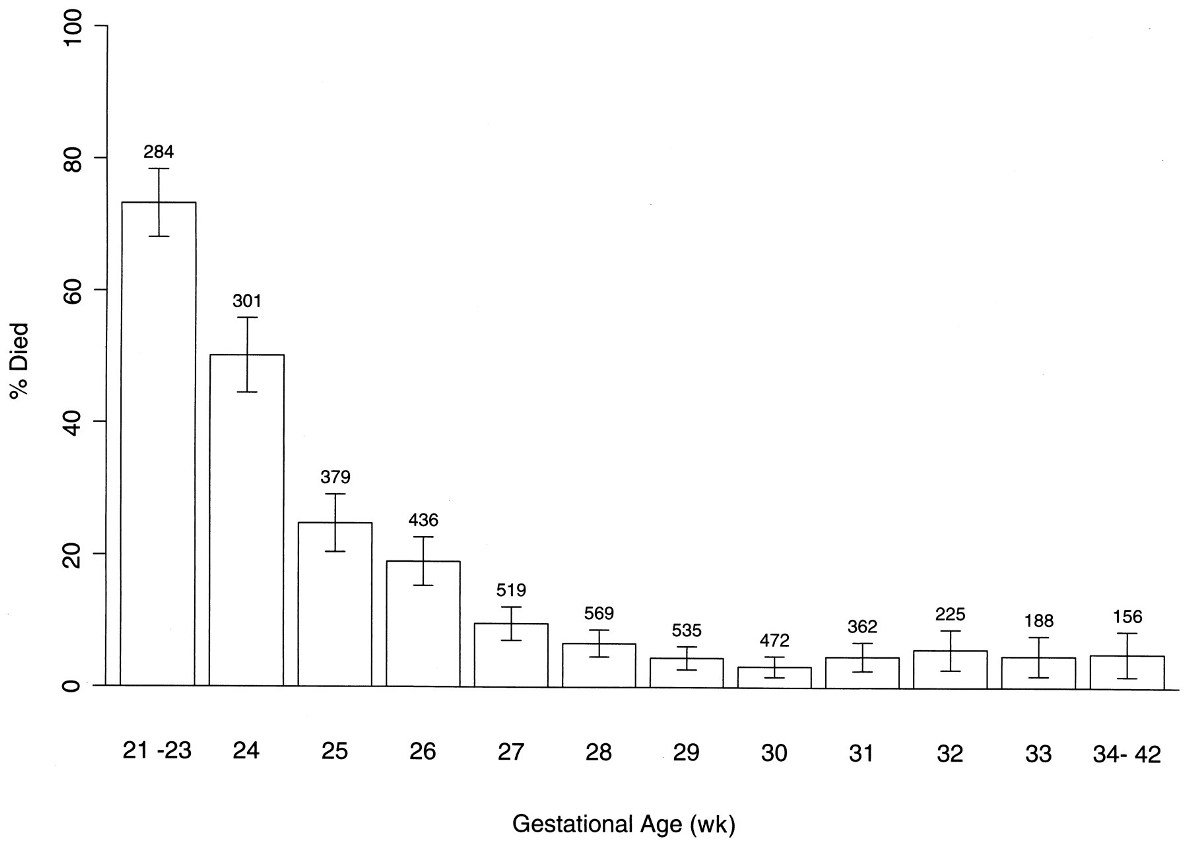
NOTES:
[107] Paper: “Fetal Homologue of Infant Crying.” By J.L. Gingras and others. Archives of Disease in Childhood: Fetal and Neonatal Edition, April 27, 2005. Pages F415–F418. <www.ncbi.nlm.nih.gov>
Page F415: “[I]n a stable state (quiet or active sleep), the fetus was challenged with … [vibroacoustic stimulation]. [This] … was provided by an artificial larynx (model 5c; Western Electric) that emits fundamental tones of about 100 Hz and 95 dB and was mechanically altered to provide exactly 0.5 second of stimulation. … The physiological intrauterine noise intensity has been reported to be about 85 dB.5”
Page F418: “The behaviors were seen in all gestational ages studied, indicating that the behavior occurs as early as 28 weeks gestation, and possibly earlier.”
[108] Advisory: “Hearing Conservation Program.” University Health Services, University of Cincinnati, June 11, 1999. <ehs.uc.edu>
|
Noise Source |
Decibels |
|
Lawn mower, food blender |
90 |
[109] Paper: “Pain and its Effects in the Human Neonate and Fetus.” By K.J.S. Anand & P.R. Hickey. New England Journal of Medicine, November 19, 1987. Pages 1321–1329. <www.nejm.org>
Page 1325:
Most recently the motor responses of 124 healthy full-term neonates to a pinprick in the leg were reported to be flexion and adduction of the upper and lower limbs associated with grimacing, crying, or both, and these responses were subsequently quantified. Similar responses have also been documented in very premature neonates, and in a recent study, Fitzgerald and others found that premature neonates (<30 weeks) not only had lower thresholds for a flexor response but also had increased sensitization after repeated stimulation. …
In other studies of the cry response to painful procedures, neonates were found to be more sensitive to pain than older infants (those 3 to 12 months old)….
NOTE: This article uses the obstetric method of counting from the last menstrual period, as evidenced by the chart on page 1322, which uses a gestation of 40 weeks for pregnancy. Two weeks must be subtracted to provide the actual time since fertilization.
[110] Paper: “Symptom Management: Acute Pain, Chapter 3—Pain in Preverbal Children.” United States National Institutes of Health, Publication Number 94-2421, June 1994. <www.nih.gov>
Page 2:
Fitzgerald demonstrated that that the pain threshold was low in premature infants. … [H]uman neonates subjected to repeated heel lances on one foot exhibited a pain threshold lower in the injured foot than in the noninjured foot. Treatment of the affected foot with a local anesthetic cream raised the pain threshold. … Serotonin (5HT) is a biogenic amine transmitter that serves an important role in pain modulation. … Serotonin levels in the young infants are low and may limit the effectiveness of the endogenous pain control mechanisms (Fitzgerald 1991b). These finding led Fitzgerald (1991b) to speculate that the established pain in the neonate could be worse than the observed pain response.
[111] Paper: “Very Low Birth Weight Outcomes of the National Institute of Child Health and Human Development Neonatal Research Network, January 1995 Through December 1996.” By James A. Lemons, Avroy A. Fanaroff, and others. Pediatrics, January 2001. <pediatrics.aappublications.org>
Page 4:
Fig. 3. Mortality Before Discharge by Gestational Age as Estimated by Best Obstetrical Estimate Among Infants Born in NICHD [National Institute of Child Health and Human Development] Neonatal Research Network Centers Between January 1, 1995 and December 31, 1996. Data expressed as percentage died and 95% confidence intervals for each gestational age group.
NOTES:
[112] This picture of a premature infant was taken three days after birth at 32 weeks after fertilization (34 weeks post-LMP).
[113] Paper: “Flavor Sensing in Utero and Emerging Discriminative Behaviors in the Human Fetus.” By Beyza Ustun and others. Psychological Science, October 2022. Pages 1651–1663. <journals.sagepub.com>
Page 1651:
The diet of pregnant women exposes fetuses to a variety of flavors consisting of compound sensations involving smell, taste, and chemesthesis. The effects of such prenatal flavor exposure on chemosensory development have so far been measured only postnatally in human infants. Here, we report the first direct evidence of human fetal responsiveness to flavors transferred via maternal consumption of a single-dose capsule by measuring frame-by-frame fetal facial movements. Pregnant women and their fetuses based in the northeast of England were involved in this study from 32 to 36 weeks’ gestation.
Page 1652:
Through their developing sensory abilities, fetuses are alert to aspects of their environment in the womb. For example, by swallowing and inhaling the amniotic fluid, a fetus can sense the flavors of food eaten by its mother. However, the current literature on human studies has exclusively focused on postnatal outcomes of prenatal flavor exposure. Instead, by analyzing their facial reactions, we present direct, novel evidence that fetuses can discriminate different flavors in amniotic fluid. We found that when fetuses were exposed to carrot flavor, they were more likely to show “laughter-face” reactions, and when they were exposed to kale flavor, they were more likely to show “cry-face” reactions. We also found that facial responses to flavors became more complex as fetuses matured. This study sheds new light not only on fetal sensory abilities but also on the specificity of facial responses to different flavors relating to their discriminative abilities.
Page 1653:
One hundred mothers between the ages of 18 and 40 years … with healthy, singleton fetuses were enrolled in this study. We chose a target sample size of 100 before recruitment to obtain 85% power … for the main comparison, that is, fetal FMs depending on the flavor exposure. Given that a recent study … reported a large and significant effect size in fetal movements at 32 weeks, medium and even large effect sizes are not unusual in this type of research. We opted to stop collecting data in the study when we reached a predetermined number of participants. Although we were able to recruit 100 women, we could not include all scans in the study for a variety of reasons.
Page 1654:
For this study, at 32 and 36 weeks’ gestation, all women underwent nonmedical 4D ultrasound scans in accordance with the British Medical Ultrasound Society guidelines…. All participants were asked not to ingest anything in the hour prior to their appointment to optimize the effect of the flavor stimuli. In the experimental groups, participants had abstained from consuming any food and/or drink involving carrot and kale on the day of the scan. Experimental group mothers swallowed one vegetable capsule (carrot/kale) with a mouthful of water approximately 20 min … before each scan. The waiting time was based on the time needed for the capsule shell to dissolve in the small…. Control group mothers were not exposed to any flavorant before and/or throughout the scans.
[114] Textbook: Before We Are Born: Essentials of Embryology and Birth Defects (5th edition). By Keith L. Moore & T.V.N. Persaud. W.B. Saunders Company, 1998.
Page 109: “The expected date of delivery (EDD) of a fetus is 266 days, or 38 weeks, after fertilization; that is, 280 days, or 40 weeks, after LNMP [last normal menstrual period] (Table 7-1).”
[115] Entry: “neonate.” Dorland’s Illustrated Medical Dictionary (29th edition). W. B. Saunders Company, 2000.
Page 1184: “a newborn infant.”
[116] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] VIII:
Specific and direct harm medically diagnosable even in early pregnancy may be involved. Maternity, or additional offspring, may force upon the woman a distressful life and future. Psychological harm may be imminent. Mental and physical health may be taxed by child care. There is also the distress, for all concerned, associated with the unwanted child, and there is the problem of bringing a child into a family already unable, psychologically and otherwise, to care for it. In other cases, as in this one, the additional difficulties and continuing stigma of unwed motherhood may be involved. All these are factors the woman and her responsible physician necessarily will consider in consultation.
[Section] XI:
For the stage subsequent to viability the State, in promoting its interest in the potentiality of human life, may, if it chooses, regulate, and even proscribe, abortion except where necessary, in appropriate medical judgment, for the preservation of the life or health of the mother. …
In Doe v. Bolton, post, p. 179, procedural requirements contained in one of the modern abortion statutes are considered. That opinion and this one, of course, are to be read together.
[117] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] IV: “[T]he medical judgment may be exercised in the light of all factors—physical, emotional, psychological, familial, and the woman’s age—relevant to the wellbeing of the patient. All these factors may relate to health.”
[118] Ruling: Planned Parenthood of Southeastern PA v. Casey. United States Supreme Court. June 29, 1992. <caselaw.findlaw.com>
Majority:
It must be stated at the outset and with clarity that Roe’s essential holding, the holding we reaffirm, has three parts. First is a recognition of the right of the woman to choose to have an abortion before viability and to obtain it without undue interference from the State. Before viability, the State’s interests are not strong enough to support a prohibition of abortion or the imposition of a substantial obstacle to the woman’s effective right to elect the procedure. Second is a confirmation of the State’s power to restrict abortions after fetal viability if the law contains exceptions for pregnancies which endanger the woman’s life or health. And third is the principle that the State has legitimate interests from the outset of the pregnancy in protecting the health of the woman and the life of the fetus that may become a child.
[119] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] IV:
D. The appellants next argue that the District Court should have declared unconstitutional three procedural demands of the Georgia statute: (1) that the abortion be performed in a hospital accredited by the Joint Commission on Accreditation of Hospitals:11 (2) that the procedure be approved by the hospital staff abortion committee; and (3) that the performing physician’s judgment be confirmed by the independent examinations of the patient by two other licensed physicians. …
We hold that the JCAH-accreditation [Joint Commission on Accreditation of Hospitals] requirement does not withstand constitutional scrutiny in the present context. …
We conclude that the interposition of the hospital abortion committee is unduly restrictive of the patient’s rights and needs that, at this point, have already been medically delineated and substantiated by her personal physician. …
There remains, however, the required confirmation by two Georgia-licensed physicians in addition to the recommendation of the pregnant woman’s own consultant (making under the statute, a total of six physicians involved, including the three on the hospital’s abortion committee). We conclude that this provision, too, must fall.
The statute’s emphasis, as has been repetitively noted, is on the attending physician’s “best clinical judgment that an abortion is necessary.” That should be sufficient. The reasons for the presence of the confirmation step in the statute are perhaps apparent, but they are insufficient to withstand constitutional challenge. … If a physician is licensed by the State, he is recognized by the State as capable of exercising acceptable clinical judgment.
[120] Article: “Daschle Bill May Not Ban Anything; Abortionists Could Use Own Judgment.” By Frank J. Murray. Washington Times, May 15, 1997. <www.washingtontimes.com>
… Dr. Warren Hern, who literally wrote the textbook on “Abortion Practice.”
The Denver gynecologist said the fact of occasional death in childbearing can justify any abortion, no matter how late it is done.
“I will certify that any pregnancy is a threat to a woman’s life and could cause ‘grievous injury’ to her ‘physical health,’ ” Dr. Hern said, using key words from the Daschle bill….
[121] Webpage: “The Guttmacher Institute’s Future.” Guttmacher Institute Board of Directors, June 23, 2005. <www.guttmacher.org>
Guiding Principles …
The Institute works to protect, expand and equalize access to information, services and rights that will enable women and men to
• avoid unplanned pregnancies;
• prevent and treat sexually transmitted infections, including HIV [human immunodeficiency virus];
• exercise the right to choose abortion;
• achieve healthy pregnancies and births; and
• have healthy, satisfying sexual relationships.
[122] Webpage: “Who Was Alan Guttmacher?” Guttmacher Institute. Accessed July 28, 2021 at <bit.ly>
The Guttmacher Institute, an independent, nonprofit, tax-exempt organization with offices in New York and Washington, D.C., was established in 1968 to provide research, policy analysis and education in the fields of reproductive health, reproductive rights and population. It was named to honor a distinguished obstetrician-gynecologist, author and leader in reproductive rights. While Alan F. Guttmacher was president of the Planned Parenthood Federation of America and a leader in the International Planned Parenthood Federation in the 1960s and early 1970s, he saw the need for the institution that now bears his name, and he nurtured its development.
[123] Webpage: “Perspectives on Sexual and Reproductive Health: A Journal of Peer-Reviewed Research.” Guttmacher Institute. Accessed July 28, 2021 at <www.guttmacher.org>
“Perspectives on Sexual and Reproductive Health is published by the Guttmacher Institute in partnership with Wiley-Blackwell and is available online only.”
[124] Paper: “Reasons U.S. Women Have Abortions: Quantitative and Qualitative Perspectives.” By Lawrence B. Finer, Lori F. Frohwirth, Lindsay A. Dauphinee, Susheela Singh, and Ann M. Moore. Perspectives on Sexual and Reproductive Health, September 2005. Pages 100–118. <www.guttmacher.org>
Page 110:
Lawrence B. Finer is associate director for domestic research, Lori F. Frohwirth is research associate, Lindsay A. Dauphinee is research assistant, Susheela Singh is vice president for research and Ann M. Moore is senior research associate—all at the Guttmacher Institute, New York. …
Methods: In 2004, a structured survey was completed by 1,209 abortion patients at 11 large providers, and in-depth interviews were conducted with 38 women at four sites. Bivariate analyses examined differences in the reasons for abortion across subgroups, and multivariate logistic regression models assessed associations between respondent characteristics and reported reasons.
Page 111:
Our eight-page questionnaire covered in detail the reasons why the respondent chose to terminate her pregnancy. The first question was open-ended: “Please describe briefly why you are choosing to have an abortion now. If you have more than one reason, please list them all, starting with the most important one first.”
Page 113:
Table 2. Percentage of women reporting that specified reasons contributed to their decision to have an abortion, 2004 and 1987 … 2004 (N=1,160) … Possible problems affecting the health of the fetus [=] 13 … Physical problem with my health [=] 12 … Was a victim of rape [=] 1 … Became pregnant as a result of incest [=] <0.5
Page 118:
This study is subject to some limitations. Our sample is not strictly nationally representative. Also, only 58% of the abortion patients seen by the participating facilities completed the survey, and nonresponse on some variables—notably, income—was high. However, the social and demographic characteristics of respondents were similar to those of two nationally representative surveys, which provides some reassurance that the findings are representative of abortion patients in the United States.
[125] Paper: “Reasons U.S. Women Have Abortions: Quantitative and Qualitative Perspectives.” By Lawrence B. Finer, Lori F. Frohwirth, Lindsay A. Dauphinee, Susheela Singh, and Ann M. Moore. Perspectives on Sexual and Reproductive Health, September 2005. Pages 100–118. <www.guttmacher.org>
Page 111:
Our eight-page questionnaire covered in detail the reasons why the respondent chose to terminate her pregnancy. The first question was open-ended: “Please describe briefly why you are choosing to have an abortion now. If you have more than one reason, please list them all, starting with the most important one first.”
Page 114:
Table 3. Percentage distribution of women having an abortion, by their most important reason for having the abortion, 2004 and 1987 … 2004 (N=957) … Physical problem with my health [=] 4 … Possible problems affecting the health of the fetus [=] 3 … Was a victim of rape [=]<0.5 … [Became pregnant as a result of incest not large enough to be listed]
[126] Textbook: Statistics: Concepts and Controversies (6th edition). By David S. Moore and William I. Notz. W. H. Freeman and Company, 2006.
Pages 42–43:
The variability of a statistic from a random sample does not depend on the size of the population as long as the population is at least 100 times larger than the sample.
Why does the size of the population have little influence on the behavior of statistics from random samples? Imagine sampling harvested corn by thrusting a scoop into a lot of corn kernels. The scoop doesn’t know whether it is surrounded by a bag of corn or by an entire truckload. As long as the corn is well mixed (so that the scoop selects a random sample), the variability of the result depends only on the size of the scoop.
Page 44:
News reports often only mention the margin of error. Most often this margin of error is for 95% confidence. That is, if we choose many samples, the truth about the population would be within the margin of error 95% of the time. We can estimate the margin of error for 95% confidence based on a simple random sample of size n by the formula 1/√n. As this formula suggests, only the size of the sample, not the size of the population matters. This is true as long as the population is much larger than the sample.
CALCULATION: 1/√1,209 = 2.9%
[127] Paper: “Reasons U.S. Women Have Abortions: Quantitative and Qualitative Perspectives.” By Lawrence B. Finer, Lori F. Frohwirth, Lindsay A. Dauphinee, Susheela Singh, and Ann M. Moore. Perspectives on Sexual and Reproductive Health, September 2005. Pages 100–118. <www.guttmacher.org>
Page 117:
Women’s reported reasons for ending pregnancies have been consistent over time. Furthermore, the proportion of women reporting each major reason changed relatively little between 1987 and 2004. The few larger changes appear to have been at least partially due to changes in the composition of the population, rather than entirely to changes in women’s tendency to give those reasons.
[128] Paper: “Reasons Why Women Have Induced Abortions: A Synthesis of Findings From 14 Countries.” By Sophia Chae and others. Contraception, October 2017. Pages 233–241. <www.sciencedirect.com>
Page 233:
We examined nationally representative data from 14 countries collected in official statistics, population-based surveys, and facility-based surveys of abortion patients. In each country, we calculated the percentage distribution of women who have abortions by main reason given for the abortion. …
In most countries, the most frequently cited reasons for having an abortion were socioeconomic concerns or limiting childbearing. With some exceptions, little variation existed in the reasons given by women’s sociodemographic characteristics.
Page 238:
Table 2. Percentage distribution of women who had an abortion by main reason given for seeking abortion, various countries and years …
Risk to maternal health … Belgium, 2011 [=] 2.9 … Kyrgyz Republic, 2012 [=] 44.4 …
Risk to fetal health … Azerbaijan, 2006 [=] 1.1 … Belgium, 2011 [=] 1.1 … Ghana, 2007 [=] 1.1 … Turkey, 2003 [=] 7.2
Page 239:
This study contains several limitations. In 11 of the 14 countries, the timeframe for abortions was 5 years prior to the survey, while marital status, educational attainment, and residence were measured at the time of the survey. Thus, women’s characteristics at the time of their abortion may differ from those at the time of the survey; this likely affects younger women disproportionately. Moreover, recall bias may affect women’s responses, especially for those who obtained an abortion further in the past. Future research should consider using panel data to overcome this limitation.
[129] Webpage: “Five Ways to Prevent Abortion (And One Way That Won’t).” Planned Parenthood, January 1, 2004. Updated 9/22/06. <www.plannedparenthood.org>
The way to prevent abortion is not to make it illegal. That won’t work. It never has. Whenever governments have made abortions illegal, they have not stopped them. Throughout the centuries, when women have felt abortion to be their only option, they have had them. Whether they were legal or not. In the two decades before abortion was legal in the United States, nearly one million women went “underground” each year for illegal operations. Thousands died for lack of medical care. Tens of thousands were maimed. All were forced to behave as if they were criminals in order to do what they felt was right for themselves. We hope those days are gone forever, even though anti-choice extremists are determined to turn back the clock.
[130] Fact Sheet: “Abortion After the First Trimester.” Planned Parenthood. Accessed October 2002 at <www.plannedparenthood.org>
“Presently the death rate from abortion at all stages of gestation is 0.6 per 100,000 procedures (Paul and others, 1999).”
NOTE: “Paul and others, 1999” is a secondary source that cites the CDC. See next footnote.
[131] Book: A Clinician’s Guide to Medical and Surgical Abortion. By Maureen Paul & others. Churchill Livingstone, 1999.
Page 19: “In the United States mortality [from abortion] was (per 100,000) 2.6 during the period 1972–1976, 0.9 in 1977–1981, 0.7 in 1982–1986, and 0.6 in 1987–1991 (based on deaths reported by the CDC [U.S. Centers for Disease Control] and number of abortions from AGI [Alan Guttmacher Institute]).”
NOTE: This corresponds to the figure for subsequent years quoted in the next footnote.
[132] Fact sheet: “Abortion Surveillance.” U.S. Centers for Disease Control, National Center for Chronic Disease Prevention & Health Promotion, June 7, 2002. <www.cdc.gov>
“The case-fatality rate for known legal induced abortion for 1993 to 1997 was 0.6 deaths per 100,000 legal abortions.”
[133] Report: “Abortion Surveillance—United States, 1996.” By Lisa M. Koonin and others. U.S. Centers for Disease Control, Division of Reproductive Health, July 30, 1999. <www.cdc.gov>
“Table 19. Number of Deaths and Case-Fatality Rates* for Abortion-Related Deaths Reported to CDC [U.S. Centers for Disease Control], by Type of Abortion – United States, 1972–1992 … Year [=] 1972 … Illegal [=] 39 … Year [=] 1974 … Legal [=] 26 … * Legal induced abortion-related deaths per 100,000 legal induced abortions.”
NOTE: The data in this source and the sources cited in the next footnote come from different divisions of the CDC and are at variance with one another due to methodological dissimilarities. It was necessary to use data from both divisions because the data from this source only goes back to 1972, and the sources in the next footnote do not isolate legal vs. illegal abortion-related deaths.
[134] Calculated with data from:
a) Report: “Table 290F. Deaths For Approximately 64 Selected Causes, By 10-Year Age Groups, Race, And Sex: United States, 1950–59.” U.S. Centers for Disease Control, National Center for Health Statistics. Accessed August 2008 at <www.cdc.gov>
Page 169 (of PDF): “Cause of Death [=] Abortion”
b) Report: “Table 290A. Deaths For 60 Selected Causes, By 10-Year Age Groups, Race, And Sex: United States, 1960–67.” U.S. Centers for Disease Control, National Center for Health Statistics. Accessed August 2008 at <www.cdc.gov>
Page 169 (of PDF): “Cause of Death [=] Abortion”
c) Report: “Table 290A. Deaths For 69 Selected Causes, By 10-Year Age Groups, Race, And Sex: United States, 1968–78.” U.S. Centers for Disease Control, National Center for Health Statistics. Accessed August 2008 at <www.cdc.gov>
Page 358 (of PDF): “Cause of Death [=] Abortions”
d) Report: “Resident Population by Age, Color, and Sex: United States, 1950–1959.” U.S. Centers for Disease Control, National Center for Health Statistics. Mailed to Just Facts from the aforementioned agency, August 7, 2008.
e) Report: “Population by Age Groups, Race, and Sex for 1960–97.” U.S. Centers for Disease Control, National Center for Health Statistics. Accessed August 2008 at <www.cdc.gov>
Page 19 (of PDF): “Resident Population of the United States by 10 Year Age Groups, Race, and Sex for 1960 and Revised Estimates for 1961–1969”
Page 21 (of PDF): “Resident Population of the United States by 10 Year Age Groups, Race, and Sex for 1960 and Revised Estimates for 1971–1979”
[135] Report: “Maternal Mortality Surveillance, United States, 1980–1985.” By Lisa M. Koonin & others. Centers for Disease Control and Prevention, Morbidity and Mortality Weekly Report, December 1, 1988. <www.cdc.gov>
Finally, the coding system used by national vital statistics and states to describe maternal deaths includes a combination of outcomes of pregnancy (e.g. ectopic pregnancy, abortion), immediate causes of death (e.g., hemorrhage), and underlying obstetrical conditions that contribute to death (e.g., obstructed labor). This system of classification precludes a determination of the real causes of maternal death. To develop strategies to prevent maternal deaths, public health personnel need to know the immediate cause of death as well as the underlying conditions that led to death.
[136] Calculated with data from:
a) Report: “Table 290F. Deaths For Approximately 64 Selected Causes, By 10-Year Age Groups, Race, And Sex: United States, 1950–59.” U.S. Centers for Disease Control, National Center for Health Statistics. Accessed August 2008 at <www.cdc.gov>
Page 167 (of PDF): “Cause of Death [=] Deliveries and Complications of Pregnancy, Childbirth and the Puerperium”
b) Report: “Table 290A. Deaths For 60 Selected Causes, By 10-Year Age Groups, Race, And Sex: United States, 1960–67.” U.S. Centers for Disease Control, National Center for Health Statistics. Accessed August 2008 at <www.cdc.gov>
Page 167 (of PDF): “Cause of Death [=] Deliveries and Complications of Pregnancy, Childbirth and the Puerperium”
c) Report: “Table 290A. Deaths For 69 Selected Causes, By 10-Year Age Groups, Race, And Sex: United States, 1968–78.” U.S. Centers for Disease Control, National Center for Health Statistics. Accessed August 2008 at <www.cdc.gov>
Page 363 (of PDF): “Cause of Death [=] Other Complications of Pregnancy, Childbirth and the Puerperium”
d) Report: “Resident Population by Age, Color, and Sex: United States, 1950–1959.” U.S. Centers for Disease Control, National Center for Health Statistics. Mailed to Just Facts from the aforementioned agency, August 7, 2008.
e) Report: “Population by Age Groups, Race, and Sex for 1960–97.” U.S. Centers for Disease Control, National Center for Health Statistics. Accessed August 2008 at <www.cdc.gov>
Page 19 (of PDF): “Resident Population of the United States by 10 Year Age Groups, Race, and Sex for 1960 and Revised Estimates for 1961–1969”
Page 21 (of PDF): “Resident Population of the United States by 10 Year Age Groups, Race, and Sex for 1960 and Revised Estimates for 1971–1979”.
[137] Report: “Maternal Mortality Surveillance, United States, 1980–1985.” By Lisa M. Koonin & others. Centers for Disease Control and Prevention, Morbidity and Mortality Weekly Report, December 1, 1988. <www.cdc.gov>
“Death certificates alone may not provide adequate information on the sequence of events that led to death. Ultimately a single code is assigned to classify the underlying cause of death. Often, however, several factors may contribute to a death; therefore, the death cannot be adequately described with a unidimensional code.”
[138] Calculated with data from:
a) Report: “Table 290F. Deaths For Approximately 64 Selected Causes, By 10-Year Age Groups, Race, And Sex: United States, 1950–59.” U.S. Centers for Disease Control, National Center for Health Statistics. Accessed August 2008 at <www.cdc.gov>
Page 1 (of PDF): “Cause of Death [=] All Causes”
Page 43 (of PDF): “Cause of Death [=] Malignant Neoplasms”
Page 199 (of PDF): “Cause of Death [=] Motor Vehicle Accidents”
Page 208 (of PDF): “Cause of Death [=] Homicide”
b) Report: “Table 290A. Deaths For 60 Selected Causes, By 10-Year Age Groups, Race, And Sex: United States, 1960–67.” U.S. Centers for Disease Control, National Center for Health Statistics. Accessed August 2008 at <www.cdc.gov>
Page 1 (of PDF): “Cause of Death [=] All Causes”
Page 40 (of PDF): “Cause of Death [=] Malignant Neoplasms”
Page 200 (of PDF): “Cause of Death [=] Motor Vehicle Accidents”
Page 210 (of PDF): “Cause of Death [=] Homicide”
c) Report: “Table 290A. Deaths For 69 Selected Causes, By 10-Year Age Groups, Race, And Sex: United States, 1968–78.” U.S. Centers for Disease Control, National Center for Health Statistics. Accessed August 2008 at <www.cdc.gov>
Page 2 (of PDF): “Cause of Death [=] All Causes”
Page 73 (of PDF): “Cause of Death [=] Malignant Neoplasms Including Neoplasms of Lymphatic and Hematopoietic Tissues”
Page 406 (of PDF): “Cause of Death [=] Motor Vehicle Accidents”
Page 422 (of PDF): “Cause of Death [=] Homicide”
d) Report: “Resident Population by Age, Color, and Sex: United States, 1950–1959.” U.S. Centers for Disease Control, National Center for Health Statistics. Mailed to Just Facts from the aforementioned agency, August 7, 2008.
e) Report: “Population by Age Groups, Race, and Sex for 1960–97.” U.S. Centers for Disease Control, National Center for Health Statistics. Accessed August 2008 at <www.cdc.gov>
Page 19 (of PDF): “Resident Population of the United States by 10 Year Age Groups, Race, and Sex for 1960 and Revised Estimates for 1961–1969”
Page 21 (of PDF): “Resident Population of the United States by 10 Year Age Groups, Race, and Sex for 1960 and Revised Estimates for 1971–1979”
[139] Fact sheet: “Abortion After the First Trimester in the United States.” By John Mugge and others. Revised by Deborah Golub. Planned Parenthood, 2004. Accessed February 16, 2017 at <www.plannedparenthood.org>
Page 3:
The risk of death from medication abortion through 63 days’ gestation is about one per 100,000 procedures (Grimes, 2005). The risk of death with surgical abortion is about one per 1,000,000 through 63 days’ gestation (Bartlett and others, 2004). The risk of death from miscarriage is about one per 100,000 (Saraiya and others, 1999). But the risk of death associated with childbirth is about 10 times as high as that associated with all abortion (Christiansen & Collins, 2006).
[140] Paper: “Pregnancy-Associated Deaths: A 15-Year Retrospective Study and Overall Review of Maternal Pathophysiology.” By Lydia R. Christiansen & Kim A. Collins. American Journal of Forensic Medicine and Pathology, March 2006. Pages 11–19. <www.ncbi.nlm.nih.gov>
Page 11:
Pregnancy-related death is defined by the International Classification of Diseases, Tenth Revision (ICD-10) as the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the cause of death. In the year 2000, a collaborative effort involving World Health Organization (WHO), UNICEF [United Nations Children’s Fund], and UNFPA [United Nations Population Fund] estimated 660 maternal deaths in the United States. This averages 11 maternal deaths per 100,000 live births reported.
Page 13: “The risk of death from complications of pregnancy decreased approximately 99% during the 20th century, from approximately 850 maternal deaths per 100,000 live births in 1900 to 7.5 in 1982.4”
Page 18: “It is evident that homicides, suicides, and accidents account for a large proportion of pregnancy-related deaths.”
NOTE: The figures from “Christiansen & Collins, 2006” cannot be used as a comparator for the others studies cited by Planned Parenthood in the footnote above (i.e., Grimes, Bartlett) because these studies are limited by gestational age and do not apply to “all abortion.”
[141] Fact sheet: “Abortion After the First Trimester.” Planned Parenthood. Accessed October 2002 at <www.plannedparenthood.org>
“Presently the death rate from abortion at all stages of gestation is 0.6 per 100,000 procedures (Paul and others, 1999). The risk of death associated with childbirth is about 10 times as high as that associated with abortion (AGI [Alan Guttmacher Institute], 1998).”
NOTE: “Paul and others, 1999” and “AGI, 1998” are secondary sources that cite the CDC [U.S. Centers for Disease Control]. See the next two footnotes.
[142] Book: A Clinician’s Guide to Medical and Surgical Abortion. By Maureen Paul & others. Churchill Livingstone, 1999.
Page 19: “In the United States mortality [from abortion] was (per 100,000) 2.6 during the period 1972–1976, 0.9 in 1977–1981, 0.7 in 1982–1986, and 0.6 in 1987–1991 (based on deaths reported by the CDC [U.S. Centers for Disease Control] and number of abortions from AGI [Alan Guttmacher Institute]).”
[143] Webpage: “Facts in Brief\Induced Abortion.” Guttmacher Institute. Accessed October 2002 at <bit.ly>
The risk of death associated with childbirth is about 10 times as high as that associated with abortion. …
The data in this fact sheet are the most current available. Most are from research conducted by the Alan Guttmacher Institute and/or published in its peer-reviewed journals. An additional source is the Centers for Disease Control and Prevention.
[144] Report: “Strategies to Reduce Pregnancy-Related Deaths: From Identification and Review to Action.” By Cynthia Berg and others. Division of Reproductive Health, U.S. Centers for Disease Control and Prevention, 2001. <stacks.cdc.gov>
Page 14:
Sources of pregnancy-related deaths are listed below in order of simplicity and convenience:
• Death certificate cause-of-death codes—the core source for finding cases.
• Manual review of death certificates.
• Pregnancy check boxes on death certificates.
• Computerized linkages of vital records.
• Other computerized data sources.
• Obstetricians, other clinicians, and groups.
• The news media.
• Autopsy and medical records.
[145] Correspondence: “Chang and Berg Respond To Horon.” By Jeani Chang & Cynthia J. Berg. American Journal of Public Health, November 2005. Pages 1879–1880. <www.ajph.org>
“We have no choice but to rely on the methods used by each reporting area to determine whether a death (including a death because of homicide) is pregnancy-associated. As stated in our discussion, the cause of death on death certificates is the most common way of ascertaining pregnancy-associated deaths.”
[146] Report: “Strategies to Reduce Pregnancy-Related Deaths: From Identification and Review to Action.” By Cynthia Berg and others. Division of Reproductive Health, U.S. Centers for Disease Control and Prevention, 2001. <stacks.cdc.gov>
Page 13:
Currently, no single source of information captures all pregnancy-related deaths, despite all deaths and essentially all live births in the United States being registered by Vital Statistics. Several reasons account for this failure:
• Lack of physician training in, or knowledge about, how to fill out a death certificate.
• ICD[International Classification of Diseases] coding rules that make the cause-of-death code on a death certificate fall outside the range of conditions considered to be pregnancy-related (in ICD-9, those codes are 630–676; in ICD-10, chapter O).
• Reliance on death certificate data to estimate cause of death.
• Medical records that fail to indicate that the events leading to death began with pregnancy, especially if the death occurred during the postpartum period.
• Medical and autopsy records that cannot be located or are not available for review.
[147] Report: “Maternal Mortality Surveillance, United States, 1980–1985.” By Lisa M. Koonin & others. Centers for Disease Control and Prevention, Morbidity and Mortality Weekly Report, December 1, 1988. <www.cdc.gov>
At present, vital statistics collected by NCHS [National Center for Health Statistics] are the only source of information about U.S. ratios of maternal mortality. Until January 1988, no systematic, national system existed for studying the epidemiology of maternal mortality. Some states collect and publish state ratios of maternal mortality; however, both the national and the state vital statistics systems have several limitations.
First, information reported from vital statistics alone is limited. Death certificates alone may not provide adequate information on the sequence of events that led to death. Ultimately a single code is assigned to classify the underlying cause of death. Often, however, several factors may contribute to a death; therefore, the death cannot be adequately described with a unidimensional code.31
[148] Correspondence: “Chang and Berg Respond To Horon.” By Jeani Chang & Cynthia J. Berg. American Journal of Public Health, November 2005. Pages 1879–1880. <www.ajph.org>
We have no choice but to rely on the methods used by each reporting area to determine whether a death (including a death because of homicide) is pregnancy-associated. As stated in our discussion, the cause of death on death certificates is the most common way of ascertaining pregnancy-associated deaths. Next is computerized linking of deaths among women of reproductive age with birth certificates and fetal death certificates; we believe this system is used in about half the reporting areas.
[149] Report: “Strategies to Reduce Pregnancy-Related Deaths: From Identification and Review to Action.” By Cynthia Berg and others. Division of Reproductive Health, U.S. Centers for Disease Control and Prevention, 2001. <stacks.cdc.gov>
Page 18:
Linking Vital Records
Death certificates for reproductive-aged women who die can be linked with certificates of reportable pregnancy outcomes (live births and fetal deaths) that occurred during the preceding year. Although many states require that induced abortions be reported, only one includes on its records identifying data that could be used to link those records with other computerized records. Linking data sets is being done in an increasing number of states, and published reports indicate that such links can increase case ascertainment by 36%† to 153% (Table 3, Box 3). However, linking vital records cannot ensure that all pregnancy-related deaths will be identified, since only about two-thirds to three-quarters of pregnancy-related deaths are associated with either a live birth or a fetal death. Excluded from linkages would be deaths associated with ectopic pregnancies, induced and some spontaneous abortions, gestational trophoblastic disease, and undelivered pregnancies.
NOTE: † This figure of 36% is in error. The figure should be 30%, as per Table 3 on page 19, which is the cited source (see below).
Page 19:
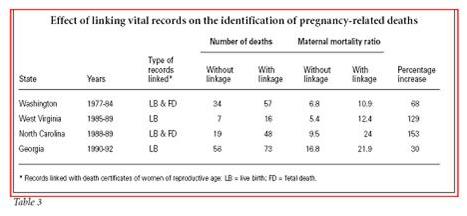
[150] Report: “Strategies to Reduce Pregnancy-Related Deaths: From Identification and Review to Action.” By Cynthia Berg and others. Division of Reproductive Health, U.S. Centers for Disease Control and Prevention, 2001. <stacks.cdc.gov>
Page 18:
Linking Vital Records
Death certificates for reproductive-aged women who die can be linked with certificates of reportable pregnancy outcomes (live births and fetal deaths) that occurred during the preceding year. Although many states require that induced abortions be reported, only one includes on its records identifying data that could be used to link those records with other computerized records.
[151] Report: “Maternal Mortality Surveillance, United States, 1980–1985.” By Lisa M. Koonin & others. Centers for Disease Control and Prevention, Morbidity and Mortality Weekly Report, December 1, 1988. <www.cdc.gov>
Finally, the coding system used by national vital statistics and states to describe maternal deaths includes a combination of outcomes of pregnancy (e.g. ectopic pregnancy, abortion), immediate causes of death (e.g., hemorrhage), and underlying obstetrical conditions that contribute to death (e.g., obstructed labor). This system of classification precludes a determination of the real causes of maternal death. To develop strategies to prevent maternal deaths, public health personnel need to know the immediate cause of death as well as the underlying conditions that led to death.
[152] Report: “Strategies to Reduce Pregnancy-Related Deaths: From Identification and Review to Action.” By Cynthia Berg and others. Division of Reproductive Health, U.S. Centers for Disease Control and Prevention, 2001. <stacks.cdc.gov>
Page 25:
Maternal Mortality Review Committees
In most cases, the state is the level at which pregnancy-related deaths are reviewed, although the process can occur in some very large cities and counties. The legislation that enables maternal mortality review and the review committee’s place within the governmental organization vary widely from state to state.
[153] Webpage: “CDC’s Abortion Surveillance System: FAQs.” U.S. Centers for Disease Control, Division of Reproductive Health. Updated January 06, 2017. <www.cdc.gov>
Are States Required to Report Their Abortion Statistics to CDC?
No, states and areas voluntarily report data to CDC for report preparation. CDC’s Division of Reproductive Health prepares surveillance reports as data becomes available. There is no national requirement for data submission or reporting.
[154] Phone call from Just Facts to the U.S. Centers for Disease Control, Division of Reproductive Health, July 1, 2008.
Just Facts requested a state-by-state breakdown of the data in Table 19 of “Abortion Surveillance—United States, 2004,” which shows abortion-related fatalities for 1972–2003. The CDC would not release this data on the grounds that it would violate their privacy agreements with certain states.
[155] Paper: “Physician and Public Opinions on Quality of Health Care and the Problem of Medical Errors.” By Andrew R. Robinson and others. Archives of Internal Medicine, October 28, 2002. Pages 2186–2190. <archinte.ama-assn.org>
Page 2186: “Uniformly, physicians believed that fear of medical malpractice is a barrier to reporting of errors and that greater legal safeguards are necessary for a mandatory reporting system to be successful.”
Page 2189: “Table 4. Colorado and National Physician Opinions … Medical malpractice litigation is a barrier to the reporting of medical errors. … National No. (%) [=] 299 (98.4)”
NOTE: 98.4% of physicians in the national sample agreed with this statement.
[156] Report: “Vital Statistics of the United States, 1989. Volume II—Mortality, Part A.” U.S. Centers for Disease Control, National Center for Health Statistics and Prevention, 1993. <www.cdc.gov>
Page 13 (of PDF):
Symbols Used in Tables
Data not available ---
Category not applicable …
Quantity zero –
Page 262: “Table 1-25. Deaths From 282 Selected Causes, by Race—United States and Each State: 1989.”
|
Cause of Death |
Maryland (All races) |
|
Legally induced abortion |
– |
NOTE: Abortion-related mortality data provided by the CDC’s [U.S. Centers for Disease Control] National Center for Health Statistics is at variance with that provided by CDC’s Division of Reproductive Health due to methodological dissimilarities. The National Center for Health Statistics is only cited here because the Division of Reproductive Health does not break down their national data on a state-by states basis. In July 2008, Just Facts filed a Freedom of Information Act Request with the CDC for this data and is awaiting a response.
[157] Report: “Vital Statistics of the United States, 1990. Volume II—Mortality, Part A.” U.S. Centers for Disease Control, National Center for Health Statistics and Prevention, 1994. <www.cdc.gov>
Page 262: “Table 1-25. Deaths From 282 Selected Causes, by Race—United States and Each State: 1990.”
|
Cause of Death |
Maryland (All Races) |
|
Legally induced abortion |
— |
[158] Report: “Vital Statistics of the United States, 1991. Volume II—Mortality, Part A.” U.S. Centers for Disease Control, National Center for Health Statistics and Prevention, 1996. <www.cdc.gov>
Page 262: “Table 1-25. Deaths From 282 Selected Causes, by Race—United States and Each State: 1991.”
|
Cause of Death |
Maryland (All Races) |
|
Legally induced abortion |
— |
[159] Report: “Vital Statistics of the United States, 1992. Volume II – Mortality, Part B.” U.S. Centers for Disease Control, National Center for Health Statistics and Prevention, 1996. <www.cdc.gov>
Page 320: “Table 8-6. Deaths From 72 Selected Causes, by 10-Year Age Groups, Race, and Sex.”
|
Maryland, Cause of Death: Pregnancy with Abortive Outcome |
Female (Total of All Age Groups) |
|
White |
— |
|
All other |
— |
|
Black |
— |
[160] Autopsy number 89-593: “Erica Richardson.” By Julia C. Goodin & others. Office of the Chief Medical Examiner, State of Maryland, June 28, 1989. Autopsy performed on March 3, 1989. <health.maryland.gov>
Page 1: “Description of Injury … Close examination of the anterior portion of the uterus showed a large irregular perforation of the anterior lower uterine wall which extended into a portion of the cervix.”
Page 5:
Opinion: This, 16 year old black female, Erica Richardson, died from rupture of lower uterus and cervix with complications, including hemorrhage into the pelvic cavity surrounding the uterus and air embolism (air escaping into the vasculature and heart). According to police reports, the deceased was known to have been pregnant and this is consistent with autopsy findings. However, she had undergone an evacuation [abortion] procedure which resulted in perforation of the uterus.
[161] Article: “Teen’s Death After Abortion Brings Suit.” By Larry Perl. Prince George’s Journal Weekly, May 30–31, 1990.
The malpractice suit claims that on the evening of March 1, 1989, Dr. Gene Crawford punctured 16-year-old Erica Kae Richardson’s uterus and cervix—then left her “bleeding to death” on an operating table in his Laurel office for four hours, without monitoring vital signs.
At 10:45 p.m., Crawford carried Richardson to her aunt’s car and told the aunt to “take [her] home and out her to bed,” the suit states. … The aunt, deciding that her niece needed “emergency treatment,” drove to Bowie Health Center, where Richardson was rushed into the emergency room at 11 p.m., in respiratory arrest, and died shortly after midnight the suit states. …
Richardson’s mother … referred questions to the attorneys. … Donald McLaughlin said Richardson’s aunt, Denise Crarey, helped Richardson get an abortion without telling Richardson’s mother. McLaughlin added that though Crarey and Richardson’s mother are sisters, they have “a very strained relationship.” Crarey, a registered nurse, took Richardson first to Washington Hospital Center, which wouldn’t perform the abortion because Richardson was too far along in her pregnancy, McLaughlin said.
[162] Article: “Mother Is Suing Doctor: Daughter Died After Abortion.” By Melanie Mader. Maryland Laurel Leader, June 29, 1990. Pages A1, 3. <www.baltimoresun.com>
Page A3: “Richardson-Smith was unaware that her daughter was having an abortion until the Bowie medical center called her, McLaughlin said.”
[163] Press release: “Human Life International Claims Maryland Health Department ‘Ignores, Covers-Up’ Abortion Deaths.” PR Newswire, November 21, 1991. <www.prnewswire.com>
“Erica Richardson, 16, died March 2, 1989, just hours after an abortion was performed upon her by Dr. Gene O. Crawford at his Metropolitan Women’s Center, 9811 Mallard Dr., Laurel, Md.”
[164] Article: “2 Tragedies Raise Doubts About Suitland Clinic; Abortion Patient, Left Paralyzed, Files Suit.” By Retha Hill. Washington Post, August 13, 1990. Page A1. <www.washingtonpost.com>
Kioko and Lofton said they have also been interviewed by board investigators about the death of Debra M. Gray, a 34-year-old woman….
The Physicians Quality Assurance Board is also looking at the case of Debra Gray, a secretary at the Naval Hospital, who went to the Hillview night clinic on July 12, 1989. …
Paramedics were called to the clinic, where Gray had gone into cardiac arrest; her brain was deprived of oxygen for at least 12 minutes, according to the autopsy records and family members. Gray, who was later found to have traces of heroin in her system, was rushed to Malcolm Grow Hospital at Andrews Air Force Base, where doctors detected no brain activity. Three days later, doctors disconnected life support systems. …
The state Medical Examiner’s Office reported that Gray’s death was precipitated by a reaction of the heroin in her system with the barbiturate. …
Kioko, who was the gynecologist performing the abortion, said that a registered nurse mixed and injected the barbiturate into Gray, and that clinic personnel thought it would put her into a “twilight” state rather than under general anesthesia.
Barbara Lofton agreed with Kioko that no anesthesiologist was at the clinic during the time Logan and Gray underwent abortions, but she said physicians administered the anesthetic. Kioko denied that.
[165] Article: “2 Tragedies Raise Doubts About Suitland Clinic; Abortion Patient, Left Paralyzed, Files Suit.” By Retha Hill. Washington Post, August 13, 1990. Page A1. <www.washingtonpost.com>
Susanne Renee Logan was three months pregnant when she went to Hillview Women’s Medical Surgical Center for an abortion. …
In sworn statements contained in a lawsuit Logan has filed, paramedics said that the 32-year-old woman was blue and in cardiac arrest when they arrived. Paramedics said clinic personnel attempted to revive her with a medicine that medical experts say has no effect on reversing the reaction to Brevital. Clinic workers had tried to resuscitate her with oxygen equipment that was not working. An oxygen mask placed over her nose and mouth was upside down. Furthermore, there was no anesthesiologist on duty to administer the drug or monitor Logan’s vital signs, according to interviews with clinic personnel. …
After four months in a coma, Logan, who suffered extensive brain damage in the Sept. 9 incident, is almost completely paralyzed. …
The emergency workers gave Logan the stimulant epinephrine intravenously, after which her heartbeat was restored.
[166] Article: “Botched-Abortion Victim Dies in Baltimore.” Washington Times, December 2, 1992. <www.washingtontimes.com>
“Susanne Logan, the Forestville woman who was paralyzed in a botched 1989 abortion at a Suitland clinic, died in Baltimore yesterday of complications from pneumonia, just three weeks after she won a multimillion-dollar settlement in her case.”
[167] Article: “Pneumonia – Diseases.” By Robert Baird. American Chronicle, March 2, 2008.
[Pneumonia] is often the final complication of some other debilitating disorder, and this is why many people who get pneumonia die. Any one whose resistance is already low is very susceptible to pneumonia, so for people who are dying of heart failure, cancer, stroke or chronic bronchitis, the actual cause of death is often pneumonia. In anyone who is semi-conscious or paralyzed, infection of the lungs is extremely likely. This is because under such conditions the normal coughing reflex that keeps the lungs clear of mucus and stagnant fluid is reduced, or even absent.
[168] Book: Victims of Choice. By Kevin Sherlock. Brennyman Books, 1996.
Page 134:
Gladyss Estanislao. This 28-year-old married Filipina woman, a legal secretary who lived in Prince George’s County, died May 12, 1989, 17 days after Alan Ross reportedly performed a vacuum abortion on her at the Wisconsin Avenue Women’s Health Care Center in Bethesda. Ross reportedly failed to diagnose Gladyss was ectopically pregnant, and then he reportedly botched the abortion.
NOTE: The sources cited are Ms. Estanislao’s death certificate and a 12/5/91 article in The Wanderer. Note the discrepancy with the source below regarding the type of abortion procedure.
[169] Article: “Sudden Death Due to Rupture of Ectopic Pregnancy Concurrent with Therapeutic Abortion.” By Ling Li & John E. Smialek. Archives of Pathology & Laboratory Medicine, July 1993. Pages 698–700. <www.ncbi.nlm.nih.gov>
Page 698: “In 1989, a case of sudden death secondary to EP [ectopic pregnancy] was investigated by the Office of the Chief Medical Examiner for the State of Maryland, Baltimore.”
Page 699:
In 1989, a 28-year-old female college student was found unresponsive on the bathroom floor near her classroom. … the subject was transported to a local hospital where she was pronounced dead on arrival.
Further investigation revealed that the woman had been seen at a clinic for a missed abortion 17 days before her death and underwent a dilation and curettage [abortion procedure]. No surgical specimen was sent to the laboratory for pathologic examination before she left the clinic. …
… A 0.3 cm rupture site was located on the lateral surface [of the left fallopian tube], surrounded by hemorrhagic tissue.
[170] Commentary: “Ectopic Pregnancy in Association with Induced Abortion: Message for the Pathologist.” By Jane W. Hardman & others. Archives of Pathology & Laboratory Medicine, July 1993. Pages 696–697. <www.ncbi.nlm.nih.gov>
Page 696: “Admittedly, in each of these cases there was a failure on the part of clinicians to recognize the clinical signs of ectopic pregnancy and to follow up with the patients accordingly.”
Page 697: “In summary, recommendations that are already in place, had they been followed in the cases reported by Drs Li and Smialek, should have prevented the deaths of three young women.”
[171] Article: “Pregnancy.” By Lynn J. Romrell (Ph.D., Associate Dean for Education and Professor of Anatomy and Cell Biology, University of Florida College of Medicine). World Book Encyclopedia, 2007 Deluxe Edition.
“An ectopic pregnancy occurs when a fertilized egg implants itself outside the uterus, usually inside the fallopian tube, the tube through which the egg passes on its way from the ovary to the uterus. The developing baby cannot survive in an ectopic pregnancy. The pregnancy may be fatal to the mother if untreated.”
[172] Book: Essentials of Medical Ultrasound: A Practical Introduction to the Principles, Techniques and Biomedical Applications. Edited by Michael H. Repacholi and Deirdre A. Benwell. Humana Press, 1982.
Chapter 5: “Clinical Applications of Diagnostic Ultrasound.” By Edward A. Lyons. Pages 141–180.
Page 176: “An important diagnosis to make is that of an ectopic pregnancy. If the pregnancy test is positive and the uterus is empty, one may be able to visualize [via ultrasound] a mass in the tube. In that instance the diagnosis of ectopic is almost 100% certain.”
[173] Textbook: Ultrasound and the Fallopian Tube. Edited by Ilan E. Timor-Tritsch & Asim Kurjak. Parthenon Publishing Group, 1996.
Chapter 4: “Ultrasonic Aspects of Ectopic Pregnancy.” By I. E. Timor-Tritsch & others. Pages 27–50.
Page 29:
One of the explicit advantages of the modern pregnancy tests … is that they can be employed in the emergency room or in the office of the gynecologist. This definitely presents an advantage since, in applying this pregnancy test followed by an office ultrasound examination of the pelvis, a fast and almost always reliable diagnosis of the presence or absence of an abnormal or normal intrauterine pregnancy can be made. In the case of an ectopic pregnancy, the chances of making the diagnosis during the first visit to the gynecologist’s office or the emergency room are high.
[174] Textbook: Ultrasound and the Fallopian Tube. Edited by Ilan E. Timor-Tritsch & Asim Kurjak. Parthenon Publishing Group, 1996.
Chapter 5: “Conservative Management of Ectopic Pregnancy Based on Color Doppler Studies.” By F. Bonilla Musoles & others. Pages 51–62.
Page 51: “Even with techniques currently available, ectopic pregnancy … results in death for one of every 2000 women affected.1 The incidence of ectopic pregnancies varies between 0.5 and 1% of all pregnancies.”
Page 52: “In most published reports about ectopic pregnancies, the diagnosis is established by [a specialized blood test] in patients with a positive pregnancy test in whom an intrauterine [in the uterus] gestational sac, with or without recognizable embryonic structures, cannot be seen by ultrasound examination.”
[175] Book: Victims of Choice. By Kevin Sherlock. Brennyman Books, 1996.
Pages 166–167:
The City of New York
Commissioner of Health
Stephen C. Joseph, M.D., M.P.H.
To: All Gynecologists, Anesthesiologists, Administrators and Others Concerned With the Provision of Abortion Services
From: Stephen Joseph, M.D., M.P.H., Commissioner of Health
Subject: Anesthesia Alert
Date: June 5, 1987 …
Complications of general anesthesia account for a substantial number of death resulting from reproductive-health-related surgery. …
During the period between 1981 and 1984, there were 30 legal abortion-related deaths in New York City….
… Particular attention must be given to dosage calculation by patient’s weight and drug interactions with other sedative or anesthetic agents.
[176] Calculated with data from the report: “Abortion Surveillance—United States, 2013.” By Tara C. Jatlaoui and others. U.S. Centers for Disease Control, Division of Reproductive Health, November 25, 2016. <www.cdc.gov>
Page 43:
Table 23. Number of Deaths and Case-Fatality Rates* for Abortion-Related Deaths Reported to CDC [U.S. Centers for Disease Control], by Type of Abortion — United States, 1973–2012† … Type of Abortion … Induced … Legal§ … Year 1981 [=] 8 … Year 1982 [=] 11 … Year 1983 [=] 11 … Year 1984 [=] 12 …
* Number of legal induced abortion-related deaths per 100,000 reported legal induced abortions. Because a substantial number of legal induced abortions occurred outside reporting areas that provided data to CDC, national case-fatality rates (i.e., number of legal induced abortion-related deaths per 100,000 reported legal induced abortions in the United States) were calculated with denominator data from a more complete source.(15,67) Case-fatality rates were computed for consecutive 5-year periods during 1973–2012 because rates based on <20 cases are highly variable.(38)
† Certain numbers might differ from those in reports published previously because additional information has been supplied to CDC subsequent to publication.
§ An abortion is defined as legal if it was performed by a licensed clinician within the limits of state law.
CALCULATION: 8 + 11 + 11 + 12 = 42
[177] Calculated with data from:
a) Webpage: “City of New York & Boroughs: Population & Population Density from 1790.” Demographia. Accessed August 2008 at <www.demographia.com>
“Population (In Thousands) … 1980 … Total [=] 7,072”
b) Webpage: “Historical National Population Estimates: July 1, 1900 to July 1, 1999.” U.S. Census Bureau, April 11, 2000. Revised June 28, 2000. <www2.census.gov>
“National Population … July 1, 1980… Total [=] 227,224,681”
CALCULATIONS:
[178] Webpage: “Abortion Services.” Planned Parenthood of Nassau County. Accessed June 28, 2008 at <www.plannedparenthood.org>
Abortion DOES NOT
• Prevent future pregnancies
• Make miscarriage more likely
• Cause premature birth, birth defects or low infant birth weight in future pregnancies
• Increase the chance of infant death in the future
• Cause breast cancer
[179] Paper: “Cost Consequences of Induced Abortion as an Attributable Risk for Preterm Birth and Impact on Informed Consent.” By Byron C. Calhoun, Elizabeth Shadigian & Brent Rooney. Journal of Reproductive Medicine, October 2007. Pages 929–937. <www.ncbi.nlm.nih.gov>
Page 930: “Fifty-nine studies were reviewed for preterm birth and links to abortion…. From this review, we selected 5 of the most recent, representative studies with an association between induced abortion and preterm birth as detailed examples of the 59 studies published in Appendix B….”
Pages 930–931:
Five large, recent, international studies have shown an association of prior abortions to preterm delivery3,6–9 (Table IV), and 50 studies over the last 50 years have shown a statistically significant association (Appendix B). All of the studies found a statistically significant increase in preterm births before 32 weeks for women undergoing at least 1 first-trimester abortion, with the ORs [odds ratios] ranging from 1.3 to 2.5.3,6–9 Women undergoing [two or more] abortions had an even larger risk of preterm birth, with ORs ranging from 1.8 to 5.2.3,6–9.
[180] Webpage: “Preterm Birth.” March of Dimes, February 2007. <www.marchofdimes.com>
Premature birth is a serious health problem. Premature babies are at increased risk for newborn health complications, as well as lasting disabilities, such as mental retardation, cerebral palsy, lung and gastrointestinal problems, vision and hearing loss, and even death. Many premature babies require care in a neonatal intensive care unit (NICU), which has specialized medical staff and equipment that can deal with the multiple problems faced by premature infants. …
All premature babies are at risk for health problems, but those born before about 32 weeks of gestation face the highest risk.
[181] Webpage: “Abortion Services: Risks and Side Effects.” Planned Parenthood of the Rocky Mountains. Updated September 21, 2007. Accessed July 2008 at <www.plannedparenthood.org>
“Serious, long-term emotional problems after abortion are about as common as they are after childbirth.”
[182] Webpage: “Abortion Procedures.” Planned Parenthood, February 8, 2008. Accessed July 2008 at <www.plannedparenthood.org>
“Serious, long-term emotional problems after abortion are about as uncommon as they are after giving birth.”
[183] Webpage: “Ask Dr. Cullins: Is Having an Abortion Emotionally and Psychologically Dangerous?” Planned Parenthood, August 6, 2004. Updated 1/23/07. <www.plannedparenthood.org>
Q: Is having an abortion emotionally and psychologically dangerous?
A: No. Most women feel relief after an abortion. Serious emotional problems after abortion are much less likely than they are after giving birth. But anti choice extremists make false claims about this. They want people to believe that most women who choose abortion suffer severe and long lasting emotional trauma. This is not true.
[184] Webpage: “Pregnant, Now What?” By Jon Knowles. Planned Parenthood, January 1, 1993. Revised 5/5/07 by Jennifer Johnsen. <www.plannedparenthood.org>
Beware of so-called “crisis pregnancy centers” that are anti-abortion. These fake clinics advertise free pregnancy testing to lure women into their anti-choice agenda.
Crisis pregnancy centers
• may perform your pregnancy tests without medical supervision.
• won’t give you complete and correct information about all options.
• may try to frighten you with misleading films and pictures that are designed to keep you from choosing abortion.
• will lie to you about the medical and emotional effects of abortion.
[185] Article: “Abortion Is Four Times Deadlier Than Childbirth: New Studies Unmask High Maternal Death Rates From Abortion.” By David C. Reardon. Post–Abortion Review, April–June 2000. <www.afterabortion.org>
“Since Finland has socialized medical care, these records are very accurate and complete.”
[186] Paper: “Suicides After Pregnancy in Finland, 1987–94: Register Linkage Study.” By Mika Gissler, Elina Hemminki & Jouko Lonnqvist. British Medical Journal, December 7, 1996. <www.bmj.com>
Information on suicides in women of reproductive age was linked with the Finnish birth, abortion, and hospital discharge registers to find out how many women who committed suicide had had a completed pregnancy during her last year of life. … There were 73 suicides associated with pregnancy, representing 5.4% of all suicides in women in this age group. The mean annual suicide rate was 11.3 per 100 000. The suicide rate associated with birth was significantly lower (5.9) and the rates associated with miscarriage (18.1) and induced abortion (34.7) were significantly higher than in the population.
[187] Paper: “Deaths Associated With Pregnancy Outcome: A Record Linkage Study of Low Income Women.” By David C. Reardon and others. Southern Medical Journal, August 2002. Pages 834–841. <www.afterabortion.org>
Page 837: “Table 2. Detailed Cause-Specific Deaths and Death Rates in 8 Subsequent Years for Women with a History of at Least One Abortion Compared with Women Having No Known History of Abortion, by Reproductive History … Cause of Death … (1) Delivery Only … Suicides [=] 24.9 … Cause of Death … (2) Abortion Only … Suicides [=] 62.8”
CALCULATION: 62.8 Abortion Only Suicides / 24.9 Delivery Only Suicides = 2.5
[188] Article: “Changing Abortion’s Pronoun.” By Stephanie Simon. Los Angeles Times, January 7, 2008. <www.latimes.com>
The concept of post-abortion trauma is hotly disputed. Several studies published in peer-reviewed medical journals suggest that women who have had abortions are more prone to depression or drug abuse. But the research does not prove cause and effect, Stotland said.
It may be, she said, that women who have abortions are more emotionally unstable in the first place. Abortion is one of the most common surgeries in the country, with more than 1 million performed a year; while some who chose the procedure surely come to regret it, doctors say they see no epidemic of trauma in either men or women.
[189] Paper: “Deaths Associated With Pregnancy Outcome: A Record Linkage Study of Low Income Women.” By David C. Reardon and others. Southern Medical Journal, August 2002. Pages 834–841. <www.afterabortion.org>
Page 838: “Table 3. Risk of Death by Specific Causes in 8 Subsequent Years for Women with Only One Known Pregnancy (Those with an Abortion vs Those with a Delivery) … Delivery of First Pregnancy and No Abortions … Cause of Death … Suicides [=] 19.1 … Abortion of First Pregnancy … Cause of Death … Suicides [=] 63.0”
CALCULATION: 63.0 Abortion of First Pregnancy / 19.1 Delivery of First Pregnancy and No Abortions = 3.3
[190] Article: “Abortion and Subsequent Mental Health: Review of the Literature.” By Carlo V. Bellieni (MD) and Giuseppe Buonocore (MD, PhD). Psychiatry and Clinical Neurosciences, July 2013. Pages 301–310. <onlinelibrary.wiley.com>
Page 301:
The risk that abortion may be correlated with subsequent mental disorders needs a careful assessment, in order to offer women full information when facing a difficult pregnancy. All research papers published between 1995 and 2011, were examined, to retrieve those assessing any correlation between abortion and subsequent mental problems. A total of 36 studies were retrieved, and six of them were excluded for methodological bias. … Abortion versus childbirth: 13 studies showed a clear risk for at least one of the reported mental problems in the abortion group versus childbirth, five papers showed no difference, in particular if women do not consider their experience of fetal loss to be difficult, or if after a fetal reduction the desired fetus survives. Only one paper reported a worse mental outcome for childbearing. Abortion versus unplanned pregnancies ending with childbirth: four studies found a higher risk in the abortion groups and three, no difference. Abortion versus miscarriage: three studies showed a greater risk of mental disorders due to abortion, four found no difference and two found that short-term anxiety and depression were higher in the miscarriage group, while long-term anxiety and depression were present only in the abortion group. …
We performed a search in PubMed and Medscape from the year 1995 to 2011. We used as key words the following: “abortion,” “mental disorder,” “depression” “anxiety,” “illicit drugs” “tobacco,” “alcohol.”
Page 302:
We retrieved 36 papers.7–42 We excluded seven studies: two for absence of a control group,26, 40 one because the control group was composed of women’s partners,25 one because it did not use a validated questionnaire,22 one because it compared the consequences of medical and surgical abortion,42 one because it was a re-elaboration of a previous paper to investigate the causes of the increase of depression in the abortion group,19 and one because there was no statistical comparison between abortion and childbirth groups.39
Page 307: “The rates of the single outcomes in the various groups of women should be outlined; in some studies rates are not available, and this makes this analysis difficult, but there is a general convergence of the data.”
[191] Calculated with data from the paper: “Relationship Between Induced Abortion and the Incidence of Depression, Anxiety Disorder, Adjustment Disorder, and Somatoform Disorder in Germany.” By Louis Jacob and others. Journal of Psychiatric Research, July 2019. Pages 75–79. <www.sciencedirect.com>
Page 75:
Aim: The goal of this retrospective cohort study was to analyze the relationship between induced abortion and the incidence of depression, anxiety disorder, adjustment disorder, and somatoform disorder in Germany.
Methods: Women who had undergone induced abortions for the first time in 281 gynecological practices in Germany between January 2007 and December 2016 were included (index date). Women with live births were matched (1:1) to those with induced abortion by age, index year, and physician. The main outcome of the study was the incidence of depression, anxiety disorder, adjustment disorder, and somatoform disorder as a function of induced abortion. Survival analyses and Cox regression models were used to investigate the association between induced abortion and psychiatric disorders.
Results: This study included 17581 women who had had an induced abortion and 17581 women who had had a live birth.
Page 76:
This study was based on data from the Disease Analyzer database (IQVIA), which compiles drug prescriptions, diagnoses, and basic medical and demographic data obtained directly and in anonymous format from computer systems used in the practices of general practitioners and specialists…. Diagnoses (International Classification of Diseases, 10th revision [ICD 10]), prescriptions (Anatomical Therapeutic Chemical [ATC] classification system), and the quality of reported data are being monitored by IQVIA based on a number of criteria (e.g., completeness of documentation, linkage between diagnoses and prescriptions). In Germany, the sampling methods used for the selection of medical practices were appropriate for obtaining a representative database of general and specialized practices…. The prescription statistics for several drugs were very similar to the data available from pharmaceutical prescription reports. The age groups for the given diagnoses in the Disease Analyzer database also matched those in corresponding disease registries. …
This study included women who had undergone induced abortions … for the first time in one of 281 gynecological practices in Germany between January 2007 and December 2016 (index date). There were several inclusion criteria: no documentation of pregnancy with abortive outcome … or delivery including antenatal screening and postpartum care … in their medical history prior to the index date or within 10 years after the index date; age between 12 and 45 years at index date; and no diagnosis of depression, anxiety disorder, adjustment disorder, or somatoform disorder prior to the index date. After applying similar inclusion criteria, women who had had live births were matched (1:1) to those who had had induced abortions by age, index year, and physician. The index date for the live birth group was a randomly selected visit between January 2007 and December 2016….
This retrospective cohort study, including more than 35000 women followed in gynecological practices in Germany, found that the incidence of depression and somatoform disorder was higher in those with induced abortions than in those with live births. Cox regression models further showed that induced abortion was associated with depression, adjustment disorder, and somatoform disorder.
CALCULATION: 17,581 + 17,581 = 35,162
[192] Paper: “Relationship Between Induced Abortion and the Incidence of Depression, Anxiety Disorder, Adjustment Disorder, and Somatoform Disorder in Germany.” By Louis Jacob and others. Journal of Psychiatric Research, July 2019. Pages 75–79. <www.sciencedirect.com>
Page 76:
This study included 17581 women who had had induced abortions and 17581 women who had had live births. The mean age was 32.7 (SD 5.4) years, and 24.0% of the population was aged between 26 and 30 years…. Within 10 years of the induced abortion or live birth, 6.7% of the women who had had induced abortions and 5.4% of those who had had live births were diagnosed with depression (log-rank p-value = 0.003). … Induced abortion was positively associated with depression (hazard ratio [HR] = 1.34; 95% confidence interval [CI]: 1.11–1.64), adjustment disorder … and somatoform disorder … but not with anxiety disorder….
[193] Paper: “Relationship Between Induced Abortion and the Incidence of Depression, Anxiety Disorder, Adjustment Disorder, and Somatoform Disorder in Germany.” By Louis Jacob and others. Journal of Psychiatric Research, July 2019. Pages 75–79. <www.sciencedirect.com>
Page 76:
This study included 17581 women who had had induced abortions and 17581 women who had had live births. The mean age was 32.7 (SD 5.4) years, and 24.0% of the population was aged between 26 and 30 years…. Within 10 years of the induced abortion or live birth, 6.7% of the women who had had induced abortions and 5.4% of those who had had live births were diagnosed with depression…. The respective figures were 3.4% and 2.7% for anxiety disorder (log-rank p-value = 0.255)…. Induced abortion was positively associated with depression … adjustment disorder … and somatoform disorder … but not with anxiety disorder (HR = 1.17; 95% CI: 0.89–1.54).
[194] Paper: “Relationship Between Induced Abortion and the Incidence of Depression, Anxiety Disorder, Adjustment Disorder, and Somatoform Disorder in Germany.” By Louis Jacob and others. Journal of Psychiatric Research, July 2019. Pages 75–79. <www.sciencedirect.com>
Page 76:
This study included 17581 women who had had induced abortions and 17581 women who had had live births. The mean age was 32.7 (SD 5.4) years, and 24.0% of the population was aged between 26 and 30 years…. Within 10 years of the induced abortion or live birth, 6.7% of the women who had had induced abortions and 5.4% of those who had had live births were diagnosed with depression…. The respective figures were 6.2% and 5.6% for adjustment disorder (log-rank p-value = 0.116)…. Induced abortion was positively associated with depression … adjustment disorder (HR = 1.45; 95% CI: 1.19–1.76) and somatoform disorder … but not with anxiety disorder….
[195] Webpage: “Adjustment Disorders.” Johns Hopkins Medicine. Accessed September 26, 2023 at <www.hopkinsmedicine.org>
An adjustment disorder is an emotional or behavioral reaction to a stressful event or change in a person’s life. The reaction is considered an unhealthy or excessive response to the event or change within three months of it happening. Stressful events or changes in the life of your child or adolescent may be a family move, the parents’ divorce or separation, the loss of a pet, or the birth of a sibling. A sudden illness or restriction to your child’s life due to chronic illness may also result in an adjustment response.
While adults can experience adjustment disorders, it is predominantly diagnosed in children and adolescents.
[196] Paper: “Relationship Between Induced Abortion and the Incidence of Depression, Anxiety Disorder, Adjustment Disorder, and Somatoform Disorder in Germany.” By Louis Jacob and others. Journal of Psychiatric Research, July 2019. Pages 75–79. <www.sciencedirect.com>
Page 76:
This study included 17581 women who had had induced abortions and 17581 women who had had live births. The mean age was 32.7 (SD 5.4) years, and 24.0% of the population was aged between 26 and 30 years…. Within 10 years of the induced abortion or live birth, 6.7% of the women who had had induced abortions and 5.4% of those who had had live births were diagnosed with depression…. The respective figures were … 19.3% and 13.3% for somatoform disorder (log-rank p-value < 0.001). … Induced abortion was positively associated with depression … adjustment disorder … and somatoform disorder (HR = 1.56; 95% CI: 1.38–1.76), but not with anxiety disorder….
[197] Article: “Somatoform Disorders.” By Oliver Oyama and others. American Family Physician, November 1, 2007. <www.aafp.org>
The somatoform disorders are a group of psychiatric disorders that cause unexplained physical symptoms. They include somatization disorder (involving multisystem physical symptoms), undifferentiated somatoform disorder (fewer symptoms than somatization disorder), conversion disorder (voluntary motor or sensory function symptoms), pain disorder (pain with strong psychological involvement), hypochondriasis (fear of having a life-threatening illness or condition), body dysmorphic disorder (preoccupation with a real or imagined physical defect), and somatoform disorder not otherwise specified (used when criteria are not clearly met for one of the other somatoform disorders). These disorders should be considered early in the evaluation of patients with unexplained symptoms to prevent unnecessary interventions and testing. Treatment success can be enhanced by discussing the possibility of a somatoform disorder with the patient early in the evaluation process, limiting unnecessary diagnostic and medical treatments, focusing on the management of the disorder rather than its cure, using appropriate medications and psychotherapy for comorbidities, maintaining a psychoeducational and collaborative relationship with patients, and referring patients to mental health professionals when appropriate.
The somatoform disorders are a group of psychiatric disorders in which patients present with a myriad of clinically significant but unexplained physical symptoms. They include somatization disorder, undifferentiated somatoform disorder, hypochondriasis, conversion disorder, pain disorder, body dysmorphic disorder, and somatoform disorder not otherwise specified.1 These disorders often cause significant emotional distress for patients and are a challenge to family physicians.
[198] Paper: “Relationship Between Induced Abortion and the Incidence of Depression, Anxiety Disorder, Adjustment Disorder, and Somatoform Disorder in Germany.” By Louis Jacob and others. Journal of Psychiatric Research, July 2019. Pages 75–79. <www.sciencedirect.com>
Page 78:
The two major strengths of this study are the number of women available for analysis and the use of real-world data from gynecological practices where diagnoses are continuously documented, allowing for unbiased exposure assessment (no recall bias). Nonetheless, the results of the present study should be interpreted in the light of several limitations. Firstly, diagnoses relied on ICD 10 codes only, and there was no information on the severity of the psychiatric disorders examined. Secondly, psychiatric disorders may have been insufficiently documented by gynecologists, leading to an underestimation of depression, anxiety disorder, adjustment disorder, and somatoform disorder. Thirdly, we had no data on factors known to have a significant impact on mental health (e.g., loneliness, social support, alcohol use), and this may have biased our findings. Finally, this was a retrospective study, and it was thus not possible to determine causality or temporality in the association between induced abortion and psychiatric disorders.
[199] Paper: “Randomised Controlled Trials – the Gold Standard for Effectiveness Research.” By Eduardo Hariton & Joseph J Locascio. BJOG (British Journal of Obstetrics & Gynecology), June 19, 2018. <obgyn.onlinelibrary.wiley.com>
Randomised controlled trials (RCTs) are the reference standard for studying causal relationships between interventions and outcomes as randomisation eliminates much of the bias inherent with other study designs. …
RCTs are prospective studies that measure the effectiveness of interventions. Although no study is likely on its own to prove causality, randomisation reduces bias and provides a rigorous tool to examine cause–effect relationships between an intervention and outcome. This is because the act of randomisation in a large study balances participant characteristics (both observed and unobserved) between the groups, allowing attribution of any differences in outcome to the intervention. This is not possible with any other study design, so RCTs are considered the reference standard for driving practice….
[200] Book: Regression With Social Data: Modeling Continuous and Limited Response Variables. By Alfred DeMaris. John Wiley & Sons, 2004.
Page 9:
Regression modeling of nonexperimental data for the purpose of making causal inferences is ubiquitous in the social sciences. Sample regression coefficients are typically thought of as estimates of the causal impacts of explanatory variables on the outcome. Even though researchers may not acknowledge this explicitly, their use of such language as impact or effect to describe a coefficient value often suggest a causal interpretation. This practice is fraught with controversy….
Page 12:
Friedman … is especially critical of drawing causal inferences from observational data, since all that can be “discovered,” regardless of the statistical candlepower used, is association. Causation has to be assumed into the structure from the beginning. Or, as Friedman … says: “If you want to pull a causal rabbit out of the hat, you have to put the rabbit into the hat.” In my view, this point is well taken; but it does not preclude using regression for causal inference. What it means, instead, is that prior knowledge of the causal status of one’s regressors is a prerequisite for endowing regression coefficients with a causal interpretation, as acknowledged by Pearl 1998.
Page 13: “In sum, causal modeling via regression, using nonexperimental data, can be a useful enterprise provided we bear in mind that several strong assumptions are required to sustain it. First, regardless of the sophistication of our methods, statistical techniques only allow us to examine associations among variables.”
[201] Article: “Late-Term Elective Abortion and Susceptibility to Posttraumatic Stress Symptoms.” By Priscilla K. Coleman and others. Journal of Pregnancy, June 28, 2010. <www.hindawi.com>
Page 2: “Finally, women who seek late-term abortions (after 16 weeks) are significantly more likely to be under age 18, Black, unemployed, and/or poor11.”
[202] Paper: “Late-Term Abortion.” By Janet E. Gans Epner and others. Journal of the American Medical Association, August 26, 1998. Pages 724–729. <jamanetwork.com>
Page 724:
Definitions of Trimesters and Viability
In this article, early second-trimester abortion procedures refer to those performed at 13 through 15 weeks of gestation. Mid second-trimester abortion procedures are those performed at 16 through 19 weeks of gestation. Late second-trimester abortions refer to procedures performed at 20 through 27 weeks of gestation. Late-term abortions refer to procedures performed during the third trimester, defined as 27 weeks of gestation or more. Weeks of gestation are defined in terms of the first day of the last menstrual period. However, gestational age may vary depending on whether the stage of pregnancy is calculated from the first day of the last menstrual period, from the estimated time of fertilization, or from the estimated time of implementation.3,4 Such distinctions are important when regulations or legal provisions refer to weeks of gestation or trimesters.
[203] Paper: “Late-Term Abortion for Fetal Anomaly: Vietnamese Women’s Experiences.” By Tine Gammeltoft and others. Reproductive Health Matters, September 2008. Pages 46–56. <www.tandfonline.com>
Page 47: “This article focuses on 17 women who had a late-term abortion due to a fetal malformation….”
Page 48: “The 17 pregnancies were terminated at varying stages of gestation: two women were at 14–18 weeks, eight at 19–24 weeks, five at 25–30 weeks and two at 32–35 weeks.”
[204] Article: “Health Law: Legislative Restrictions on Abortion.” By B. Jessie Hill. Virtual Mentor, American Medical Association Journal of Ethics, February 2012. <journalofethics.ama-assn.org>
Page 133: “[S]he was neither a patient seeking a late-term abortion nor a doctor who performs them, and therefore she was not directly affected by the law7.”
[205] Webpage: “Abortion Services.” Boulder Abortion Clinic, Accessed October 29, 2020 at <www.drhern.com>
Boulder Abortion Clinic offers the following abortion services
• First Trimester Abortion up to 13 Weeks
• Second Trimester Abortion up to 26 Weeks
• Third Trimester Abortion (commonly known as late term abortion) over 26 Weeks …
[206] Paper: “State Actions on Reproductive Health Issues in 1996.” By Terry Sollom. Perspectives on Sexual and Reproductive Health, January/February 1997. Pages 35–40. <www.guttmacher.org>
Page 39:
Antiabortion activists have vowed to pursue legislative bans on D&X [dilation and extraction] abortions with even greater intensity in 1997, which undoubtedly will lead to wide-ranging discussions and actions on late-term abortions, opening floodgates that may prove very difficult to close. This could be the case particularly if moderate lawmakers continue to express misgivings about the availability of abortion late in pregnancy.
[207] Article: “Abortion Restrictions and the Drive for Mental Health Parity: A Conflict in Values?” By Cynthia Dailard. Guttmacher Policy Review, June 1999. <www.guttmacher.org>
Page 5:
Just over one year later, in September 1998, Sen. Dick Durbin (D-IL), another consistent supporter of reproductive rights, went a step further. With a bipartisan group of prochoice senators, he introduced the Late-Term Abortion Limitation Act, which incorporates Daschle’s proposal, including its distinction between physical and mental health conditions, but adds another requirement—that a second physician, not involved in performing the abortion, be consulted to certify that the reason for the abortion meets the narrow requirements of the bill.
[208] Paper: “Prenatal Testing for Down Syndrome: Comparison of Screening Practices in the UK and USA.” By Dagmar Tapon. Journal of Genetic Counseling, April 2010. Pages 112–130. <onlinelibrary.wiley.com>
“In the USA, late-term abortions were often carried out through ‘intact dilatation and extraction’, a procedure called ‘partial birth abortion’ by the anti-abortion community…. A ban on ‘partial birth abortion’ in 2003 by President George W Bush and upheld in 2007 by the US Supreme Court leaves few safe alternatives for third trimester abortion according to the American College of Obstetrics and Gynecology….”
[209] Paper: “Infant Mortality Rate as a Measure of a Country’s Health: A Robust Method to Improve Reliability and Comparability.” By Robert M. Gonzalez and Donna Gilleskie. Demography, April 2017. Pages 701–720. <www.ncbi.nlm.nih.gov>
Page 704:
Definitions …
The late fetal period begins at 22 completed weeks of gestation (or at a weight of the fetus of 500 grams) and ends at birth. The early neonatal period begins at birth of the fetus and covers the first seven days after birth. The perinatal period encompasses both the late fetal and early neonatal periods. The infant period spans the first year after birth. Mortality rates are defined by the number of deaths occurring in a particular period and the number of live births.
Page 707:
An additional possibility may be that Cuba may count late term abortions (LTAs) as part of late fetal deaths, which would lead to substantially higher levels of late fetal deaths given Cuba’s high abortion rates.16
[210] Webpage: “Anniversary of the Murder of Dr. George Tiller.” Planned Parenthood, May 31, 2017. <www.plannedparenthood.org>
“Tiller cared for women having to make some of the most difficult decisions a woman can make, including late-term abortion services.”
[211] Article: “Abortion Pros and Cons Gain Emotional Weight.” By Francis X. Clines. New York Times, November 8, 1995. <www.nytimes.com>
“But her fury became clear as the Senate began debating the proposed banning and criminalization of the very sort of late-term abortion procedure she found herself requiring.”
[212] Article: “The Reincarnation of Pro-Life.” By Emily Bazelon (Yale Law School). New York Times Magazine, May 27, 2011. <www.nytimes.com>
“In a 2007 poll, Gallup found that twice as many people favor making late-term abortion illegal than favor overturning Roe (72 percent versus 35 percent).”
[213] Article: “Michigan Judge Allows Incest Victim to Seek Late-Term Abortion.” By Linda Perlstein. Washington Post, July 25, 1998. <www.washingtonpost.com>
“The decision appeared to end at least the legal part of a drama that for a brief moment served as a nexus for issues—late-term abortions and crossing state lines to escape restrictive laws—that have fueled the abortion debate in Congress and around the country.”
[214] Article: “Harsh Details Shift Tenor of Abortion Fight; Both Sides Bend Facts On Late-Term Procedure.” By Barbara Vobejda & David Brown. Washington Post, September 17, 1996. Page A01. <www.washingtonpost.com>
“A contentious subtext in this war of images has been the question of why women seek late-term abortions.”
[215] Webpage: “House Passes Late-Term Abortion Ban.” By Pete Kasperowicz. The Hill, June 18, 2013. <thehill.com>
“The House voted Tuesday to impose a nationwide ban on abortions after 22 weeks of pregnancy over Democratic objections that the bill represents a dramatic attempt by Republicans to restrict abortion rights.”
[216] Twitter post: “Incredibly Moving Piece on the Realities of Late-Term Abortion for Families.” By Planned Parenthood Action, February 7, 2014. <twitter.com>
“Incredibly moving piece on the realities of late-term abortion for families, and why it matters right now”
[217] Webpage: “Late-Term Abortion Care For Maternal/Fetal Indications.” Capital Women’s Group. Accessed September 20, 2023 at <www.capitalwomensservices.com>
“Capital Women’s Group offers late-term abortion care up to 36 weeks under certain circumstances, such as for fetal or maternal indications. All requests for late-term abortion care are handled on a case-by-case basis after consultation with our clinicians.”
[218] Webpage: “Late-Term Abortion Care Colorado.” Clinics for Abortion & Reproductive Excellence. Accessed September 20, 2023 at <abortionclinics.org>
“Founded May 1, 1992 by LeRoy and Mary Lou Carhart, our mission is to provide late term abortions in Colorado…. We provide assistance to women in Colorado with late term abortions, third trimester abortions, abortion after 27 weeks, maternal indication abortions, fetal indication abortions, and birth control.”
[219] Webpage: “A Conversation with Faye Wattleton: Part 1, Historical Perspectives.” Planned Parenthood Advocates of Arizona, February 4, 2013. <advocatesaz.org>
“The [most] significant erosion is this court’s willingness to uphold a law that could ignore a woman’s health in making the decision to permit a late-term abortion.”
[220] Paper: “Who Seeks Abortions at or After 20 Weeks.” By Diana Greene Foster. Perspectives on Sexual and Reproductive Health, December 2013. Pages 210–218. <onlinelibrary.wiley.com>
Page 210:
The considerable majority of abortions (91%) take place in the first trimester, before the end of the 13th week of pregnancy; 7% are performed at 14–20 weeks, and 1% at 21 weeks or later.4 Nonetheless, this final category constitutes a substantial number of abortions: Given an estimated 1.21 million abortions in the United States annually,5 more than 15,000 likely take place after 20 weeks.
[221] Webpage: “Perspectives on Sexual and Reproductive Health: A Journal of Peer-Reviewed Research.” Guttmacher Institute. Accessed October 30, 2023 at <www.guttmacher.org>
“Perspectives on Sexual and Reproductive Health (1969–2020) published peer-reviewed, policy-relevant research and analysis on sexual and reproductive health and rights in the United States and other high-income countries.”
[222] Webpage: “The Guttmacher Institute’s Future.” Guttmacher Institute Board of Directors, June 23, 2005. <www.guttmacher.org>
Guiding Principles …
The Institute works to protect, expand and equalize access to information, services and rights that will enable women and men to
• avoid unplanned pregnancies;
• prevent and treat sexually transmitted infections, including HIV [human immunodeficiency virus];
• exercise the right to choose abortion;
• achieve healthy pregnancies and births; and
• have healthy, satisfying sexual relationships.
[223] Paper: “Who Seeks Abortions at or After 20 Weeks.” By Diana Greene Foster. Perspectives on Sexual and Reproductive Health, December 2013. Pages 210–218. <onlinelibrary.wiley.com>
Page 210:
Causes of delay in obtaining abortion were assessed in open- and closed-ended questions; profiles of women who received later abortions were identified through factor analysis. …
The considerable majority of abortions (91%) take place in the first trimester, before the end of the 13th week of pregnancy; 7% are performed at 14–20 weeks, and 1% at 21 weeks or later.4 Nonetheless, this final category constitutes a substantial number of abortions: Given an estimated 1.21 million abortions in the United States annually,5 more than 15,000 likely take place after 20 weeks.
[224] Paper: “Who Seeks Abortions at or After 20 Weeks.” By Diana Greene Foster. Perspectives on Sexual and Reproductive Health, December 2013. Pages 210–218. <onlinelibrary.wiley.com>
Page 210:
Recent years have seen the introduction of state bills seeking to ban abortions after 20 weeks.1 …
1 Guttmacher Institute, State policies on later abortions, State Policies in Brief (as of October 1, 2013), 2012, <www.guttmacher.org>, accessed Oct. 8, 2013.Ӡ
NOTE: † The fact that this paper measures pregnancy from the last menstrual period is evidenced by the fact that it begins by citing the Guttmacher webpage above, which insists on this reckoning: As of January 1, 2019, this webpage stated: “Dating a pregnancy from fertilization goes against convention. When discussing pregnancy, medical professionals customarily date a pregnancy from the first day of the woman’s last menstrual period, because that is the date most women can pinpoint.”
[225] Book: Color Atlas of Life Before Birth. By Marjorie A. England. Year Book Medical Publishers, 1983.
Page 12: “Most clinicians do not know the fertilization date; the only date available to them is the first day of the last menstrual period. They use this date to define a menstrual age stretching from time 0, which is usually 14 days before fertilization….”
[226] Paper: “Pain and its Effects in the Human Neonate and Fetus.” By K.J.S. Anand & P.R. Hickey. New England Journal of Medicine, November 19, 1987. Pages 1321–1329. <www.nejm.org>
Page 1322:
Cutaneous sensory receptors appear in the perioral [mouth] area of the human fetus in the 7th week of gestation; they spread to the rest of the face, the palms of the hands and the soles of the feet by the 11th week, to the trunk and proximal parts of the arms and legs by the 15th week, and to all cutaneous and mucous surfaces by the 20th week. …
Development of the fetal neocortex begins at 8 weeks of gestation, and by 20 weeks each cortex has a full complement of 109 neurons.
NOTE: This article uses the obstetric method of counting from the last menstrual period as evidenced by the chart on page 1322, which uses a gestation of 40 weeks for pregnancy. Two weeks must be subtracted to provide the actual time since fertilization.
[227] Article: “Fetus.” By Frank D. Allan. Encyclopedia of Human Biology (Volume 3). Academic Press, 1997.
Pages 954–955:
B. Early Fetal Period (Third Month) …
Division of the heart into chambers is complete, and a definitive vascular system carries blood to and from all body parts. …
All components of the brain and the spinal cord are formed, and nerves link the stem of the brain and the spinal cord to all tissues and organs of the body.
[228] Article: “Fetus.” By Frank D. Allan. Encyclopedia of Human Biology (Volume 3). Academic Press, 1997.
Page 962:
Attempts to suckle have been seen in utero and in aborted fetuses of 3 months. …
Reflexes that develop during the third month involve the mouth and the head…. Electrical activity of the nervous system is discernible at the same time, but periods of electrical silence can occur up to midterm.
[229] Article: “Wired to Be Social: The Ontogeny of Human Interaction.” By Umberto Castiello and others. PLoS ONE, October 7, 2010. <journals.plos.org>
Page 2: “The results showed that the spatial and temporal characteristics of foetal movements were by no means uncoordinated, but depended on the goal of the different motor acts, suggesting a surprisingly advanced level of motor planning.”
Page 3:
Each woman was identified by the prenatal sonologist during her first visit at the 12th week of pregnancy and foetal age was calculated comparing the mother’s last menstruation date and the measurements of the foetus (Crown Rump Length) taken during the ultrasound examination.
Page 9:
Twin pregnancies constitute an experiment of nature which offers the unique opportunity to explore social behaviour before birth. By investigating kinematic profiles of movements in five pairs of twin foetuses, we demonstrated that, by the 14th week of gestation, twin foetuses not only display movements directed towards the uterine wall and self-directed movements, but also movements specifically aimed at the co-twin. …
Analysis of the kinematic profiles for the different categories of movements corroborates our main hypothesis that these early contacts do not occur accidentally, but reflect motor planning.
Page 10:
In this article we describe changes in the kinematic profiles of movement in twin foetuses probing the social dimension of motor planning and control. The central advance of this study is the demonstration that ‘social actions’ are already performed in the second trimester of gestation. Starting from the 14th week of gestation twin foetuses plan and execute movements specifically aimed at the co-twin. These findings force us to predate the emergence of social behaviour: when the context enables it, as in the case of twin foetuses, other-directed actions are not only possible but predominant over self-directed actions.
NOTE: This article uses the obstetric method of counting from the last menstrual period as evidenced by the statement that “foetal age was calculated” based on the “mother’s last menstruation date.” Thus, two weeks must be subtracted to provide the actual time since fertilization.
[230] Textbook: Before We Are Born: Essentials of Embryology and Birth Defects (5th edition). By Keith L. Moore & T.V.N. Persaud. W.B. Saunders Company, 1998.
Page 106: “Limb movements, which occur at the end of the embryonic period (8 weeks), become coordinated by the 14th week, but are too slight to be felt by the mother.”
[231] Paper: “Fetal and Maternal Analgesia/Anesthesia for Fetal Procedures.” By Marc Van de Velde and Frederik De Buck. Fetal Diagnosis and Therapy, April 25, 2012. Pages 201–209. <www.karger.com>
Page 206: “Whether a fetus is capable of experiencing pain as a conscious and emotional feeling remains unclear and is subject to great debate,67 but we cannot deny that the fetal nervous system mounts protective responses to tissue injury. A physiological fetal reaction to painful stimuli occurs from between 16 and 24 weeks’ gestation on.”
[232] Paper: “Pain and its Effects in the Human Neonate and Fetus.” By K.J.S. Anand & P.R. Hickey. New England Journal of Medicine, November 19, 1987. Pages 1321–1329. <www.nejm.org>
Page 1322:
Cutaneous sensory receptors appear in the perioral [mouth] area of the human fetus in the 7th week of gestation; they spread to the rest of the face, the palms of the hands and the soles of the feet by the 11th week, to the trunk and proximal parts of the arms and legs by the 15th week, and to all cutaneous and mucous surfaces by the 20th week. …
Development of the fetal neocortex begins at 8 weeks of gestation, and by 20 weeks each cortex has a full complement of 109 neurons.
NOTE: This article uses the obstetric method of counting from the last menstrual period as evidenced by the chart on page 1322, which uses a gestation of 40 weeks for pregnancy. Two weeks must be subtracted to provide the actual time since fertilization.
[233] Paper: “Effect of Direct Fetal Opioid Analgesia on Fetal Hormonal and Hemodynamic Stress Response to Intrauterine Needling.” By Nicholas M. Fisk and others. Anesthesiology, October 2001. Pages 828–835. <pubs.asahq.org>
Page 828: “Our group has shown that the human fetus from 18–20 weeks elaborates pituitary-adrenal, sympatho-adrenal, and circulatory stress responses to physical insults.”
[234] Article: “Fetus.” American Medical Association Complete Medical Encyclopedia. Random House, 2003.
Page 558: “At 20 weeks, the fetus is 10 inches long and about 11 ounces. The limbs have lengthened, and teeth and hair are beginning to form. The fetus now sleeps and wakes and hears sounds.”
[235] Intrauterine picture taken at 20 weeks after fertilization under the direction of Professor Andrzej Skawina of Collegium Medicum Jagiellonian University (Krakow, Poland) and Antoni Marsinek of the Czerwiakowski Gynecological and Obstetrics Hospital (Krakow, Poland); Photographers: Andrzej Zachwieja and Jan Walczewski. Copyright: Life Issues.
NOTE: A number of different photographers have published intrauterine photos. Just Facts asked several of these individuals for permission to reproduce their pictures, and Life Issues was the only one who consented. The pictures from Life Issues look similar to those taken by the other photographers.
[236] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] VIII:
Specific and direct harm medically diagnosable even in early pregnancy may be involved. Maternity, or additional offspring, may force upon the woman a distressful life and future. Psychological harm may be imminent. Mental and physical health may be taxed by child care. There is also the distress, for all concerned, associated with the unwanted child, and there is the problem of bringing a child into a family already unable, psychologically and otherwise, to care for it. In other cases, as in this one, the additional difficulties and continuing stigma of unwed motherhood may be involved. All these are factors the woman and her responsible physician necessarily will consider in consultation.
[Section] XI:
For the stage subsequent to viability the State, in promoting its interest in the potentiality of human life, may, if it chooses, regulate, and even proscribe, abortion except where necessary, in appropriate medical judgment, for the preservation of the life or health of the mother. …
In Doe v. Bolton, post, p. 179, procedural requirements contained in one of the modern abortion statutes are considered. That opinion and this one, of course, are to be read together.
[237] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] IV: “[T]he medical judgment may be exercised in the light of all factors—physical, emotional, psychological, familial, and the woman’s age—relevant to the wellbeing of the patient. All these factors may relate to health.”
[238] Ruling: Planned Parenthood of Southeastern PA v. Casey. United States Supreme Court. June 29, 1992. <caselaw.findlaw.com>
Majority:
It must be stated at the outset and with clarity that Roe’s essential holding, the holding we reaffirm, has three parts. First is a recognition of the right of the woman to choose to have an abortion before viability and to obtain it without undue interference from the State. Before viability, the State’s interests are not strong enough to support a prohibition of abortion or the imposition of a substantial obstacle to the woman’s effective right to elect the procedure. Second is a confirmation of the State’s power to restrict abortions after fetal viability if the law contains exceptions for pregnancies which endanger the woman’s life or health. And third is the principle that the State has legitimate interests from the outset of the pregnancy in protecting the health of the woman and the life of the fetus that may become a child.
[239] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] IV:
D. The appellants next argue that the District Court should have declared unconstitutional three procedural demands of the Georgia statute: (1) that the abortion be performed in a hospital accredited by the Joint Commission on Accreditation of Hospitals:11 (2) that the procedure be approved by the hospital staff abortion committee; and (3) that the performing physician’s judgment be confirmed by the independent examinations of the patient by two other licensed physicians. …
We hold that the JCAH-accreditation [Joint Commission on Accreditation of Hospitals] requirement does not withstand constitutional scrutiny in the present context. …
We conclude that the interposition of the hospital abortion committee is unduly restrictive of the patient’s rights and needs that, at this point, have already been medically delineated and substantiated by her personal physician. …
There remains, however, the required confirmation by two Georgia-licensed physicians in addition to the recommendation of the pregnant woman’s own consultant (making under the statute, a total of six physicians involved, including the three on the hospital’s abortion committee). We conclude that this provision, too, must fall.
The statute’s emphasis, as has been repetitively noted, is on the attending physician’s “best clinical judgment that an abortion is necessary.” That should be sufficient. The reasons for the presence of the confirmation step in the statute are perhaps apparent, but they are insufficient to withstand constitutional challenge. … If a physician is licensed by the State, he is recognized by the State as capable of exercising acceptable clinical judgment.
[240] Article: “Daschle Bill May Not Ban Anything; Abortionists Could Use Own Judgment.” By Frank J. Murray. Washington Times, May 15, 1997. <www.washingtontimes.com>
… Dr. Warren Hern, who literally wrote the textbook on “Abortion Practice.”
The Denver gynecologist said the fact of occasional death in childbearing can justify any abortion, no matter how late it is done.
“I will certify that any pregnancy is a threat to a woman’s life and could cause ‘grievous injury’ to her ‘physical health,’ ” Dr. Hern said, using key words from the Daschle bill….
[241] Webpage: “States with Gestational Limits for Abortion (As of August 1, 2020).” Kaiser Family Foundation. Accessed June 22, 2021 at <bit.ly>
|
Location |
State Imposed Threshold for Abortions Later in Pregnancy |
Abortions Later in Pregnancy Permitted When Pregnancy Threatens Woman’s: |
|
Alabama |
22 weeks LMP |
Life and physical health |
|
Arkansas |
22 weeks LMP |
Life and physical health |
|
Florida |
24 weeks LMP |
Life and physical health |
|
Georgia |
22 weeks LMP |
Life and physical health |
|
Indiana |
22 weeks LMP |
Life and physical health |
|
Iowa |
22 weeks LMP |
Life and physical health |
|
Kansas |
22 weeks LMP |
Life and physical health |
|
Kentucky |
22 weeks LMP |
Life and physical health |
|
Louisiana |
22 weeks LMP |
Life and physical health |
|
Massachusetts |
24 weeks LMP |
Life and health |
|
Mississippi |
20 weeks LMP |
Life and physical health |
|
Nebraska |
22 weeks LMP |
Life and physical health |
|
Nevada |
24 weeks LMP |
Life and health |
|
North Carolina |
20 weeks LMP |
Life and physical health |
|
North Dakota |
22 weeks LMP |
Life and physical health |
|
Ohio |
22 weeks LMP |
Life and physical health |
|
Oklahoma |
22 weeks LMP |
Life and physical health |
|
Pennsylvania |
24 weeks LMP |
Life and physical health |
|
South Carolina |
22 weeks LMP |
Life and physical health |
|
South Dakota |
22 weeks LMP |
Life and physical health |
|
Texas |
22 weeks LMP |
Life and physical health |
|
Virginia |
3rd trimester |
Life and health |
|
West Virginia |
22 weeks LMP |
Life and physical health |
|
Wisconsin |
22 weeks LMP |
Life and physical health |
Notes
The U.S. Supreme Court has held that states may constitutionally ban or restrict abortions after the point of fetal viability except where necessary to preserve a woman’s life or health.
The exception of “physical health” permits abortions when the woman suffers from a “substantial and irreversible impairment of a major bodily function.”
[242] Article: “The Reincarnation of Pro-Life.” By Emily Bazelon (Yale Law School). New York Times Magazine, May 27, 2011. <www.nytimes.com>
… Terry O’Neill, president of NOW [National Organization for Women]—told her that people on their side were gun shy, afraid to bring a suit that could end up in the Supreme Court and thus test Justice Anthony Kennedy. Two decades ago, Kennedy was crucial to the 5-to-4 watershed decision to uphold Roe in Planned Parenthood v. Casey. But that was before Samuel Alito, an abortion opponent, replaced Sandra Day O’Connor, one of Kennedy’s co-authors in Casey. …
[L]itigators trying to uphold a woman’s right to an abortion are not running scared….
The bait that they have been wise to avoid involves the prohibition of abortion after 20 or 22 weeks of pregnancy. … If the abortion rights groups were to sue, they would risk returning to dangerous political ground. …
In a 2007 poll, Gallup found that twice as many people favor making late-term abortion illegal than favor overturning Roe (72 percent versus 35 percent).
[243] Article: “Harsh Details Shift Tenor of Abortion Fight; Both Sides Bend Facts On Late-Term Procedure.” By Barbara Vobejda & David Brown. Washington Post, September 17, 1996. Page A01. <www.washingtonpost.com>
“The usual alternative to intact D&E [dilation and evacuation] is ‘dismemberment D&E,’ in which the fetal limbs are pulled off the body in utero, sometimes while the fetus is still alive.”
[244] Paper: “Fetal Pain: Implications for Research and Practice.” By Vivette Glover and Nicholas M. Fisk. British Journal of Obstetrics & Gynaecology, August 19, 2005. Pages 881–886. <onlinelibrary.wiley.com>
Page 884: “Late terminations may cause pain to the fetus if they involve an invasive procedure, such as surgical dismemberment.”
[245] Paper: “Fetal Plasma Cortisol and Beta-Endorphin Response to Intrauterine Needling.” By X. Giannakoulopoulos and others. Lancet, July 9, 1994. Pages 77–81. <www.thelancet.com>
Page 80:
Just as physicians now provide neonates with adequate analgesia,5 our findings suggest that those dealing with the fetus should consider making similar modifications to their practice. This applies not just to diagnostic and therapeutic procedures on the fetus, but possibly also to termination of pregnancy, especially by surgical techniques involving dismemberment.
5 Rogers, MC. Do the Right Thing: Pain Relief in Infants and Children. New England Journal of Medicine 1992; 326: 55–56.
[246] Presentation: “Dilation and Extraction for Late Second Trimester Abortion.” By Martin Haskell. National Abortion Federation, September 13, 1992. <operationrescue.org>
Page 1:
The surgical method described in this paper [partial-birth abortion] differs from classic D&E [dilation and evacuation] in that it does not rely upon dismemberment to remove the fetus. Nor are inductions or infusions used to expel the intact fetus.
Rather, the surgeon grasps and removes a nearly intact fetus through an adequately dilated cervix. The author has coined the term Dilation and Extraction or D&X to distinguish it from dismemberment-type D&E’s.
[247] Article: “The Facts on Partial-Birth Abortion; Both Sides Have Misled the Public.” By Ruth Padawer. Bergen Record, September 15, 1996. <northjersey.newspapers.com>
Doctors at Metropolitan Medical in Englewood estimate that their clinic alone performs 3,000 abortions a year on fetuses between 20 and 24 weeks, of which at least half are by intact dilation and evacuation [D&E]. …
“I always try an intact D&E first,” said a Metropolitan Medical gynecologist, who, like every other provider interviewed for this article, spoke on condition of anonymity for fear of retribution. If the fetus isn’t breech, or if the cervix isn’t dilated enough, providers switch to traditional, or “classic,” D&E, in utero dismemberment.
[248] Ruling: West Alabama Women’s Center v. Miller. U.S. Court of Appeals for the Eleventh Circuit. August 22, 2018. Decided 3–0. Majority: Carnes, Dubina. Concurring: Abrams. <media.ca11.uscourts.gov>
Ed Carnes, Chief Judge: “This case involves a method of abortion that is clinically referred to as Dilation and Evacuation (D & E). Or dismemberment abortion, as the State less clinically calls it. That name is more accurate because the method involves tearing apart and extracting piece-by-piece from the uterus what was until then a living unborn child.”
[249] Article: “2nd Trimester Abortion: An Interview with W. Martin Haskell, MD.” Cincinnati Medicine, Fall 1993. Pages 18–19. <www.nrlc.org>
Page 19:
Q: What led you to develop D & X [dilation and extraction]?
A: D & E’s [dilation and evacuations], the procedure typically used for later abortions, have always been somewhat problematic because of the toughness and development of the fetal tissues. Most physicians do terminations after 20 weeks by saline infusion or prostaglandin induction, which terminates the fetus and allows tissue to soften.
[250] Ruling: West Alabama Women’s Center v. Miller. U.S. Court of Appeals for the Eleventh Circuit. August 22, 2018. Decided 3–0. Majority: Carnes, Dubina. Concurring: Abrams. <media.ca11.uscourts.gov>
Ed Carnes, Chief Judge:
Nearly 93% of abortions performed in Alabama occur before 15 weeks, at which time dismemberment abortion is unnecessary because the unborn child is small enough for practitioners to use other methods that the Act does not prohibit. For the 7% of abortions that occur after 15 weeks, 99% of them are by dismemberment. That’s because at that later stage of pregnancy dismemberment abortion is simpler and safer than other methods, with major complications arising less than 1% of the time.
[251] Ruling: Gonzales v. Carhart. United States Supreme Court, April 18, 2007. Decided 5–4. Majority: Kennedy, Roberts, Scalia, Thomas, Alito. Concurring: Thomas, Scalia. Dissenting: Ginsburg, Stevens, Souter, Breyer. <caselaw.findlaw.com>
Majority:
[Section] I (A): …
Of the remaining abortions that take place each year, most occur in the second trimester. The surgical procedure referred to as “dilation and evacuation” or “D&E” is the usual abortion method in this trimester. …
After sufficient dilation the surgical operation can commence. The woman is placed under general anesthesia or conscious sedation. The doctor, often guided by ultrasound, inserts grasping forceps through the woman’s cervix and into the uterus to grab the fetus. The doctor grips a fetal part with the forceps and pulls it back through the cervix and vagina, continuing to pull even after meeting resistance from the cervix. The friction causes the fetus to tear apart. For example, a leg might be ripped off the fetus as it is pulled through the cervix and out of the woman. The process of evacuating the fetus piece by piece continues until it has been completely removed. A doctor may make 10 to 15 passes with the forceps to evacuate the fetus in its entirety, though sometimes removal is completed with fewer passes. Once the fetus has been evacuated, the placenta and any remaining fetal material are suctioned or scraped out of the uterus. The doctor examines the different parts to ensure the entire fetal body has been removed. See, e.g., Nat. Abortion Federation, supra, at 465; Planned Parenthood, supra, at 962.
Some doctors, especially later in the second trimester, may kill the fetus a day or two before performing the surgical evacuation. They inject digoxin or potassium chloride into the fetus, the umbilical cord, or the amniotic fluid. Fetal demise may cause contractions and make greater dilation possible. Once dead, moreover, the fetus’ body will soften, and its removal will be easier. Other doctors refrain from injecting chemical agents, believing it adds risk with little or no medical benefit. Carhart, supra, at 907–912; Nat. Abortion Federation, supra, at 474–475.
[252] Ruling: Gonzales v. Carhart. United States Supreme Court, April 18, 2007. Decided 5–4. Majority: Kennedy, Roberts, Scalia, Thomas, Alito. Concurring: Thomas, Scalia. Dissenting: Ginsburg, Stevens, Souter, Breyer. <caselaw.findlaw.com>
Majority:
[Section] I (A): …
Of the remaining abortions that take place each year, most occur in the second trimester. The surgical procedure referred to as “dilation and evacuation” or “D&E” is the usual abortion method in this trimester. …
After sufficient dilation the surgical operation can commence. The woman is placed under general anesthesia or conscious sedation. The doctor, often guided by ultrasound, inserts grasping forceps through the woman’s cervix and into the uterus to grab the fetus. The doctor grips a fetal part with the forceps and pulls it back through the cervix and vagina, continuing to pull even after meeting resistance from the cervix. The friction causes the fetus to tear apart. For example, a leg might be ripped off the fetus as it is pulled through the cervix and out of the woman. The process of evacuating the fetus piece by piece continues until it has been completely removed. A doctor may make 10 to 15 passes with the forceps to evacuate the fetus in its entirety, though sometimes removal is completed with fewer passes. Once the fetus has been evacuated, the placenta and any remaining fetal material are suctioned or scraped out of the uterus. The doctor examines the different parts to ensure the entire fetal body has been removed. See, e.g., Nat. Abortion Federation, supra, at 465; Planned Parenthood, supra, at 962.
Some doctors, especially later in the second trimester, may kill the fetus a day or two before performing the surgical evacuation. They inject digoxin or potassium chloride into the fetus, the umbilical cord, or the amniotic fluid. Fetal demise may cause contractions and make greater dilation possible. Once dead, moreover, the fetus’ body will soften, and its removal will be easier. Other doctors refrain from injecting chemical agents, believing it adds risk with little or no medical benefit. Carhart, supra, at 907–912; Nat. Abortion Federation, supra, at 474–475. …
The main difference between the two procedures is that in [a partial-birth abortion] a doctor extracts the fetus intact or largely intact with only a few passes.
[Section] III (C) 1:
The Act excludes most D&Es [dilation and evacuations] in which the fetus is removed in pieces, not intact. … Removing the fetus in this manner does not violate the Act because the doctor will not have delivered the living fetus to one of the anatomical landmarks or committed an additional overt act that kills the fetus after partial delivery. …
D&E does not involve the delivery of a fetus because it requires the removal of fetal parts that are ripped from the fetus as they are pulled through the cervix.
[253] U.S. Code Title 7, Chapter 48, Section 1902: “Humane Methods of Livestock Slaughter.” Accessed September 9, 2023 at <www.law.cornell.edu>
No method of slaughtering or handling in connection with slaughtering shall be deemed to comply with the public policy of the United States unless it is humane. Either of the following two methods of slaughtering and handling are hereby found to be humane:
(a) in the case of cattle, calves, horses, mules, sheep, swine, and other livestock, all animals are rendered insensible to pain by a single blow or gunshot or an electrical, chemical or other means that is rapid and effective, before being shackled, hoisted, thrown, cast, or cut; or
(b) by slaughtering in accordance with the ritual requirements of the Jewish faith or any other religious faith that prescribes a method of slaughter whereby the animal suffers loss of consciousness by anemia of the brain caused by the simultaneous and instantaneous severance of the carotid arteries with a sharp instrument and handling in connection with such slaughtering.
[254] Code of Federal Regulations Title 9, Subchapter A, Part 313: “Humane Slaughter of Livestock.” Accessed September 9, 2023 at <www.law.cornell.edu>
§313.2 Handling of Livestock. …
(2) The dragging of disabled animals and other animals unable to move, while conscious, is prohibited.
§313.15 Mechanical; Captive Bolt. …
(a) Application of stunners, required effect; handling.
(1) The captive bolt stunners shall be applied to the livestock in accordance with this section so as to produce immediate unconsciousness in the animals before they are shackled, hoisted, thrown, cast, or cut. The animals shall be stunned in such a manner that they will be rendered unconscious with a minimum of excitement and discomfort. …
(3) Immediately after the stunning blow is delivered the animals shall be in a state of complete unconsciousness and remain in this condition throughout shackling, sticking and bleeding.
§313.16 Mechanical; Gunshot. …
(a) Utilization of firearms, required effect; handling.
(1) The firearms shall be employed in the delivery of a bullet or projectile into the animal in accordance with this section so as to produce immediate unconsciousness in the animal by a single shot before it is shackled, hoisted, thrown, cast, or cut. The animal shall be shot in such a manner that they will be rendered unconscious with a minimum of excitement and discomfort.
(3) Immediately after the firearm is discharged and the projectile is delivered, the animal shall be in a state of complete unconsciousness and remain in this condition throughout shackling, sticking and bleeding.
§313.30 Electrical; Stunning or Slaughtering with Electric Current. …
(3) Electric current. Each animal shall be given a sufficient application of electric current to ensure surgical anesthesia throughout the bleeding operation. Suitable timing, voltage and current control devices shall be used to ensure that each animal receives the necessary electrical charge to produce immediate unconsciousness. The current shall be applied so as to avoid the production of hemorrhages or other tissue changes which could interfere with inspection procedures.
[255] Public Law 116-72: “Preventing Animal Cruelty and Torture Act.” 116th U.S. Congress. Signed into law by Donald J. Trump on November 25, 2019. <www.congress.gov>
Sec. 2. Revision of Section 48.
(a) In General.—Section 48 of title 18, United States Code, is amended to read as follows:
Sec. 48. Animal crushing
(a) Offenses.—
1) Crushing.—It shall be unlawful for any person to purposely engage in animal crushing in or affecting interstate or foreign commerce or within the special maritime and territorial jurisdiction of the United States. …
f) Definitions.—In this section—
(1) the term “animal crushing” means actual conduct in which one or more living non-human mammals, birds, reptiles, or amphibians is purposely crushed, burned, drowned, suffocated, impaled, or otherwise subjected to serious bodily injury (as defined in section 1365 and including conduct that, if committed against a person and in the special maritime and territorial jurisdiction of the United States, would violate section 2241 or 2242);
[256] U.S. Code Title 18, Part I, Chapter 3, Section 48: “Animal Crushing.” Accessed September 9, 2023 at <www.law.cornell.edu>
(a) Offenses.—
(1) Crushing.—
It shall be unlawful for any person to purposely engage in animal crushing in or affecting interstate or foreign commerce or within the special maritime and territorial jurisdiction of the United States. …
(c) Penalties.—
Whoever violates this section shall be fined under this title, imprisoned for not more than 7 years, or both.
(d) Exceptions.—
(1) In general.—This section does not apply with regard to any conduct, or a visual depiction of that conduct, that is—
(A) a customary and normal veterinary, agricultural husbandry, or other animal management practice;
(B) the slaughter of animals for food;
(C) hunting, trapping, fishing, a sporting activity not otherwise prohibited by Federal law, predator control, or pest control;
(D) medical or scientific research;
(E) necessary to protect the life or property of a person; or
(F) performed as part of euthanizing an animal.
[257] U.S. Code Title 18, Part I, Chapter 65, Section 1365: “Tampering with Consumer Products.” Accessed September 9, 2023 at <www.law.cornell.edu>
(h) As used in this section …
(3) the term “serious bodily injury” means bodily injury which involves—
(A) a substantial risk of death;
(B) extreme physical pain;
(C) protracted and obvious disfigurement; or
(D) protracted loss or impairment of the function of a bodily member, organ, or mental faculty;
[258] Illinois Compiled Statues, Chapter 720, Title III, Section 12-20.5: “Dismembering A Human Body.” Accessed October 7, 2023 at <law.justia.com>
(a) A person commits dismembering a human body when he or she knowingly dismembers, severs, separates, dissects, or mutilates any body part of a deceased’s body.
(b) This Section does not apply to: …
(7) physicians licensed to practice medicine in all of its branches or holding a visiting professor, physician, or resident permit under the Medical Practice Act of 1987, performing acts in accordance with usual and customary standards of medical practice, or a currently enrolled student in an accredited medical school in furtherance of his or her education at the accredited medical school. …
(d) Sentence. Dismembering a human body is a Class X felony.
[259] Oregon Revised Statutes, Volume 04, Chapter 166, Section 166.087: “Abuse of Corpse in the First Degree.” Accessed October 7, 2023 at <law.justia.com>
(1) A person commits the crime of abuse of corpse in the first degree if the person: …
(b) Dismembers, mutilates, cuts or strikes a corpse.
(2) Abuse of corpse in the first degree is a Class B felony. [1993 c.294 §2]
Note: 166.087 was enacted into law by the Legislative Assembly but was not added to or made a part of ORS chapter 166 or any series therein by legislative action. See Preface to Oregon Revised Statutes for further explanation.
NOTE: See the next footnote, which documents that the note above doesn’t mean the statute “is any less the law.”
[260] “Preface to the Oregon Revised Statutes.” Oregon State Legislature, December 3, 2021. Modified 3/30/2022. <www.oregonlegislature.gov>
Page viii:
“Not added to and made a part of.” Notes may indicate that a particular ORS [Oregon Revised Statutes] section was not added to and made a part of the ORS chapter or series in which the section appears. These notes mean that the placement of the section was editorial and not by legislative action. Notes also are used when the series references are either too numerous or too complex to bear further adjustment. However, the note does not mean that the section not added to a series or a chapter is any less the law. The note is intended only to remind the user that definitions, penalties and other references to the series should be examined carefully to determine whether they apply to the noted section.
[261] Report: “The State of Abortion in the United States.” National Right to Life Committee, January 23, 2023. <www.nrlc.org>
Page 42:
During the 2015 state legislative session, Kansas* and Oklahoma* became the first two states to enact the Unborn Child Protection from Dismemberment Abortion Act. D&E dismemberment abortions of living unborn babies are as brutal as the partial-birth abortion method, which is now illegal in the United States. Eleven more states (Alabama*, Arkansas*, Indiana, Kentucky*, Louisiana*, Mississippi, Nebraska, North Dakota, Ohio, Texas, and West Virginia^) have enacted laws to protect unborn children from this brutal abortion procedure.
*not in effect pending litigation
^Law rendered ineffective with passage of the Unborn Child Protection Act W. Va. Code § 16-2R-1 et seq.
[262] Report: “The State of Abortion in the United States.” National Right to Life Committee, January 23, 2023. <www.nrlc.org>
Page 42:
During the 2015 state legislative session, Kansas* and Oklahoma* became the first two states to enact the Unborn Child Protection from Dismemberment Abortion Act. D&E dismemberment abortions of living unborn babies are as brutal as the partial-birth abortion method, which is now illegal in the United States. Eleven more states (Alabama*, Arkansas*, Indiana, Kentucky*, Louisiana*, Mississippi, Nebraska, North Dakota, Ohio, Texas, and West Virginia^) have enacted laws to protect unborn children from this brutal abortion procedure.
*not in effect pending litigation
^Law rendered ineffective with passage of the Unborn Child Protection Act W. Va. Code § 16-2R-1 et seq.
[263] Alabama Code Title 26, Chapter 23G, Section 3: “Dismemberment Abortion Prohibited Unless Necessary to Prevent Serious Health Risk to Mother of Unborn Child.” Accessed July 6, 2019 at <law.justia.com>
(a) Notwithstanding any other provision of law, it shall be unlawful for any individual to purposely perform or attempt to perform a dismemberment abortion and thereby kill an unborn child unless necessary to prevent serious health risk to the unborn child’s mother.
(b) An individual accused in any proceeding of unlawful conduct under subsection (a) may seek a hearing before the State Board of Medical Examiners on whether the dismemberment abortion was necessary to prevent serious health risk to the unborn child’s mother. The findings of the board are admissible on that issue at any trial in which such unlawful conduct is alleged. Upon a motion of the individual accused, the court shall delay the beginning of the trial for not more than 30 days to permit the hearing to take place.
(c) No woman upon whom an abortion is performed or attempted to be performed shall be thereby liable for performing or attempting to perform a dismemberment abortion. No nurse, technician, secretary, receptionist, or other employee or agent who is not a physician but who acts at the direction of a physician, and no pharmacist or other individual who is not a physician but who fills a prescription or provides instruments or materials used in an abortion at the direction of or to a physician, shall be thereby liable for performing or attempting to perform a dismemberment abortion.
(d) This chapter does not prevent abortion for any reason including rape and incest by any other method, unless otherwise prevented by law.
(Act 2016–397, §3.)
[264] Ruling: West Alabama Women’s Center v. Miller. U.S. Court of Appeals for the Eleventh Circuit. August 22, 2018. Decided 3–0. Majority: Carnes, Dubina. Concurring: Abrams. <media.ca11.uscourts.gov>
Ed Carnes, Chief Judge:
This case involves a method of abortion that is clinically referred to as Dilation and Evacuation (D & E). Or dismemberment abortion, as the State less clinically calls it. That name is more accurate because the method involves tearing apart and extracting piece-by-piece from the uterus what was until then a living unborn child. …
At that stage of pregnancy, it is settled under existing Supreme Court decisions that the State of Alabama cannot forbid this method of abortion entirely. … Recognizing that, the State has instead sought to make the procedure more humane by enacting the Alabama Unborn Child Protection from Dismemberment Abortion Act, which forbids dismembering a living unborn child.
Under the Act, the one performing the abortion is required to kill the unborn child before ripping apart its body during the extraction. See Id. Killing an unborn child and then dismembering it is permitted; killing an unborn child by dismembering it is not. …
The plaintiffs are the West Alabama Women’s Center, the Alabama Women’s Center, and the medical directors of both clinics.3 In 2016 the plaintiffs sued on behalf of themselves and their present and future patients, claiming that the Act was unconstitutional on its face.4
They then moved for a preliminary injunction barring enforcement of the Act. After holding an evidentiary hearing the district court entered an order preliminarily enjoining enforcement of the Act. In the course of doing so, the court issued an opinion with findings that there are no safe and effective ways for abortion practitioners to comply with the Act by killing the unborn child before dismembering it. …
The Supreme Court has interpreted the Fourteenth Amendment to bestow on women a fundamental constitutional right of access to abortions. See Roe v. Wade…. About twenty years after a majority of the Court had discovered that right lurking somewhere in the “penumbras of the Bill of Rights” as illuminated by the “concept of ordered liberty” … a majority of the Court devised an “undue burden” test to go with it, see Planned Parenthood of Se. Pa. v. Casey…. The Court’s most recent articulation of that test goes like this:
[T]here exists an undue burden on a woman’s right to decide to have an abortion, and consequently a provision of law is constitutionally invalid, if the purpose or effect of the provision is to place a substantial obstacle in the path of a woman seeking an abortion before the fetus attains viability. …
Over the past couple of decades the Supreme Court has issued several decisions drawing and redrawing the contours of the undue burden standard. Three of those decisions bear on the outcome of this case. …
Nearly 93% of abortions performed in Alabama occur before 15 weeks, at which time dismemberment abortion is unnecessary because the unborn child is small enough for practitioners to use other methods that the Act does not prohibit. For the 7% of abortions that occur after 15 weeks, 99% of them are by dismemberment. That’s because at that later stage of pregnancy dismemberment abortion is simpler and safer than other methods, with major complications arising less than 1% of the time. Of those post-15 week dismemberment abortions, one year hospitals performed 7 and clinics performed about 500. Those 500 dismemberment abortions occurred at only two clinics: the West Alabama Women’s Center and the Alabama Women’s Center. So the plaintiffs are the only clinics in Alabama that perform abortions at or after the 15-week mark.
With those background facts in mind, we turn to the State’s proposed fetal demise methods. The State contends that practitioners can cause fetal demise without much difficulty, so the Act does not effectively prohibit dismemberment abortions and thereby impose an undue burden on women seeking abortions. But the State conceded at oral argument: “[I]f there [is] no safe and effective way to cause fetal demise before [dismemberment,] … this law would be unconstitutional.” … As a result, this case turns on whether the fetal demise methods are feasible, which in this context means safe, effective, and available. The State proposes three methods: (1) injecting potassium chloride into the unborn child’s heart; (2) cutting the umbilical cord in utero; and (3) injecting digoxin into the amniotic fluid. The district court found each to be infeasible. …
All of those findings about the fetal demise methods––their attendant risks; their technical difficulty; their untested nature; the time and cost associated with performing them; the lack of training opportunities; and the inability to recruit experienced practitioners to perform them—support the conclusion that the Act would “place a substantial obstacle in the path of a woman seeking an abortion before the fetus attains viability.” Id. (emphasis and quotation marks omitted). So does the fact that every court to consider the issue has ruled that laws banning dismemberment abortions are invalid and that fetal demise methods are not a suitable workaround. …
In our judicial system, there is only one Supreme Court, and we are not it. As one of the “inferior Courts,” we follow its decisions. U.S. Const. art. III, § 1 (“The judicial Power of the United States, shall be vested in one supreme Court, and in such inferior Courts as the Congress may from time to time ordain and establish.”). The primary factfinder is the district court, and we are not it. Our role is to apply the law the Supreme Court has laid down to the facts the district court found. The result is that we affirm the judgment of the district court.
Joel F. Dubina, Circuit Judge, concurring specially:
I concur fully in Chief Judge Carnes’s opinion because it correctly characterizes the record in this case, and it correctly analyzes the law. I write separately to agree on record with Justice Thomas’s concurring opinion in Gonzales v. Carhart … with whom then Justice Scalia also joined. Specifically, Justice Thomas wrote, “I write separately to reiterate my view that the Court’s abortion jurisprudence, including Casey … and Roe v. Wade … has no basis in the Constitution…. The problem I have, as noted in the Chief Judge’s opinion, is that I am not on the Supreme Court, and as a federal appellate judge, I am bound by my oath to follow all of the Supreme Court’s precedents, whether I agree with them or not.
[265] 2019 Indiana Code, Title 16, Article 18, Chapter 2: “Definitions: Dismemberment Abortion.” Accessed October 21, 2023 at <law.justia.com>
Sec. 96.4. (a) “Dismemberment abortion” means an abortion with the purpose of killing a living fetus in which the living fetus is extracted one (1) piece at a time from the uterus through clamps, grasping forceps, tongs, scissors, or another similar instrument that, through the convergence of two (2) rigid levers, slices, crushes, or grasps a portion of the fetus’s body to cut or rip it off.
(b) “Dismemberment abortion” does not include an abortion that uses suction to dismember a fetus by sucking fetal parts into a collection container.
[266] Order: Bernard v. Individual Members of Indiana Medical Licensing Board. U.S. District Court, Southern District of Indiana. June 28, 2019. <caselaw.findlaw.com>
Conclusion and Order
HEA [House Enrolled Act] 1211 prohibits physicians from utilizing the most common, safest, often most cost effective, and best understood method of second trimester abortion, requiring instead resort to alternatives that are medically riskier, more costly, less reliable, and in some instances simply unavailable, while accomplishing little more than expressing hostility towards the constitutionally fundamental right of women to control their own reproductive lives as established in Roe.
For this reason and the others given above:
Plaintiff’s motion for a preliminary injunction is GRANTED.
Defendants are PRELIMINARILY ENJOINED from enforcing HEA 1211, Act of April 24, 2019 … prohibiting the knowing or intentional performance of a “dismemberment abortion” as defined therein. NO BOND is required of Plaintiff.
IT IS SO ORDERED. …
Sarah Evans Barker, Judge
[267] Webpage: “American Medical News.” American Medical Association. Accessed September 6, 2008 at <bit.ly>
American Medical News is the newspaper for America’s physicians. Published since 1958, it is one of the most widely read publications in the United States on news affecting the medical profession. From Medicare and managed care to public health and practice management, no other source covers the same range of current events affecting medical practice.
American Medical News is published by the American Medical Association and is intended to serve as a credible forum for information affecting physicians and their practices. The content of articles and the opinions expressed in AMNews are not necessarily endorsed by the AMA [American Medical Association].
[268] Article: “Veto-Proof Majority in House Votes to Prohibit Late-Term Procedure.” By Diane M. Gianelli. American Medical News, November 20, 1995. <www.nrlc.org>
“Partial birth” abortions, also called “intact D&E” (for dilation and evacuation), or “D&X” (dilation and extraction) are done by only a handful of U.S. physicians, including Martin Haskell, MD, of Dayton, Ohio, and, until his recent death, James T. McMahon, MD, of the Los Angeles area. Dr. McMahon said in a 1993 AMNews interview that he had trained about a half-dozen physicians to do the procedure.
The procedure usually involves the extraction of an intact fetus, feet first, through the birth canal, with all but the head delivered. The surgeon forces scissors into the base of the skull, spreads them to enlarge the opening, and uses suction to remove the brain.
[269] Entry: “abortion, partial-birth.” Melloni’s Illustrated Medical Dictionary (4th edition). Parthenon Publishing Group, 2002.
Page 2: “Common term for termination of a late pregnancy with a breech presentation. Labor is induced by conventional methods; the cervix is widely dilated and delivery is expedited by evacuation the cranial contents with a suction catheter, then compressing the cranium.”
[270] Article: “2nd Trimester Abortion: An Interview with W. Martin Haskell, MD.” Cincinnati Medicine, Fall 1993. Pages 18–19. <www.nrlc.org>
Page 19:
The D & X Procedure—Dilation and Extraction (D & X), a method for second trimester abortion up to 26 weeks, was developed in 1992 by Cincinnati physician W. Martin Haskell, MD. It is a modification of Dismemberment and Extraction (D & E) which has been used in the US since the 1970s. Haskell has performed more than 700 D & X procedures in his office.
Step One—The patient’s cervix is dilated to 9–11 mm over a period of two days using Dilapan hydroscopic dilators. The patient remains at home during the dilation period.
Step Two—In the operating room, patients are given Valium, the Dilapan are removed and the cervix is scrubbed. anesthetized and grasped with a tenaculum. Membranes are ruptured.
Step Three—The surgical assistant scans the fetus with ultrasound, locating the lower extremities.
Step Four—Using a large forcep, the surgeon opens and closes its jaws to firmly grasp a lower extremity. The surgeon turns the fetus if necessary and pulls the extremity into the vagina.
Step Five—The surgeon uses his fingers to deliver the opposite lower extremity, then the torso, shoulders, and upper extremities.
Step Six—The skull lodges at the internal cervical os [hole at the center of the cervix]. Usually there is not enough dilation for it to pass through. The fetus is spine up.
Step Seven—A right-handed surgeon slides the fingers of his left hand along the back of the fetus and hooks the shoulders of the fetus with the index and ring fingers (palm down). He slides the tip of his middle finger along the spine towards the skull while applying traction to the shoulder and lower extremities. The middle finger lifts and pushes the anterior cervical lip out of the way.
Step Eight—While maintaining this tension, the surgeon takes a pair of blunt curved scissors in the right hand. He advances the tip, curved down, along the spine and under his middle finger until he feels it contact the base of the skull under the tip of his middle finger. The surgeon forces the scissors into the base of the skull and spreads the scissors to enlarge the opening.
Step Nine—The surgeon removes the scissors and introduces a suction catheter into this hole and evacuates the skull contents.
Step Ten—With the catheter still in place, he applies traction to the fetus, removing it completely from the patient, then removes the placenta.
[271] Presentation: “Dilation and Extraction for Late Second Trimester Abortion.” By Martin Haskell. National Abortion Federation, September 13, 1992. <operationrescue.org>
Page 1:
The surgical method described in this paper [partial-birth abortion] differs from classic D&E [dilation and evacuation] in that it does not rely upon dismemberment to remove the fetus. Nor are inductions or infusions used to expel the intact fetus.
Rather, the surgeon grasps and removes a nearly intact fetus through an adequately dilated cervix. The author has coined the term Dilation and Extraction or D&X to distinguish it from dismemberment-type D&E’s.
This procedure can be performed in a properly equipped physician’s office under local anesthesia. It can be used successfully in patients 20–26 weeks in pregnancy.
The author has performed over 700 of these procedures with a low rate of complications.
NOTE: Pages 2–5 describe the procedure in greater detail.
[272] Webpage: “Summary of House Resolution 1833: Partial-Birth Abortion Ban Act of 1995.” U.S. House of Representatives, 104th Congress (1995–1996). Accessed April 15, 2017 at <www.congress.gov>
Sponsor: Canady, Charles T. [R-FL] (Introduced 06/14/1995) …
Subjects any physician who knowingly performs a partial-birth abortion in or affecting interstate or foreign commerce to a fine or imprisonment for not more than two years or both, except where such an abortion is necessary to save the life of a mother endangered by a physical disorder, illness, or injury, provided that no other medical procedure would suffice.
Defines: (1) “partial-birth abortion” as an abortion in which the person performing the abortion partially vaginally delivers a living fetus before killing the fetus and completing the delivery; and (2) “physician” as a doctor of medicine or osteopathy legally authorized to practice medicine and surgery by the State in which the doctor performs such activity, or any other individual legally authorized by the State to perform abortions.
Permits the father (if married to the mother at the time she receives a partial-birth abortion procedure) and (if the mother has not attained the age of 18 at the time of the abortion) the maternal grandparents to obtain, through a civil action, relief which would include money damages for all psychological and physical injuries and statutory damages equal to three times the cost of the partial-birth abortion, unless the pregnancy resulted from the plaintiff’s criminal conduct or the plaintiff consented to the abortion.
[273] Webpage: “Cosponsors of House Resolution 1833: Partial-Birth Abortion Ban Act of 1995.” U.S. House of Representatives, 104th Congress (1995–1996). Accessed April 21, 2017 at <www.congress.gov>
“Sponsor: Canady, Charles T. [R-FL] … Cosponsor statistics: 115 current [96 Republicans, 19 Democrats]”
[274] Calculated with data from:
a) Vote 94: “Partial-Birth Abortion Ban Act of 1995.” U.S. House of Representatives, March 27, 1996. <clerk.house.gov>
b) Vote 596: “Partial-Birth Abortion Ban Act of 1995.” U.S. Senate, December 7, 1995. <www.senate.gov>
Combined vote totals from both Houses of Congress:
|
Party |
Voted “Yes” |
Voted “No” |
Voted “Present” or Did Not Vote† |
|||
|
Number |
Portion |
Number |
Portion |
Number |
Portion |
|
|
Republican |
259 |
90% |
23 |
8% |
6 |
2% |
|
Democrat |
81 |
34% |
149 |
62% |
11 |
5% |
|
Independent |
0 |
0% |
1 |
100% |
0 |
0% |
|
NOTE: †Voting “Present” is effectively the same as not voting. |
||||||
[275] Webpage: “Actions on House Resolution 1833: Partial-Birth Abortion Ban Act of 1995.” U.S. House of Representatives, 104th Congress (1995–1996). Accessed April 21, 2017 at <www.congress.gov>
|
Date |
Action |
|
6/14/1995 |
Introduced in House |
|
11/1/1995 |
Passed/agreed to in House: On passage Passed by the Yeas and Nays: 288–139, 1 Present (Roll no. 756). |
|
12/7/1995 |
Passed Senate with amendments by Yea-Nay Vote. 54–44. |
|
3/27/1996 |
On motion that the House agree to the Senate amendments Agreed to by the Yeas and Nays: 286–129, 1 Present (Roll no. 94). |
|
4/10/1996 |
Vetoed by President. |
|
9/19/1996 |
Passed House over veto: Two-thirds of the Members present having voted in the affirmative the bill is passed, the objections of the President to the contrary notwithstanding. Passed by the Yeas and Nays (2/3 required): 285–137 (Roll No. 422). |
|
9/26/1996 |
Failed of passage in Senate over veto: Failed of passage in Senate over veto by Yea–Nay Vote. 58–40. Record Vote No: 301. |
[276] Calculated with data from the footnote above and the report: “Veto Override Procedure in the House and Senate.” By Elizabeth Rybicki. Congressional Research Service, March 2019. <crsreports.congress.gov>
According to Article 1, Section 7, of the Constitution, when the President chooses not to sign a bill1 and instead returns it to the chamber that originated it, the chamber shall enter the message of the President detailing the reasons for the veto in its Journal and then “proceed to reconsider” the bill.2 A vetoed bill can become law if two-thirds of the Members voting in each chamber agree, by recorded vote, a quorum being present, to repass the bill and thereby override the veto of the President.
CALCULATION: 98 Voting Members × 2/3 = 65.3
[277] Webpage: “Summary of House Resolution 1122: Partial-Birth Abortion Ban Act of 1997.” U.S. House of Representatives, 105th Congress (1997–1998). Accessed April 21, 2017. <www.congress.gov>
Sponsor: Solomon, Gerald B. H. [R-NY] (Introduced 03/19/1997) …
Amends the Federal criminal code to prohibit any physician from knowingly performing a partial-birth abortion in or affecting interstate or foreign commerce, unless it is necessary to save the life of the mother. Prescribes penalties.
Defines a “partial birth abortion” as an abortion in which a person, deliberately and intentionally, partially vaginally delivers a living fetus before killing the fetus and completing the delivery.
Authorizes the father, if married to the mother at the time of the abortion, and the maternal grandparents of the fetus, if the mother is under 18 years of age, to obtain specified relief in a civil action, unless the pregnancy resulted from the plaintiff’s criminal conduct or the plaintiff consented to the abortion.
Authorizes a defendant accused of an offense under this Act to seek a hearing before the State Medical Board on whether the physician’s conduct was necessary to save the life of the mother.
Prohibits the prosecution of a woman upon whom a partial-birth abortion is performed for conspiracy to violate this Act or under provisions regarding punishment as a principal or an accessory or for concealment of a felony.
[278] Calculated with data from:
a) Vote 500: “Partial-Birth Abortion Ban Act of 1997.” U.S. House of Representatives, October 8, 1997. <clerk.house.gov>
b) Vote 71: “Partial-Birth Abortion Ban Act of 1997.” U.S. Senate, May 20, 1997. <www.senate.gov>
Combined vote totals from both Houses of Congress:
|
Party |
Voted “Yes” |
Voted “No” |
Voted “Present” or Did Not Vote† |
|||
|
Number |
Portion |
Number |
Portion |
Number |
Portion |
|
|
Republican |
268 |
95% |
12 |
4% |
2 |
1% |
|
Democrat |
92 |
37% |
155 |
62% |
4 |
2% |
|
Independent |
0 |
0% |
1 |
100% |
0 |
0% |
|
NOTE: †Voting “Present” is effectively the same as not voting. |
||||||
[279] Webpage: “Actions on House Resolution 1122: Partial-Birth Abortion Ban Act of 1997.” U.S. House of Representatives, 105th Congress (1997–1998). Accessed April 21, 2017 at <www.congress.gov>
|
Date |
Action |
|
3/19/1997 |
Introduced in House |
|
3/20/1997 |
Passed/agreed to in House: On passage Passed by recorded vote: 295–136 (Roll no. 65). |
|
5/20/1997 |
Passed/agreed to in Senate: Passed Senate with amendments by Yea–Nay Vote. 64–36. Record Vote No: 71. |
|
10/8/1997 |
Resolving differences—House actions: On motion that the House agree to the Senate amendments Agreed to by the Yeas and Nays: 296–132 (Roll no. 500). |
|
10/10/1997 |
Vetoed by President. |
|
7/23/1998 |
Passed House over veto: Two-thirds of the Members present having voted in the affirmative the bill is passed, the objections of the President to the contrary notwithstanding. Passed by the Yeas and Nays (2/3 required): 296–132 (Roll No. 325). |
|
9/18/1998 |
Failed of passage in Senate over veto: Failed of passage in Senate over veto by Yea–Nay Vote. 64–36. Record Vote No: 277. |
[280] Calculated with data from the footnote above and the report: “Veto Override Procedure in the House and Senate.” By Elizabeth Rybicki. Congressional Research Service, March 2019. <crsreports.congress.gov>
According to Article 1, Section 7, of the Constitution, when the President chooses not to sign a bill1 and instead returns it to the chamber that originated it, the chamber shall enter the message of the President detailing the reasons for the veto in its Journal and then “proceed to reconsider” the bill.2 A vetoed bill can become law if two-thirds of the Members voting in each chamber agree, by recorded vote, a quorum being present, to repass the bill and thereby override the veto of the President.
CALCULATION: 100 Voting Members × 2/3 = 66.7
[281] Webpage: Summary of Senate Bill S.3: Partial-Birth Abortion Ban Act of 2003.” U.S. Senate, 108th Congress (2003–2004). Accessed April 21, 2017 at <www.congress.gov>
Sponsor: Santorum, Rick [R-PA] (Introduced 02/14/2003) …
Amends the Federal criminal code to prohibit any physician or other individual from knowingly performing a partial-birth abortion, except when necessary to save the life of a mother whose life is endangered by a physical disorder, illness, or injury.
Defines a “partial-birth abortion” as an abortion in which the person performing the abortion: (1) deliberately and intentionally vaginally delivers a living fetus until, in the case of a head-first presentation, the entire fetal head is outside the mother’s body, or, in the case of a breech presentation, any part of the fetal trunk past the navel is outside the mother’s body; and (2) performs the overt act, other than completion of delivery, that kills the partially delivered living fetus.
Authorizes the father, if married to the mother at the time of the abortion, and the maternal grandparents of the fetus, if the mother is under 18 years of age, to obtain specified relief in a civil action, unless the pregnancy resulted from the plaintiff’s criminal conduct or the plaintiff consented to the abortion.
Authorizes a defendant accused of an offense under this Act to seek a hearing before the State Medical Board on whether the physician’s conduct was necessary to save the life of the mother.
Prohibits the prosecution of a woman upon whom a partial-birth abortion is performed for conspiracy to violate this Act or under provisions regarding punishment as a principal or an accessory or for concealment of a felony.
[282] Webpage: “Cosponsors of Senate Bill S.3: Partial-Birth Abortion Ban Act of 2003.” U.S. Senate, 108th Congress (2003–2004). Accessed April 21, 2017 at <www.congress.gov>
“Cosponsor statistics: 45 current [2 Democrats, 43 Republicans]”
[283] Calculated with data from:
a) Vote 530: “Partial-Birth Abortion Ban Act of 2003.” U.S. House of Representatives, October 2, 2003. <clerk.house.gov>
b) Vote 402: “Partial-Birth Abortion Ban Act of 2003.” U.S. Senate, October 21, 2003. <www.senate.gov>
Combined vote totals from both Houses of Congress:
|
Party |
Voted “Yes” |
Voted “No” |
Voted “Present” or Did Not Vote† |
|||
|
Number |
Portion |
Number |
Portion |
Number |
Portion |
|
|
Republican |
265 |
95% |
7 |
3% |
8 |
3% |
|
Democrat |
80 |
32% |
167 |
66% |
6 |
2% |
|
Independent |
0 |
0% |
2 |
100% |
0 |
0% |
|
NOTE: †Voting “Present” is effectively the same as not voting. |
||||||
[284] Webpage: “Actions on Senate Bill 3: Partial-Birth Abortion Ban Act of 2003.” U.S. Senate, 108th Congress (2003–2004). Accessed April 21, 2017 at <www.congress.gov>
|
Date |
Action |
|
2/14/2003 |
Introduced in Senate |
|
3/13/2003 |
Passed Senate with an amendment by Yea–Nay Vote. 64–33. Record Vote Number: 51 |
|
10/2/2003 |
Conference report agreed to in House: On agreeing to the conference report Agreed to by the Yeas and Nays: 281–142 (Roll no. 530). |
|
10/21/2003 |
Conference report agreed to in Senate: Senate agreed to conference report by Yea–Nay Vote. 64–34. Record Vote Number: 402. |
|
11/5/2003 |
Signed by President. Became Public Law No: 108-105. |
[285] Senate Bill 3: “Partial-Birth Abortion Ban Act of 2003.” U.S. Senate, 108th Congress (2003–2004). Accessed April 21, 2017 at <www.congress.gov>
Sec. 1531. Partial-birth abortions prohibited
(a) Any physician who, in or affecting interstate or foreign commerce, knowingly performs a partial-birth abortion and thereby kills a human fetus shall be fined under this title or imprisoned not more than 2 years, or both.
[286] Ruling: Gonzales v. Carhart. United States Supreme Court, April 18, 2007. Decided 5–4. Majority: Kennedy, Roberts, Scalia, Thomas, Alito. Concurring: Thomas, Scalia. Dissenting: Ginsburg, Stevens, Souter, Breyer. <caselaw.findlaw.com>
Majority:
[Section] IV (B): “In addition the Act’s prohibition only applies to the delivery of ‘a living fetus.’ … If the [partial-birth abortion] procedure is truly necessary in some circumstances, it appears likely an injection that kills the fetus is an alternative under the Act that allows the doctor to perform the procedure.”
[287] Ruling: Gonzales v. Carhart. United States Supreme Court, April 18, 2007. Decided 5–4. Majority: Kennedy, Roberts, Scalia, Thomas, Alito. Concurring: Thomas, Scalia. Dissenting: Ginsburg, Stevens, Souter, Breyer. <caselaw.findlaw.com>
Majority:
In No. 05-380 (Carhart) respondents are LeRoy Carhart, William G. Fitzhugh, William H. Knorr, and Jill L. Vibhakar, doctors who perform second-trimester abortions. These doctors filed their complaint against the Attorney General of the United States in the United States District Court for the District of Nebraska. They challenged the constitutionality of the Act and sought a permanent injunction against its enforcement.
[288] Ruling: Gonzales v. Carhart. United States Supreme Court, April 18, 2007. Decided 5–4. Majority: Kennedy, Roberts, Scalia, Thomas, Alito. Concurring: Thomas, Scalia. Dissenting: Ginsburg, Stevens, Souter, Breyer. <caselaw.findlaw.com>
Majority:
In No. 05-380 (Carhart) respondents are LeRoy Carhart, William G. Fitzhugh, William H. Knorr, and Jill L. Vibhakar, doctors who perform second-trimester abortions. These doctors filed their complaint against the Attorney General of the United States in the United States District Court for the District of Nebraska. They challenged the constitutionality of the Act and sought a permanent injunction against its enforcement. …
Respondents have not demonstrated that the Act, as a facial matter, is void for vagueness, or that it imposes an undue burden on a woman’s right to abortion based on its overbreadth or lack of a health exception. For these reasons the judgments of the Courts of Appeals for the Eighth and Ninth Circuits are reversed.
[289] Article: “McCain Promises Judges Like Roberts, Alito.” Associated Press, May 6, 2008. <www.cbsnews.com>
“Obama, on the other hand, voted against Roberts and Alito.”
[290] Article: “Obama, McCain Talk Issues at Pastor’s Forum.” By Ed Hornick. CNN, August 17, 2008. <www.cnn.com>
“Neither candidate shied away from a question about which current Supreme Court justice they would not have nominated. Obama’s reply: Clarence Thomas.”
[291] Article: “Obama: I Would Not Have Nominated Clarence Thomas.” By Sam Stein. Huffington Post, August 16, 2008. <www.huffingtonpost.com>
[Quoting Obama:] “I would not have nominated Justice Scalia….”
[292] Senate Bill 1173: “Freedom of Choice Act.” U.S. Senate, 110th Congress (2007–2008). Accessed April 22, 2017 at <www.congress.gov>
In the Senate of the United States
April 19, 2007
Mrs. Boxer (for herself, Mrs. Murray, Ms. Stabenow, Mr. Bingaman, Mr. Menendez, Mr. Lautenberg, Mr. Cardin, Mr. Schumer, Mrs. Clinton, Mrs. Feinstein, Ms. Mikulski, Mr. Baucus, and Ms. Cantwell) introduced the following bill; which was read twice and referred to the Committee on the Judiciary …
To protect, consistent with Roe v. Wade, a woman’s freedom to choose to bear a child or terminate a pregnancy, and for other purposes. …
Sec. 4. Interference with Reproductive Health Prohibited. …
(b) Prohibition of Interference—A government may not—
(1) deny or interfere with a woman’s right to choose—
(A) to bear a child;
(B) to terminate a pregnancy prior to viability; or
(C) to terminate a pregnancy after viability where termination is necessary to protect the life or health of the woman; or
(2) discriminate against the exercise of the rights set forth in paragraph (1) in the regulation or provision of benefits, facilities, services, or information. …
Sec. 6. Retroactive Effect.
This Act applies to every Federal, State, and local statute, ordinance, regulation, administrative order, decision, policy, practice, or other action enacted, adopted, or implemented before, on, or after the date of enactment of this Act.
[293] House Resolution 1964 IH: Freedom of Choice Act.” U.S. House of Representatives, 110th Congress (2007–2008). Accessed April 22, 2017 at <www.congress.gov>
In the House of Representatives
April 19, 2007
Mr. Nadler (for himself, Mr. Abercrombie, Mr. Ackerman, Mr. Allen, Mr. Arcuri, Ms. Baldwin, Ms. Berkley, Mr. Berman, Mr. Blumenauer, Mr. Boucher, Mrs. Capps, Mr. Cohen, Mr. Conyers, Mr. Davis of Illinois, Mrs. Davis of California, Mr. DeFazio, Mr. Ellison, Mr. Emanuel, Mr. Farr, Mr. Fattah, Mr. Filner, Mr. Frank of Massachusetts, Mr. Grijalva, Ms. Harman, Ms. Hirono, Mr. Holt, Mr. Honda, Mr. Inslee, Ms. Jackson-Lee of Texas, Mr. Jackson of Illinois, Mr. Kucinich, Mr. Lantos, Mr. Larsen of Washington, Ms. Lee, Mr. Loebsack, Mrs. Lowey, Ms. Matsui, Ms. McCollum of Minnesota, Mr. McDermott, Mrs. Maloney of New York, Mr. Miller of North Carolina, Mr. Moran of Virginia, Mr. Olver, Mr. Porter, Ms. Linda T. Sánchez of California, Ms. Schakowsky, Mr. Shays, Ms. Slaughter, Ms. Solis, Mr. Stark, Ms. Sutton, Mr. Thompson of California, Mr. Towns, Ms. Watson, Mr. Waxman, Mr. Weiner, Mr. Wexler, and Ms. Woolsey) introduced the following bill; which was referred to the Committee on the Judiciary …
To protect, consistent with Roe v. Wade, a woman’s freedom to choose to bear a child or terminate a pregnancy, and for other purposes. …
Sec. 2. Findings. …
(9) Further threatening Roe, the Supreme Court recently upheld the first-ever Federal ban on abortion, which has no exception to protect a woman’s health. The majority decision in Gonzales v. Carhart and Gonzales v. Planned Parenthood Federation of America permits the government to interfere with a woman’s right to choose to terminate a pregnancy and effectively overturns a core tenet of Roe v. Wade by abandoning more than 30 years of protection for women’s health. …
Sec. 4. Interference with Reproductive Health Prohibited.
(a) Statement of Policy—It is the policy of the United States that every woman has the fundamental right to choose to bear a child, to terminate a pregnancy prior to fetal viability, or to terminate a pregnancy after fetal viability when necessary to protect the life or health of the woman.
(b) Prohibition of Interference—A government may not—
(1) deny or interfere with a woman’s right to choose—
(A) to bear a child;
(B) to terminate a pregnancy prior to viability; or
(C) to terminate a pregnancy after viability where termination is necessary to protect the life or health of the woman; or
(2) discriminate against the exercise of the rights set forth in paragraph (1) in the regulation or provision of benefits, facilities, services, or information. …
Sec. 6. Retroactive Effect.
This Act applies to every Federal, State, and local statute, ordinance, regulation, administrative order, decision, policy, practice, or other action enacted, adopted, or implemented before, on, or after the date of enactment of this Act.
[294] Open letter from Kim Gandy (President, National Organization for Women). April 20, 2007. <www.now.org>
Yesterday [April 19, 2007] I was pleased to stand with Senator Barbara Boxer, Representative Jerrold Nadler and many members of Congress as they announced the reintroduction of this important act, which would legislatively reverse the Court’s damaging decision [in Gonzalez v. Carhart] and will enshrine in federal law our right to safe, legal abortion.
[295] Introduction of Bills and Joint Resolutions: S.1173. Congressional Record, May 11, 2007. Page S6017. <www.govinfo.gov>
Page S6017: “At the request of Mrs. BOXER, the name of the Senator from Illinois (Mr. OBAMA) was added as a cosponsor of S. 1173, a bill to protect, consistent with Roe v. Wade, a woman’s freedom to choose to bear a child or terminate a pregnancy, and for other purposes.”
[296] Speech: “Barack Obama before Planned Parenthood Action Fund.” July 17, 2007. Transcribed by Laura Echevarria. <bit.ly>
“Well, the first thing I’d do as President is, is sign the Freedom of Choice Act. … That’s the first thing that I’d do.”
[297] Transcript: “The President’s News Conference.” Administration of Barack H. Obama, April 29, 2009. <www.govinfo.gov>
[President Obama:] …
Now, the freedom of choice act is not my highest legislative priority. I believe that women should have the right to choose, but I think that the most important thing we can do to tamp down some of the anger surrounding this issue is to focus on those areas that we can agree on. And that’s where I’m going to focus.”
[298] Article: “2nd Trimester Abortion: An Interview with W. Martin Haskell, MD.” Cincinnati Medicine, Fall 1993. <www.nrlc.org>
Page 19:
The D & X Procedure—Dilation and Extraction (D & X), a method for second trimester abortion up to 26 weeks, was developed in 1992 by Cincinnati physician W. Martin Haskell, MD. It is a modification of Dismemberment and Extraction (D & E) which has been used in the US since the 1970s. Haskell has performed more than 700 D & X procedures in his office.
Step One—The patient’s cervix is dilated to 9–11 mm over a period of two days using Dilapan hydroscopic dilators. The patient remains at home during the dilation period.
Step Two—In the operating room, patients are given Valium, the Dilapan are removed and the cervix is scrubbed. anesthetized and grasped with a tenaculum. Membranes are ruptured.
Step Three—The surgical assistant scans the fetus with ultrasound, locating the lower extremities.
Step Four—Using a large forcep, the surgeon opens and closes its jaws to firmly grasp a lower extremity. The surgeon turns the fetus if necessary and pulls the extremity into the vagina.
Step Five—The surgeon uses his fingers to deliver the opposite lower extremity, then the torso, shoulders, and upper extremities.
Step Six—The skull lodges at the internal cervical os [hole at the center of the cervix]. Usually there is not enough dilation for it to pass through. The fetus is spine up.
Step Seven—A right-handed surgeon slides the fingers of his left hand along the back of the fetus and hooks the shoulders of the fetus with the index and ring fingers (palm down). He slides the tip of his middle finger along the spine towards the skull while applying traction to the shoulder and lower extremities. The middle finger lifts and pushes the anterior cervical lip out of the way.
Step Eight—While maintaining this tension, the surgeon takes a pair of blunt curved scissors in the right hand. He advances the tip, curved down, along the spine and under his middle finger until he feels it contact the base of the skull under the tip of his middle finger. The surgeon forces the scissors into the base of the skull and spreads the scissors to enlarge the opening.
Step Nine—The surgeon removes the scissors and introduces a suction catheter into this hole and evacuates the skull contents.
Step Ten—With the catheter still in place, he applies traction to the fetus, removing it completely from the patient, then removes the placenta.
[299] Letter: “Barbara Bolsen (Editor, American Medical News) to Charles T. Canady (Chairmen, Subcommittee on the Constitution, Judiciary Committee, U.S. House of Representatives).” July 11, 1995. <www.congress.gov>
Page H1063:
We have full documentation of these interviews, including tape recordings and transcripts. …
Haskell: And I’ll be quite frank: most of my abortions are elective in that 20–24 week range … In my particular case, probably 20% are for genetic reasons. And the other 80% are purely elective….
NOTE: This statement was made in an interview conducted for an article published on July 5, 1993. That Haskell was referring to partial-birth abortion is demonstrated in the next two footnotes.
[300] Presentation: “Dilation and Extraction for Late Second Trimester Abortion.” By Martin Haskell. National Abortion Federation, September 13, 1992. <operationrescue.org>
Page 1:
The surgical method described in this paper differs from classic D&E [dilation and evacuation] in that it does not rely upon dismemberment to remove the fetus. Nor are inductions or infusions used to expel the intact fetus.
Rather, the surgeon grasps and removes a nearly intact fetus through an adequately dilated cervix. The author has coined the term Dilation and Extraction or D&X to distinguish it from dismemberment-type D&E’s. …
Page 2: “The author routinely performs this procedure on all patients 20 through 24 weeks LMP [last menstrual period] with certain exceptions.”
[301] Article: “Shock-Tactic Ads Target Late-Term Abortion Procedure: Foes Hope Campaign Will Sink Federal Abortion Rights Legislation.” By Diane M. Gianelli. American Medical News, July 5, 1993. <www.congress.gov>
Pages S16794–S16795:
But Dr. Haskell and another doctor who routinely use the [partial-birth] procedure for late term abortions told AMNews that the majority of fetuses aborted this way are alive until the end of the procedure. …
Dr. Haskell said he performs abortions “up until about 25 weeks’ ” gestation, most of them elective.
[302] House report 104-267: “Partial-Birth Abortion Ban Act of 1995.” Judiciary Committee, U.S. House of Representatives, September 27, 1995. <www.govinfo.gov>
Page 8:
The writings of both Dr. Haskell and Dr. McMahon advocate partial-birth abortion as the method they prefer for all late-term abortions.22 Dr. Haskell told the AMNews that the vast majority of the partial-birth abortions he performs are elective. He stated, “And I’ll be quite frank: most of my abortions are elective in that 20–24 week range. … In my particular case, probably 20% are for genetic reasons. And the other 80% are purely elective. …”23
Dr. McMahon uses the partial-birth abortion method through the entire 40 weeks of pregnancy. He claims that most of the abortions he performs are “non-elective,” but his definition of “non-elective” is extremely broad. Dr. McMahon sent a letter to the Constitution Subcommittee in which he described abortions performed because of the mother’s youth or depression as “non-elective.”24
22 Haskell, supra note 4 at 27; Letter from James T. McMahon, M.D., to the Subcomm. on the Constitution of the House Comm. on the Judiciary (June 6, 1995) (on file with the Subcomm. on the Constitution of the House Comm. on the Judiciary).
23 Letter from Barbara Bolsen, supra note 17.
24 Letter from James T. McMahon, M.D., supra note 20.
[303] Letter from 53 Organizations to U.S. Congressman Christopher Smith, October 2, 1995.
October 2, 1995
The Honorable Christopher H. Smith
U.S. House of Representatives
2370 Rayburn House Office Building
Washington, DC 20515
Dear Representative Smith:
As organizations which support full access to safe, legal abortion services, we urge you to oppose H.R. 1833, legislation that would ban a particular type of abortion procedure, known to abortion providers as intact D&E [dilation and evacuation] or D&X [dilation and extraction]. The technique has been sensationalized by anti-abortion advocates, who inaccurately refer to the surgery as a “partial birth” abortion—a term unknown in the medical community, and invented solely for this legislation. …
This surgical procedure is used only in rare cases, fewer than 500 per year. It is most often performed in the case of wanted pregnancies gone tragically wrong, when a family learns late in pregnancy of severe fetal anomalies or a medical condition that threatens the pregnant woman’s life or health. …
Sincerely,
Advocates for Youth
The Alan Guttmacher Institute
American Association of University Women
American Civil Liberties Union
American Humanist Association
American Jewish Committee
American Jewish Congress
Americans for Democratic Action
Americans for Religious Liberty
Association of Reproductive Health Professionals
The Center for Reproductive Law and Policy
Center for Women’s Policy Studies
Clara Bell Duvall Education Fund
Coalition of Labor Union Women
Disciples for Choice
The Feminist Majority
Hollywood Women’s Political Committee
Human Rights Campaign Fund
Institute for Research on Women’s Health
International Projects Assistance Service
Medical Students for Choice
Michigan Welfare Rights League
National Abortion Federation
National Abortion and Reproductive Rights Action League
National Asian Women’s Health Network
National Association of Nurse Practitioners
National Black Women’s Health Project
National Center for the ProChoice Majority
National Council of Jewish Women
National Family Planning and Reproductive Health Association
National Latina Institute for Reproductive Health
National Organization for Women
National Republican Coalition for Choice
National Women’s Health Network
National Women’s Law Center
Native American Women’s Health Education Resource Center
NOW Legal Defense and Education Fund
People For the American Way Action Fund
Planned Parenthood Federation of America
Population Action International
ProChoice Resource Center
Religious Coalition for Reproductive Choice
Society of Physicians for Reproductive Health and Choice
Union of American Hebrew Congregations
United Church Board for Homeland Ministries
Voters For Choice
Women of Reform Judaism, The Federation of Temple Sisterhood
Women’s Institute for Freedom of the Press
Women’s Law Project
Women’s Legal Defense Fund
Women’s Rabbinic Network
YWCA of the USA
Zero Population Growth
[304] Press release: “Aiming at the Right to Abortion, Congress Votes to Ban a Medical Procedure That Saves Women’s Lives.” PR Newswire, November 1, 1995. <www.prnewswire.com>
Distribution: To National and Health/Medical Editors …
Planned Parenthood Federation of America issued the following:
In an unprecedented intrusion by Congress into medical decisions, the U.S. House of Representatives today voted to ban a late abortion procedure designed to save women’s lives. The procedure, dilation and extraction (D&X), is extremely rare and done only in cases when the woman’s life is in danger or in cases of extreme fetal abnormality.
[305] Article: “Medicine Adds to Debate on Late-Term Abortion: Abortion Rights Leader Urges End to ‘Half Truths.’ ” By Diane M. Gianelli. American Medical News, March 3, 1997.
Page 3: “When [Ron] Fitzsimmons criticizes his movement for its handling of this issue, he points the finger at himself first. In November 1995, he was interviewed by Nightline … telling the reporter that women had these abortion only in the most extreme circumstances of life endangerment or fetal anomaly.”
[306] Article: “An Abortion Rights Advocate Says He Lied About Procedure.” By David Stout. New York Times, February 26, 1997. <www.nytimes.com>
Ron Fitzsimmons, the executive director of the National Coalition of Abortion Providers, said he intentionally misled in previous remarks about the procedure … because he feared that the truth would damage the cause of abortion rights. …
Mr. Fitzsimmons … appeared on Nightline on ABC and … said the procedure was used rarely and only on women whose lives were in danger or whose fetuses were damaged.
[307] On September 4, 2008, Just Facts contacted the ABC News Store to obtain a copy of this transcript and was told that the program aired on 11/7/95, was entitled “Late-Term Abortions,” and ABC’s legal department has not approved it for release. This was confirmed by a search of their archives which revealed that this episode is missing and that the shows surrounding it on 11/06/95 and 11/09/95 are available [<abcnewsstore.go.com>].
[308] Press release: “Capitol Hill Hearing Testimony, March 21, 1996, Diana Zuckerman, National Policy Director of Planned Parenthood to the House Judiciary Committee on the Constitution, Partial-Birth Abortion.” Planned Parenthood Federation of America, March 21, 1996.
We at Planned Parenthood are outraged that Congress is continuing to intrude into difficult and private medical decisions best left to women, families, and doctors. The attempt to ban dilation and extraction (D&X), a late abortion procedure that is used very rarely and in the most tragic circumstances, places women’s lives in jeopardy. …
The truth is that the D&X procedure is only used when the woman’s life or health is in danger or in cases of extreme fetal anomaly.
[309] Article: “The Facts on Partial-Birth Abortion; Both Sides Have Misled the Public.” By Ruth Padawer. Bergen Record, September 15, 1996. <northjersey.newspapers.com>
Doctors at Metropolitan Medical in Englewood estimate that their clinic alone performs 3,000 abortions a year on fetuses between 20 and 24 weeks, of which at least half are by intact dilation and evacuation. …
“I always try [a partial-birth abortion first],” said a Metropolitan Medical gynecologist, who, like every other provider interviewed for this article, spoke on condition of anonymity for fear of retribution. …
“We have an occasional amnio abnormality, but it’s a minuscule amount,” said one of the doctors at Metropolitan Medical, an assessment confirmed by another doctor there. “Most are Medicaid patients, black and white, and most are for elective, not medical, reasons: people who didn’t realize, or didn’t care, how far along they were. Most are teenagers.”
NOTE: This article alleges that “abortion foes” have also misled in this debate. Most of the points made to substantiate this statement are addressed in House report 104-267. One that is not is this statement: “In reality, only about 600, or 0.04 percent, of abortions of any type are performed after 26 weeks, according to the latest figures from Guttmacher.” Compare that with the following from American Medical News:
Accurate figures on second- and third-trimester abortions are elusive because a number of states don’t require doctors to report abortion statistics. For example, one-third of all abortions are said to occur in California, but the state has no reporting requirements. …
There is a particular debate over the number of third-trimester abortions. Former Surgeon General C. Everett Koop, MD, estimated in 1984 that 4,000 are performed annually. The abortion federation puts the number at 300 to 500. Dr. Haskell says that “probably Koop’s numbers are more correct.” [Article: “Shock-Tactic Ads Target Late-Term Abortion Procedure: Foes Hope Campaign Will Sink Federal Abortion Rights Legislation.” By Diane M. Gianelli. American Medical News, July 5, 1993.]
[310] Letter to the editor and response: “Abortion Numbers Questioned.” From the Management of Metropolitan Medical Associates, September 23, 1996. Bergen Record, October 2, 1996. <northjersey.newspapers.com>
The editor replies: The Record stands behind the story and rebuts the claims in Metropolitan Medical’s unsigned letter. …
Metropolitan Medical’s letter contradicts what two prominent staff physicians at the clinic, one of whom is also a high-ranking administrator, told Staff Writer Ruth Padawer independently of each other. The first physician said the clinic each week performs 60 to 100 abortions at 20 weeks gestation or later, or 3,000 to 5,000 a year. The second physician told Padawer that the clinic handles 3,000 such cases a year.
Both physicians also independently told Padawer that at least half the post-20 week abortions performed at the clinic were by the intact D&E [dilation and evacuation] method. …
As for the Metropolitan Medical’s claim that a quotation by one of its doctors was “erroneous”: Padawer read back to him all of his quotations, including the one about the Medicaid patients. She also read him the paragraph preceding and following the quotations. He confirmed the accuracy and context of each quotation.
[311] Article: “An Abortion Rights Advocate Says He Lied About Procedure.” By David Stout. New York Times, February 26, 1997. <www.nytimes.com>
Ron Fitzsimmons, the executive director of the National Coalition of Abortion Providers, said he intentionally misled in previous remarks about the procedure … because he feared that the truth would damage the cause of abortion rights. …
… Mr. Fitzsimmons recalled the night in November 1995, when he appeared on “Nightline” on ABC and “lied through my teeth” when he said the procedure was used rarely and only on women whose lives were in danger or whose fetuses were damaged. …
In the vast majority of cases, the procedure is performed on a healthy mother with a healthy fetus that is 20 weeks or more along, Mr. Fitzsimmons said.
[312] Article: “Medicine Adds to Debate on Late-Term Abortion: Abortion Rights Leader Urges End to ‘Half Truths.’ ” By Diane M. Gianelli. American Medical News, March 3, 1997.
What abortion rights supporters failed to acknowledge, Fitzsimmons said, is that the vast majority of these abortion are performed in the 20-plus week range on healthy fetuses and healthy mothers. “The abortion rights folks know it, the anti-abortion folks know it, and so, probably, does everyone else,” he said.
He knows it, he says, because when the bill to ban it came down the pike, he called around until he found doctors who did them.
“I learned right away that this was being done for the most part in cases that did not involve those extreme circumstances,” he said. …
[Quoting Fitzsimmons:] “When you’re a doctor who does these abortions and the leaders of your movement appear before Congress and go on network news and say these procedures are done in only the most tragic of circumstances, how do you think it makes you feel? You know they’re primarily done on healthy women and healthy fetuses, and it makes you feel like a dirty little abortionist with a dirty little secret.”
[313] Article: “Abortion: Activists Lied: Pro-Choice Advocates Admit to Deception.” Bergen Record, February 27, 1997. <www.nrlc.org>
“The spin out of Washington was that it was only done for medical necessity, even though we knew it wasn’t so,” said Renee Chelian, president of the National Coalition of Abortion Providers and a member of the National Abortion Federation who runs three abortion clinics in the Detroit area, “I kept waiting for the NAF [National Abortion Federation] to clarify it and they never did. I got caught up: What do we do about this secret? Who do we tell and what happens when we tell? But frankly, no one was asking me, so I didn’t have to worry.
[314] Article: “Possible Ban on Abortion Technique Leaves Doctors Uneasy.” By Mary Duenwald. New York Times, April 22, 2003. <www.nytimes.com>
One aspect of the debate has changed. When it began, some opponents of the ban said the targeted form of abortion was used only when a fetus had extreme abnormalities or a mother’s health was endangered by pregnancy. Now, both sides acknowledge that abortions done late in the second trimester, no matter how they are conducted, are most often performed to end healthy pregnancies because the woman arrived relatively late to her decision to abort.
A Guttmacher study from 1987 indicates that only 2 percent of abortions done after 16 weeks of pregnancy are done because of fetal abnormalities.
[315] Editorial: “Anti-Abortionists on Trial.” By the Editorial Board. New York Times, July 25, 2012. <www.nytimes.com>
“The overwhelming number of abortions occur well before 20 weeks; later abortions mostly often involve severely troubled pregnancies that pose risks to a woman’s health or life.”
[316] Video: “Pete Buttigieg Explains Why He’s Pro-Choice.” The View, February 6, 2020. <youtu.be>
Time marker 4:38:
If this is a late-term situation, then by definition, it’s one where a woman was expecting to carry the pregnancy to term. Then she gets the most, perhaps, devastating news of her life. We’re talking about families that may have picked out a name, may be assembling a crib, and they learn something excruciating, and are faced with this terrible choice.
[317] Transcript: Face the Nation. Hosted by John Dickerson. CBS, September 20, 2015. <www.cbsnews.com>
Dickerson: This week, the Senate is going to vote to impose a federal ban on late-term abortions. Do you support a federal limit on abortion at any stage of pregnancy?
Clinton: This is one of those really painful questions that people raise. And, obviously, it’s really emotional. I think that the kind of late-term abortions that take place are because of medical necessity. And, therefore, I would hate to see the government interfering with that decision. I think that, again, this gets back to whether you respect a woman’s right to choose or not. And I think that is what this whole argument once again is about.
[318] Article: “Separating Fact From Fiction in Abortion Talking Points.” By Meg Kelly. Washington Post, June 12, 2019. <www.washingtonpost.com>
“For women that are really in that difficult position, so-called late-term abortions—some people try to make [it as though] that commonly happens. That happens when a woman’s life is being threatened and the viability of the fetus as well is compromised.”
— Sen. Cory Booker (D-N.J.), in a town hall, April 16, 2019
[319] Article: “Julian Castro Calls for Surge in Federal Spending to End Homelessness.” By Michael Finnegan. Los Angeles Times, June 17, 2019. <www.latimes.com>
“Democratic presidential candidate Julian Castro called for a sharp rise in federal spending on housing for millions of Americans who are living on the street or struggling to pay rent.”
[320] Article: “Separating Fact From Fiction in Abortion Talking Points.” By Meg Kelly. Washington Post, June 12, 2019. <www.washingtonpost.com>
“The evidence over many years shows that to the extent that an abortion is performed after 20–24 weeks those are very very limited circumstances and necessary for the life of the mother or for other reasons.”
— Former housing and urban development secretary Julián Castro, on Meet the Press Daily, June 7, 2019
[321] Statement of U.S. Senator Jeanne Shaheen (D-NH). Congressional Record, February 25, 2019. Page S1418. <www.congress.gov>
“We must always remember that abortions that are performed later in pregnancy are most often done as the result of severe fetal diagnoses and the serious risks that pregnancy poses to the life of the mother.”
[322] Statement of U.S. Representative Diana DeGette (D-CO). Congressional Record, October 3, 2017. Page H7717. <www.congress.gov>
Madam Speaker, I rise for my former district director Chris and his wife, Bridget. This is their story. Bridget was pregnant with their very much-wanted second child. After the 20th week, they were stunned to learn that the brain stem of the fetus was not attached, and if the baby even survived, then the newborn would likely die within hours. …
… Ninety-nine percent of abortions are conducted before the 20-week mark. Virtually all the rest are just like this situation.
[323] Article: “Abortion Bill Draws GOP Outrage Against Va. Gov. Northam, Democratic Legislators.” By Gregory S. Schneider and Laura Vozzella. Washington Post, January 30, 2019. <www.washingtonpost.com>
Ofirah Yheskel, a spokeswoman for Northam, said the Republicans were mischaracterizing his remarks.
“No woman seeks a third-trimester abortion except in the case of tragic or difficult circumstances, such as a nonviable pregnancy or in the event of severe fetal abnormalities, and the governor’s comments were limited to the actions physicians would take in the event that a woman in those circumstances went into labor,” she said.
[324] Article: “ ‘Executing Babies’: Here Are the Facts Behind Trump’s Misleading Abortion Tweet.” By Denise Grady. New York Times, February 26, 2019. <www.nytimes.com>
“Less than 1 percent of all abortions are done after 24 weeks, and many are performed because the fetus has a fatal condition or the pregnant woman’s life or health is at severe risk.”
[325] Article: “Trent Franks Expands His DC Abortion Ban Nationwide.” By Laura Bassett. Huffington Post, May 17, 2013. <www.huffpost.com>
“According to the Centers for Disease Control and Prevention, late-term abortions are very rare. Slightly more than 1 percent of abortions are conducted after 24 weeks, and most of those cases result from a severe fetal anomaly or a health threat to the mother.”
[326] Webpage: “Facts are Important: Abortion Care Later in Pregnancy is Important to Women’s Health.” American College of Obstetricians and Gynecologists, February 2019. <bit.ly>
Many abortions that occur later in pregnancy involve fetal anomalies incompatible with life, such as anencephaly, the absence of the brain and cranium above the base of the skull, or limb-body wall complex, when the organs develop outside of the body cavity.ii In these cases, where death is likely before or shortly after birth, patients may decide whether to continue the pregnancy and deliver a nonviable fetus or have an abortion.
ii <rarediseases.info.nih.gov> †
NOTES:
[327] Article: “ ‘Four Takeaways From the DeSantis-Crist Debate in Florida’s Governor Race.” By Patricia Mazzei and Maggie Astor. New York Times, October 24, 2022. <www.nytimes.com>
He [Ron DeSantis] accused Mr. Crist of supporting abortion “up until the moment of birth.” That is a common Republican claim, but abortion until the moment of birth doesn’t exist, even in states without gestational limits. He also said Mr. Crist supported “dismemberment abortions,” a pejorative term for procedures performed later in pregnancy that, when they do happen, are often prompted by medical emergencies or severe fetal abnormalities.
[328] Article: “Method to End 20-Week Pregnancies Stirs a Corner of the Abortion Debate.” By Tamar Lewin. New York Times, July 5, 1995. <www.nytimes.com>
“We only know of two physicians who do this,” said Vicki Saporta, executive director of the National Abortion Federation, “and combined they do 450 a year.” …
This procedure is not taking place on live fetuses, the way it’s being portrayed,” Ms. Saporta said. “The fetal demise has already occurred, and most of these fetuses have severe abnormalities and were never healthy to start with.
[329] Article: “2nd Trimester Abortion: An Interview with W. Martin Haskell, MD.” Cincinnati Medicine, Fall 1993. <www.nrlc.org>
Page 19:
The D & X Procedure—Dilation and Extraction (D & X), a method for second trimester abortion up to 26 weeks, was developed in 1992 by Cincinnati physician W. Martin Haskell, MD. It is a modification of Dismemberment and Extraction (D & E) which has been used in the US since the 1970s. Haskell has performed more than 700 D & X procedures in his office.
Step One—The patient’s cervix is dilated to 9–11 mm over a period of two days using Dilapan hydroscopic dilators. The patient remains at home during the dilation period.
Step Two—In the operating room, patients are given Valium, the Dilapan are removed and the cervix is scrubbed. anesthetized and grasped with a tenaculum. Membranes are ruptured.
Step Three—The surgical assistant scans the fetus with ultrasound, locating the lower extremities.
Step Four—Using a large forcep, the surgeon opens and closes its jaws to firmly grasp a lower extremity. The surgeon turns the fetus if necessary and pulls the extremity into the vagina.
Step Five—The surgeon uses his fingers to deliver the opposite lower extremity, then the torso, shoulders, and upper extremities.
Step Six—The skull lodges at the internal cervical os [hole at the center of the cervix]. Usually there is not enough dilation for it to pass through. The fetus is spine up.
Step Seven—A right-handed surgeon slides the fingers of his left hand along the back of the fetus and hooks the shoulders of the fetus with the index and ring fingers (palm down). He slides the tip of his middle finger along the spine towards the skull while applying traction to the shoulder and lower extremities. The middle finger lifts and pushes the anterior cervical lip out of the way.
Step Eight—While maintaining this tension, the surgeon takes a pair of blunt curved scissors in the right hand. He advances the tip, curved down, along the spine and under his middle finger until he feels it contact the base of the skull under the tip of his middle finger. The surgeon forces the scissors into the base of the skull and spreads the scissors to enlarge the opening.
Step Nine—The surgeon removes the scissors and introduces a suction catheter into this hole and evacuates the skull contents.
Step Ten—With the catheter still in place, he applies traction to the fetus, removing it completely from the patient, then removes the placenta.
[330] Article: “Method to End 20-Week Pregnancies Stirs a Corner of the Abortion Debate.” By Tamar Lewin. New York Times, July 5, 1995. <www.nytimes.com>
Dr. Haskell, whose paper on how to perform the procedure was distributed to other doctors by the National Abortion Federation, said in a letter to Mr. Canady’s subcommittee: “Statements that fetuses are not dead until nearly the end of the procedure are not accurate. Death occurs early in the procedure if not before. Representations that fetuses are living, conscious, feeling pain, wiggling, kicking or trying to escape are totally fictitious.”
[331] Article: “Shock-Tactic Ads Target Late-Term Abortion Procedure: Foes Hope Campaign Will Sink Federal Abortion Rights Legislation.” By Diane M. Gianelli. American Medical News, July 5, 1993. <www.congress.gov>
Page S16795:
A letter to the Star-Tribune said the procedure shown “is only performed after fetal death when an autopsy is necessary or to save the life of the mother.” And the Morrisville, Vt., Transcript … quoted the abortion federation as providing similar information. “The fetus is dead 24 hours before the pictured procedure is undertaken,” the editorial stated.
But Dr. Haskell and another doctor [McMahon] who routinely use the procedure for late term abortions told AMNews that the majority of fetuses aborted this way are alive until the end of the procedure.
[332] Article: “Veto-Proof Majority in House Votes to Prohibit Late-Term Procedure.” By Diane M. Gianelli. American Medical News (a publication of the American Medical Association), November 20, 1995. <bit.ly>
Page 3 (of PDF):
Frequently quoted is testimony of a nurse, Brenda Shafer, RN, who witnessed three of these procedures in Dr. Haskell’s clinic and called it “the most horrifying experience of my life.
“The baby’s body was moving. His little fingers were clasping together. He was kicking his feet.” Afterwards, she said, “he threw the baby in a pan.” She said she saw the baby move. “I still have nightmares about what I saw.”
[333] Article: “Method to End 20-Week Pregnancies Stirs a Corner of the Abortion Debate.” By Tamar Lewin. New York Times, July 5, 1995. <www.nytimes.com>
“But anti-abortion groups point to statements in earlier news accounts, including a 1993 article in the American Medical News, a publication of the American Medical Association, that quoted the two doctors as saying, ‘The majority of fetuses aborted this way are alive until the end of the procedure.’ ”
[334] House report 104-267: “Partial-Birth Abortion Ban Act of 1995.” Judiciary Committee, U.S. House of Representatives, September 27, 1995. <www.gpo.gov>
Pages 5–6:
Dr. Martin Haskell and Dr. James McMahon, two abortionists who use the partial-birth abortion method, were interviewed by the American Medical News in 1993. These doctors “told the AMNews that the majority of fetuses aborted this way are alive until the end of the procedure.”14
Dr. Haskell and the National Abortion Federation disputed the accuracy of the AMNews article after the “Partial-Birth Abortion Ban Act” was introduced this year, claiming that out-of-context quotes were used.15 …
14 Diane M. Gianelli, “Shock-Tactic Ads Target Late-Term Abortion Procedure: Foes Hope Campaign Will Sink Federal Abortion Rights Legislation,” American Medical News, July 5, 1993, at 3, 21.
[335] Article: “Veto-Proof Majority in House Votes to Prohibit Late-Term Procedure.” By Diane M. Gianelli. American Medical News, November 20, 1995. <www.nrlc.org>
“The accuracy of the article was challenged, two years after publication, by Dr. Haskell and the National Abortion Federation, who told Congress the doctors were quoted ‘out of context.’ ”
[336] Letter: “Barbara Bolsen (Editor, American Medical News) to Charles T. Canady (Chairmen, Subcommittee on the Constitution, Judiciary Committee, U.S. House of Representatives).” July 11, 1995. <www.congress.gov>
Page H10633:
We have full documentation of these interviews, including tape recordings and transcripts. Enclosed is a transcript of the contested quotes that relate to the allegations of inaccuracies made against AMNews.
Let me also note that in the two years since publication of our story, neither the organization nor the physician who complained about the report in testimony to your committee has contacted the reporter or any editor at AMNews to complain about it. AMNews has a longstanding reputation for balance, fairness and accuracy in reporting, including reporting on abortion, an issue that is as divisive within medicine as it is within society in general. We believe that the story in question comports entirely with that reputation. …
AMN: Let’s talk first about whether or not the fetus is dead beforehand …
Haskell: No, it’s not. No, it’s really not. A percentage are for various numbers of reasons. Some just because of the stress—intrauterine stress during, you know, the two days that the cervix is being dilated. Sometimes the membranes rupture and it takes a very small superficial infection to kill a fetus in utero when the membranes are broken. And so in my case, I would think probably about a third of those are definitely are (sic) dead before I actually start to remove the fetus. And probably the other two-thirds are not.
AMN: Is the skull procedure also done to make sure that the fetus is dead so you’re not going to have the problem of a live birth?
Haskell: It’s immaterial. If you can’t get it out, you can’t get it out.
AMN: I mean, you couldn’t dilate further? Or is that riskier?
Haskell: Well, you could dilate further over a period of days.
AMN: Would that just make it … would it go from a 3-day procedure to a 4- or a 5-?
Haskell: Exactly. The point here is to effect a safe legal abortion. I mean, you could say the same thing about the D procedure. You know, why do you do the D procedure? Why do you crush the fetus up inside the womb? To kill it before you take it out?
Well, that happens, yes. But that’s not why you do it. You do it to get it out. I could do the same thing with a D procedure. I could put dilapan in for four or five days and say I’m doing a D procedure and the fetus could just fall out. But that’s not really the point. The point here is you’re attempting to do an abortion. And that’s the goal of your work, is to complete an abortion. Not to see how do I manipulate the situation so that I get a live birth instead.
AMN, wrapping up the interview: I wanted to make sure I have both you and (Dr.) McMahon saying “No” then. That this is misinformation, these letters to the editor saying it’s only done when the baby’s already dead, in case of fetal demise and you have to do an autopsy. But some of them are saying they’re getting that information from NAF [National Abortion Federation]. Have you talked to Barbara Radford or anyone over there? I called Barbara and she called back, but I haven’t gotten back to her.
Haskell: Well, I had heard that they were giving that information, somebody over there might be giving information like that out. The people that staff the NAF office are not medical people. And many of them when I gave my paper, many of them came in, I learned later, to watch my paper because many of them have never seen an abortion performed of any kind.
AMN: Did you also show a video when you did that?
Haskell: Yeah. I taped a procedure a couple of years ago, a very brief video, that simply showed the technique. The old story about a picture’s worth a thousand words.
AMN: As National Right to Life will tell you.
Haskell: Afterwards they were just amazed. They just had no idea. And here they’re rapid supporters of abortion. They work in the office there. And … some of them have never seen one performed….
[337] House report 104-267: “Partial-Birth Abortion Ban Act of 1995.” Judiciary Committee, U.S. House of Representatives, September 27, 1995. <frwebgate.access.gpo.gov>
Page 6:
In a letter to the Honorable Charles T. Canady, Dr. James McMahon, an abortionist who uses the partial-birth abortion method, implies that large doses of analgesia kill the baby before the doctor begins delivery. He states:
The fetus feels no pain through the entire series of procedures. This is because the mother is given narcotic analgesia at a dose based upon her weight. The narcotic is passed, via the placenta, directly into the fetal bloodstream. Due to the enormous weight difference, a medical coma is induced in the fetus. There is a neurological fetal demise. There is never a live birth.18 …
18 Letter from James T. McMahon, M.D., to Congressman Charles T. Canady (June 23, 1995) (on file with the Subcomm. on the Constitution of the House Comm. on the Judiciary).
[338] Newsletter: “Washington Report.” By Michael Scott. American Academy of Anesthesiologists, May 1996. <www.asahq.org>
On March 21, ASA [American Academy of Anesthesiologists] President Norig Ellison, M.D., testified before a subcommittee of the House Judiciary Committee on the issue of the effect of anesthetics on the fetus in late-term abortions. Also participating in the hearing were David J. Birnbach, M.D., President-Elect of the Society for Obstetric Anesthesia and Perinatology and Professor of Anesthesiology at St. Luke’s Roosevelt Medical Center, New York, New York; David H. Chestnut, M.D., Chair of the Department of Anesthesiology, University of Alabama Birmingham Hospital, Birmingham, Alabama; and Jean A. Wright, M.D., Associate Professor, Department of Pediatrics and Anesthesiology, Emory University, Atlanta, Georgia.
Testimony of all the anesthesiology witnesses was consistent, disputing at length the claim that anesthesia given to the mother during a late-term abortion caused neurological demise of the fetus. All of the witnesses expressed concern that widespread dissemination of this false claim by the media has caused many women to question whether to undergo necessary surgery during pregnancy, for fear of injuring the unborn child.
[339] Transcript: “Testimony of Jill L. Stanek, Mokena, IL.” Subcommittee on the Constitution, Judiciary Committee, U.S. House of Representatives, July 20, 2000. Pages 34–39. <commdocs.house.gov>
Pages 35–36:
My name is Jill Stanek, and I am a registered nurse who has worked in the Labor and Delivery Department at Christ Hospital in Oak Lawn, Illinois, for the past 5 years. Christ Hospital performs abortions on women in their second or even third trimesters of pregnancy. Sometimes the babies aborted are healthy, and sometimes they are not. …
… It is not uncommon for a live aborted baby to linger for an hour or two or even longer. One of these babies was known to live for almost an entire 8-hour shift.
In the event that a baby is aborted alive, he or she receives no medical assessments or care, but is given only what the Christ Hospital calls “comfort care.” Comfort care is defined as keeping the baby warm in a blanket until he or she dies, although even this so-called compassion is not always provided. It is not required that these babies be held during their short lives.
One night, a nursing co-worker was taking an aborted Down’s syndrome baby who was born alive to our Soiled Utility Room because his parents did not want to hold him and she did not have time to hold him. I could not bear the thought of this suffering child dying alone in a Soiled Utility Room, so I cradled and rocked him for the 45 minutes that he lived. …
Other co-workers have told me upsetting stories about live aborted babies whom they have cared for. I was told about an aborted baby who was supposed to have spina bifida, but was delivered with an intact spine. Another nurse is haunted by the memory of an aborted baby who came out weighing much more than expected—almost 2 pounds. She is haunted because she doesn’t know if she made a mistake by not getting that baby any medical help. A support associate told me about a live aborted baby who was left to die on a counter in our Soiled Utility room wrapped in a disposable towel. This baby was accidentally thrown in the garbage. Later, when they were going through the trash trying to find the baby, the baby fell out of the towel and onto the floor.
I was recently told about a situation by a nurse who said, “I can’t stop thinking about it.” She had a patient who was 23-plus weeks pregnant, and it did not look as if her baby would continue to be able to live inside of her. The baby was healthy and had up to a 39 percent chance of survival, according to our national statistics. But the patient chose to abort. The baby was born alive. … After delivery, the baby, who showed early signs of thriving—her Apgars improved—was merely wrapped in a blanket and kept in the Labor and Delivery Department until she died two and a half hours later.
[340] Transcript: “Testimony of Allison Baker, Charlottesville, VA.” Subcommittee on the Constitution, Judiciary Committee, U.S. House of Representatives, July 20, 2000. Pages 40–43. <commdocs.house.gov>
Pages 40–41:
I am also an RN. I worked at Christ Hospital for a year between the time of August 1998 to August 1999. I am now presently a pediatric nurse in Charlottesville.
During this time, I witnessed three cases. When I first started, I was on day shift. I walked into the Soiled Utility Room to throw something away, and laying on the metal part of the table with nothing underneath, there was a fetus, a baby, moving vigorously, just laying there.
I went out to find the nurse who was responsible for this baby, and she said that the mother had been what they call a therapeutic abortion, as Jill had explained, and that she just didn’t have time to do anything with the baby at the time, and that if I could, could I wrap the baby and put the baby in a warmer.
So I went to the Soiled Utility Room, wrapped the baby, and held the baby and found a warmer and placed the baby in the warmer. And for about two and a half hours, the baby maintained a heartbeat, the baby was alive. …
The next case that I actually participated in was I had come on to shift and there was a patient that had delivered a baby, a 20-week fetus who had spina bifida. The baby, once again, was alive and the baby had a heartbeat. It took an hour and 45 minutes for this baby to finally expire. …
The last case that I experienced while I was there was a 16-week fetus that was aborted, and the baby was supposed to have had Down’s. And the baby at 16 weeks was born with a heartbeat, and the parents thought that the baby would die right away because it was so early. The baby ended up living for approximately 45 minutes, and during this time, the parents were very upset and kept questioning me and other nurses: how come their baby wasn’t dead, when was their baby going to die, why was their baby alive?
[341] Article: “Bill Proposes Care for Fetus After Abortion.” By Dave McKinney. Chicago Sun-Times. March 31, 2001. <chicago.suntimes.com>
“A spokesman for Christ Hospital’s parent, Advocate Health Care, said it provides ‘compassionate care’ for its patients and estimated that between 10 percent and 20 percent of fetuses with genetic defects that are aborted survive for short periods outside the womb.”
[342] Calculated with data from the paper: “Termination of Pregnancy for Fetal Anomaly: A Population-Based Study 1995 to 2004.” By M. Wyldes. BJOG [British Journal of Obstetrics and Gynaecology], April 2007. Pages 639–642. <obgyn.onlinelibrary.wiley.com>
Page 639:
Termination of pregnancy for fetal anomaly (TOPFA) is a rare outcome of pregnancy and a principal element of fetal medicine. It is an important option for women in the UK undergoing screening for fetal anomalies during pregnancy and commonly chosen when a lethal or seriously handicapping condition is diagnosed prenatally. The 1990 amendment to the Abortion Act has no gestation limit defined for cases of TOPFA following prenatal diagnosis (category E).
The Office for National Statistics publishes an annual reference volume of data on legally induced abortions in England and Wales. Data are collected using the notification of abortion form (Form HSA4) on cases performed under the Abortion Act 1967. Cases are categorised by the statutory grounds on which they are undertaken. Category E is the most relevant for identifying TOPFA and refers to cases “where there is a substantial risk that if the child were born it would suffer from such physical or mental abnormalities as to be seriously handicapped.” The only subanalysis of this group within the annual reference volume is to give details of the type of congenital malformation or other condition. …
The West Midlands Congenital Anomaly Register (WMCAR) was setup in June 1994 and is administered by the West Midlands Perinatal Institute.
Page 640:
The study population was births to West Midlands residents delivered between 1995 and 2004. …
For the purposes of this study, a TOPFA is defined as a legally induced termination regardless of gestation or out-come following a prenatal diagnosis of a congenital anomaly. …
There were 3189 cases of TOPFA notified to the WMCAR and born to West Midlands residents between 1995 and 2004. …
There were 646 342 registered births and 808 236 conceptions during this period in the West Midlands. The prevalence of TOPFA was 49.3 per 10 000 (1 in 203) registerable births and 39.5 per 10 000 (1 in 253) conceptions.
Gestations of TOPFAs ranged from 8 to 40 weeks, median 19 weeks. …
Thirty-nine percent of TOPFAs were for chromosomal anomaly; 25% for malformations of multiple systems; 23%for neural tube defects; 5% for renal problems; and 5% for cardiac defects. …
Of the 102 live births, the gestation ranged from 17 to 33with a median of 21 weeks. The survival duration for liveborn TOPFAs was a median of 80 minutes. Thirty-seven cases survived for 1 hour or less and six cases survived 6 hours or more.
Page 641: “Within our study 3.2% of TOPFAs result in a live birth.”
CALCULATIONS:
[343] Article: “Abortion: Every Sixth Foetus Showed Signs of Life: Midwives’ Chairwoman Says ‘a Sorrowful Situation.’ ” Edited by Julian Isherwood. Politiken, December 14, 2012. <politiken.dk>
Previously, conventional wisdom has suggested that 10 per cent of foetuses gasped or showed other signs of life following a late term abortion between the 12th and 22nd week of pregnancy.
But statistics from Denmark’s second largest maternity clinic at the Aarhus University Hospital Skejby show that out of 70 late terminations between August 2011 and November 2012, 11—or 16 per cent—showed signs of life.
[344] Report: “Mortality Records with Mention of Termination of Pregnancy.” U.S. Centers for Disease Control and Prevention, National Center for Health Statistics, April 11, 2016. <www.cdc.gov>
The information presented below comes from the National Vital Statistics System (NVSS) Mortality Data. Data available for 2003 and subsequent years includes not only causes of death coded to ICD [International Classification of Diseases]-10, but also the original text describing the causes of death as reported on the death certificate by the cause-of-death certifier (usually a physician, medical examiner or coroner). With regard to infant deaths, the NVSS Mortality Data only include deaths occurring to those infants born alive; fetal deaths (stillbirths) are not included. The legal definition of live birth includes any sign of life, e.g., breath, heartbeat, pulsation of the umbilical cord, or definite movement of voluntary muscles. …
Infant deaths for the 12 year period 2003–2014 assigned to code ICD-10 code P96.4—Termination of pregnancy, affecting fetus and newborn were reviewed. During this period there were 315,392 infant deaths and 49,126,572 live births. The purpose of this analysis is to provide some additional information regarding infant deaths with this cause of death code. This category includes both spontaneous terminations of pregnancy and induced terminations of pregnancy. Analysis of the text as reported by the cause-of-death certifier show that of 588 deaths with mention of P96.4, 143 (24.3%) could definitively be classified as involving an induced termination. A list of the terms on which this number is based is shown below. Most of the remaining deaths are clearly spontaneous. However, it is possible that this number (143) underestimates the total number of deaths involving induced termination. In some cases, when a vague term such as “termination of pregnancy” was reported as due to a severe congenital anomaly or maternal complication, it was impossible to determine whether the pregnancy terminated spontaneously as the result of the anomaly or complication, or whether the mother elected to terminate because of the anomaly or complication. …
The distribution of age at death for deaths involving induced terminations are as follows:
|
Age at Death |
Frequency |
Percent |
|
<10 minutes |
25 |
17.5 |
|
10–59 minutes |
35 |
24.5 |
|
1–4 hours |
68 |
47.6 |
|
5–23 hours |
9 |
6.3 |
|
1 day or more |
6 |
4.2 |
[345] Article: “Fetus.” By Frank D. Allan. Encyclopedia of Human Biology (Volume 3). Academic Press, 1997.
Page 962:
Attempts to suckle have been seen in utero and in aborted fetuses of 3 months. …
Reflexes that develop during the third month involve the mouth and the head…. Electrical activity of the nervous system is discernible at the same time, but periods of electrical silence can occur up to midterm.
[346] Paper: “An Infant Who Survived Abortion and Neonatal Intensive Care.” By P. Clarke & others. Journal of Obstetrics and Gynaecology, January 2005. Pages 73–74. <www.tandfonline.com>
Page 73: “A 24-week gestation male infant was born alive in November 2002, several days after repeated attempts at medical termination of pregnancy.”
[347] Article: “Boy Is Aborted 3 Times and Lives.” By Lois Rogers and Sarah-Kate Templeton. London Times, February 13, 2005. <www.thetimes.co.uk>
“A baby survived at least three attempts to abort it from the womb and was born alive at 24 weeks old. … Now two years old and healthy, he is the first long-term abortion survivor to have been born so prematurely.”
[348] Article: “We’re Twinseparable! Happy with His Brother, the Boy Who Refused to Die.” By Lucy Laing. London Daily Mail, November 3, 2007. <www.dailymail.co.uk>
When doctors found that Gabriel was weaker than his brother, with an enlarged heart, and believed he was going to die in the womb, his mother Rebecca Jones had to make a heartbreaking decision. …
Mrs. Jones decided to let doctors operate to terminate Gabriel’s life.
Firstly they tried to sever his umbilical cord to cut off his blood supply, but the cord was too strong.
They then cut Mrs. Jones’s placenta in half so that when Gabriel died, it would not affect his twin brother. …
But at her 20-week scan, doctors had some devastating news. One of the boys was half the size of his brother. …
Then doctors said his heart was three times normal size….
… When Mrs. Jones reached 31 weeks doctors carried out a caesarian to deliver the twins. … Both were kept in hospital, but since going home they have thrived. At seven months, Ieuan weighs 15lb and Gabriel 12lb 6oz.
[349] Article: “Mother’s Anger Turns to Delight After Her Baby Survives an Abortion.” By Liz Hull. London Daily Mail, June 5, 2008. <www.dailymail.co.uk>
[T]heir first son had died of the condition and the second was born with serious kidney damage.
So when Finley’s mother … became pregnant while on the Pill, she and her fiance … made the agonising decision to abort this child. …
“Deciding to terminate at eight weeks was just utterly horrible but I couldn’t cope with the anguish of losing another baby,” …
… Eventually her doctor sent her for a scan—and she discovered she was 19 weeks pregnant. …
Her first baby, Thane, had lived for only 20 minutes….
Her second son … was born with a similar condition. He survives on one kidney.
[D]octors told the couple … that this child was likely to survive, so they decided he deserved a chance.
And in November, Finley was born three weeks premature….
He had minor kidney damage but is expected to lead a normal life.
[350] Article: “In Debate on Abortion, 2 Girls Make It Real.” By Tamar Lewin. New York Times, October 27, 1991. <www.nytimes.com>
Ms. DePaul will not identify Gianna’s birth mother, the doctor who performed the abortion, the clinic or the nurse who, she said, rescued Gianna by transferring her to a hospital nursery. But to support her story she released some of the medical records from the adoption, including a section called “Complications of Birth,” which has the notation, “Born during saline abortion. “
[351] Transcript: “Testimony of Gianna Jessen.” Subcommittee on the Constitution, Judiciary Committee, U.S. House of Representatives, July 20, 2000. <commdocs.house.gov>
Page 54: “I … was delivered alive on April 6, 1977, at 6 a.m. in a southern California abortion clinic.”
[352] Article: “ ‘I Survived an Abortion Attempt.’ ” By Jane Elliott. BBC News, December 6, 2005. <news.bbc.co.uk>
“She has cerebral palsy as a direct result of the procedure carried out on her in the womb. … She started to walk with leg braces and by the age of four was walking with the aid of a walker—now she walks without any assistance.”
[353] Webpage: “Gianna Jessen.” Accessed August 2008 at <www.giannajessen.com>
“On April 30, 2005 she completed her first 26.2 mile marathon…. On April 23, 2006 she completed the London Marathon as well. … In fact she has run a marathon, is an accomplished singer and writer and travels the world to campaign against abortion.”
[354] Born-Alive Infants Protection Act of 2001. Congressional Record, March 12, 2002. Pages 792–797. <www.govinfo.gov>
Page 796:
The SPEAKER pro tempore (Mr. STEARNS). The question is on the motion offered by the gentleman from Wisconsin (Mr. SENSENBRENNER) that the House suspend the rules and pass the bill, H.R. 2175 [Born-Alive Infants Protection Act].
The question was taken.
The SPEAKER pro tempore. In the opinion of the Chair, two-thirds of those present have voted in the affirmative.
[355] Born-Alive Infants Protection Act of 2001. Congressional Record, July 18, 2002. Page 7084. <www.gpo.gov>
Page 7084:
There being no objection, the Senate proceeded to consider the bill.
Mr. REID. Mr. President, I ask unanimous consent that the bill be read the third time and passed, the motion to reconsider be laid upon the table, and that any statements relating to the bill be printed in the RECORD.
The PRESIDING OFFICER. Without objection, it is so ordered.
The bill (H.R. 2175) was read the third time and passed.
[356] Public Law 107-207: “Born-Alive Infants Protection Act of 2002.” 107th United States Congress. Signed into law by President George W. Bush on August 5, 2002. <www.congress.gov>
An Act
To protect infants who are born alive. [H.R. 2175] …
(a) In determining the meaning of any Act of Congress, or of any ruling, regulation, or interpretation of the various administrative bureaus and agencies of the United States, the words “person”, “human being”, “child”, and “individual”, shall include every infant member of the species homo sapiens who is born alive at any stage of development.
(b) As used in this section, the term “born alive”, with respect to a member of the species homo sapiens, means the complete expulsion or extraction from his or her mother of that member, at any stage of development, who after such expulsion or extraction breathes or has a beating heart, pulsation of the umbilical cord, or definite movement of voluntary muscles, regardless of whether the umbilical cord has been cut, and regardless of whether the expulsion or extraction occurs as a result of natural or induced labor, cesarean section, or induced abortion.
(c) Nothing in this section shall be construed to affirm, deny, expand, or contract any legal status or legal right applicable to any member of the species homo sapiens at any point prior to being “born alive” as defined in this section.
[357] House Resolution 962: “Born-Alive Abortion Survivors Protection Act.” U.S. House of Representatives, 116th Congress (2019–2020). Accessed July 6, 2019 at <www.congress.gov>
Sponsor: Rep. Wagner, Ann [R–MO–2] (Introduced 02/05/2019)
(a) Requirements for health care practitioners.—In the case of an abortion or attempted abortion that results in a child born alive:
(1) Degree of Care Required; Immediate Admission to a Hospital.—Any health care practitioner present at the time the child is born alive shall—
(A) exercise the same degree of professional skill, care, and diligence to preserve the life and health of the child as a reasonably diligent and conscientious health care practitioner would render to any other child born alive at the same gestational age; and
(B) following the exercise of skill, care, and diligence required under subparagraph (A), ensure that the child born alive is immediately transported and admitted to a hospital.
(2) Mandatory Reporting of Violations.—A health care practitioner or any employee of a hospital, a physician’s office, or an abortion clinic who has knowledge of a failure to comply with the requirements of paragraph (1) shall immediately report the failure to an appropriate State or Federal law enforcement agency, or to both.
(b) Penalties.—
(1) In General.—Whoever violates subsection (a) shall be fined under this title, imprisoned for not more than 5 years, or both.
(2) Intentional Killing of Child Born Alive.—Whoever intentionally performs or attempts to perform an overt act that kills a child born alive described under subsection (a), shall be punished as under section 1111 of this title for intentionally killing or attempting to kill a human being.
(c) Bar to prosecution.—The mother of a child born alive described under subsection (a) may not be prosecuted for a violation of this section, an attempt to violate this section, a conspiracy to violate this section, or an offense under section 3 or 4 of this title based on such a violation.
[358] Senate Bill 311: “Born-Alive Abortion Survivors Protection Act.” U.S. Senate, 116th Congress (2019–2020). Accessed July 6, 2019 at <www.congress.gov>
Sponsor: Sen. Sasse, Ben [R–NE] (Introduced 01/31/2019) …
(a) Requirements for health care practitioners.—In the case of an abortion or attempted abortion that results in a child born alive:
(1) Degree of Care Required; Immediate Admission to a Hospital.—Any health care practitioner present at the time the child is born alive shall—
(A) exercise the same degree of professional skill, care, and diligence to preserve the life and health of the child as a reasonably diligent and conscientious health care practitioner would render to any other child born alive at the same gestational age; and
(B) following the exercise of skill, care, and diligence required under subparagraph (A), ensure that the child born alive is immediately transported and admitted to a hospital.
(2) Mandatory Reporting of Violations.—A health care practitioner or any employee of a hospital, a physician’s office, or an abortion clinic who has knowledge of a failure to comply with the requirements of paragraph (1) shall immediately report the failure to an appropriate State or Federal law enforcement agency, or to both.
(b) Penalties.—
(1) In General.—Whoever violates subsection (a) shall be fined under this title, imprisoned for not more than 5 years, or both.
(2) Intentional Killing of Child Born Alive.—Whoever intentionally performs or attempts to perform an overt act that kills a child born alive described under subsection (a), shall be punished as under section 1111 of this title for intentionally killing or attempting to kill a human being.
(c) Bar to prosecution.—The mother of a child born alive described under subsection (a) may not be prosecuted for a violation of this section, an attempt to violate this section, a conspiracy to violate this section, or an offense under section 3 or 4 of this title based on such a violation.
[359] Calculated with data from vote 27: “Cloture on the Motion to Proceed: Born-Alive Abortion Survivors Protection Act.” U.S. Senate, February 25, 2019. <www.senate.gov>
Required For Majority: 3/5 … Vote Result: Cloture on the Motion to Proceed Rejected …
|
Party |
Voted “Yes” |
Voted “No” |
Voted “Present” or Did Not Vote † |
|||
|
Number |
Portion |
Number |
Portion |
Number |
Portion |
|
|
Republican |
50 |
94% |
0 |
0% |
3 |
6% |
|
Democrat |
3 |
7% |
42 |
93% |
0 |
0% |
|
Independent |
0 |
0% |
2 |
100% |
0 |
0% |
|
NOTE: † Voting “Present” is effectively the same as not voting. |
||||||
[360] Calculated with data from vote 29: “Born-Alive Abortion Survivors Protection Act.” U.S. House of Representatives, January 11, 2023. <clerk.house.gov>
|
Party |
Voted “Yes” |
Voted “No” |
Voted “Present” or Did Not Vote† |
|||
|
Number |
Portion |
Number |
Portion |
Number |
Portion |
|
|
Republican |
219 |
99% |
0 |
0% |
3 |
1% |
|
Democrat |
1 |
0.5% |
210 |
99% |
1 |
0.5% |
|
NOTE: †Voting “Present” is effectively the same as not voting. |
||||||
[361] Webpage: “Cosponsors of Senate Bill 204: Born-Alive Abortion Survivors Protection Act.” U.S. Senate, 118th Congress (2022–2023). Accessed October 5, 2023 at <www.congress.gov>
“Cosponsor statistics: 38 current … Republican [=] 38”
[362] Webpage: “Actions Overview: S.204 — Born-Alive Abortion Survivors Protection Act.” U.S. Senate, 118th Congress (2022–2022). Accessed October 5, 2023 at <www.congress.gov>
“02/01/2023 — Introduced in Senate”
[363] Senate Bill 1095: “An Act Concerning Infants Who Are Born Alive.” State of Illinois, 92nd General Assembly, 2001. <www.ilga.gov>
(a) In determining the meaning of any statute or of any rule, regulation, or interpretation of the various administrative agencies of this State, the words “person”, “human being”, “child”, and “individual” include every infant member of the species homo sapiens who is born alive at any stage of development.
(b) As used in this Section, the term “born alive”, with respect to a member of the species homo sapiens, means the complete expulsion or extraction from its mother of that member, at any stage of development, who after that expulsion or extraction breathes or has a beating heart, pulsation of the umbilical cord, or definite movement of voluntary muscles, regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of natural or induced labor, cesarean section, or induced abortion.
(c) A live child born as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law.
[364] Senate Bill 1662: “An Act Concerning Infants Who Are Born Alive.” State of Illinois, 92nd General Assembly, 2002. <www.ilga.gov>
NOTE: The operative language is the same as the bill quoted in the footnote above.
[365] Vote on Senate Bill 1095: “An Act Concerning Infants Who Are Born Alive.” State of Illinois Senate, 92nd General Assembly, March 30, 2001. <www.ilga.gov>
“34 Yeas … 5 Nays … 13 Present … P[resent] Obama”
NOTE: In the Illinois legislature, a vote of ‘Present” has the same effect as a vote against a bill. This was implicitly stated by Obama in a debate with Alan Keyes on October 12, 2004 when he asserted that “21 other senators, Democrat and Republican … objected to the bill.” As shown in this vote record and the next, only by counting the “Present” votes can the number of 22 be reached.
[366] Vote on Senate Bill 1662: “An Act Concerning Infants Who Are Born Alive.” State of Illinois Senate, 92nd General Assembly, April 4, 2002. <www.ilga.gov>
“30 Yeas … 12 Nays … 10 Present … N[ay] Obama”
[367] Born-Alive Infants Protection Act of 2001. Congressional Record, March 12, 2002. Pages 792–797. <www.govinfo.gov>
Page 796:
The SPEAKER pro tempore (Mr. STEARNS). The question is on the motion offered by the gentleman from Wisconsin (Mr. SENSENBRENNER) that the House suspend the rules and pass the bill, H.R. 2175 [Born-Alive Infants Protection Act].
The question was taken.
The SPEAKER pro tempore. In the opinion of the Chair, two-thirds of those present have voted in the affirmative.
[368] Born-Alive Infants Protection Act of 2001. Congressional Record, July 18, 2002. Page 7084. <www.gpo.gov>
Page 7084:
There being no objection, the Senate proceeded to consider the bill.
Mr. REID. Mr. President, I ask unanimous consent that the bill be read the third time and passed, the motion to reconsider be laid upon the table, and that any statements relating to the bill be printed in the RECORD.
The PRESIDING OFFICER. Without objection, it is so ordered.
The bill (H.R. 2175) was read the third time and passed.
[369] Public Law 107-207: “Born-Alive Infants Protection Act of 2002.” 107th United States Congress. Signed into law by President George W. Bush on August 5, 2002. <www.congress.gov>
An Act
To protect infants who are born alive. [H.R. 2175] …
(a) In determining the meaning of any Act of Congress, or of any ruling, regulation, or interpretation of the various administrative bureaus and agencies of the United States, the words “person”, “human being”, “child”, and “individual”, shall include every infant member of the species homo sapiens who is born alive at any stage of development.
(b) As used in this section, the term “born alive”, with respect to a member of the species homo sapiens, means the complete expulsion or extraction from his or her mother of that member, at any stage of development, who after such expulsion or extraction breathes or has a beating heart, pulsation of the umbilical cord, or definite movement of voluntary muscles, regardless of whether the umbilical cord has been cut, and regardless of whether the expulsion or extraction occurs as a result of natural or induced labor, cesarean section, or induced abortion.
(c) Nothing in this section shall be construed to affirm, deny, expand, or contract any legal status or legal right applicable to any member of the species homo sapiens at any point prior to being ‘born alive’ as defined in this section.
[370] Transcript: “Alan Keyes and Barack Obama Debate.” Moderated by Jim Anderson. Illinois Radio Network, October 12, 2004. <www.keyesarchives.com>
Keyes: Well, I think it’s very clear. The Born Alive Infant Protection Act that was aimed at making sure that children born alive after an abortion procedure would not be set aside to die like garbage—when babies at exactly the same stage of development are being accessed and then saved right there down the hall in the same hospitals where they are boasting about their ability to save preemies. I think that we have to take seriously the testimony of people like Jill Stanek and others, and not pretend that this problem does not exist. …
And I think that’s a travesty. Senator [Obama] ignored that travesty, not once, not twice, but three times on the plea now, I suppose, that this problem does not exist. I guess he’s calling the nurses involved liars.
Obama: … You know, if Ambassador Keyes had called me up, he could have saved himself a trip because existing Illinois law mandates that any infant that has a chance for survival is provided life-saving treatment. Not only that, you’ve got to have a second doctor there to certify that in fact that is the case. That continues to be the case, that is current law today, as it should be.
Now, the bill that was put forward was essentially a way of getting around Roe vs. Wade, which is why 21 other senators, Democrat and Republican, why the Illinois Medical Society objected to the bill. At the federal level there was a similar bill that passed because it had an amendment saying this does not encroach on Roe vs. Wade. I would have voted for that bill.
[371] Senate Bill 1082: “An Act Concerning Infants Who Are Born Alive.” State of Illinois Senate, 93rd General Assembly, 2003. <www.ilga.gov>
NOTE: The operative language is the same as in the two other Illinois bills cited above: Senate Bill 1095 (2001) and Senate Bill 1662 (2002).
[372] “Amendment to Senate Bill 1082.” Filed by Senator Richard J. Winkel, Jr. (Republican). State of Illinois Senate, 93rd General Assembly, March 11, 2003. <www.ilga.gov>
Amend Senate Bill 1082 on page 1, by replacing lines 24 through 26 with the following:
“(c) Nothing in this Section shall be construed to affirm, deny, expand, or contract any legal status or legal right applicable to any member of the species homo sapiens at any point prior to being born alive as defined in this Section.”
[373] “Status of Senate Bill 1082.” State of Illinois Senate, 93rd General Assembly, 2005. <www.ilga.gov>
|
Date |
Chamber |
Action |
|
3/11/2003 |
Senate |
Senate Committee Amendment No. 1 Filed with Secretary by Sen. Richard J. Winkel, Jr. |
|
3/11/2003 |
Senate |
Senate Committee Amendment No. 1 Referred to Rules |
|
3/12/2003 |
Senate |
Senate Committee Amendment No. 1 Rules Refers to Health & Human Services |
[374] Webpage: “Health & Human Services Committee–Members.” State of Illinois Senate, 93rd General Assembly. Accessed July 2008 at <www.ilga.gov>
“Chairperson: Barack Obama [Democrat]”
[375] Senate committee action report: “Senate Bill 1082.” Illinois Senate Committee on Health and Human Services, March 12, 2003. <www.nrlc.org>
“Final Action … DPA [Do Pass As Amended] … Obama, Barack C [Chairman] D [Democrat] … No … Hunter, Mattie VC [Vice-Chairman] D … Crotty, M. Maggie D … No … Garrett, Susan D … No … Ronen, Carol D … No … Schoenberg, Jeffrey D … No … Total—4 Yes, 6 No”
[376] Article: “Lawmakers Approve Abortion-Friendly Legislation.” By Kristy Hessman. Associated Press, March 13, 2003.
Also on Thursday, the [Illinois] Senate Health and Human Services Committee rejected a bill that declares any fetus with a beating heart or muscle movement outside the womb as “born alive.” …
The sponsor, Sen. Rick Winkel, R-Champaign, said the bill is modeled after a recent federal policy that defines a “born-alive” infant. …
Winkel’s bill got four “yes” votes and six “no” votes. …
The bills are … SB1082….
[377] “Executive Order on Protecting Vulnerable Newborn and Infant Children.” By Donald Trump. White House, September 25, 2020. <www.federalregister.gov>
Section 1. Purpose. Every infant born alive, no matter the circumstances of his or her birth, has the same dignity and the same rights as every other individual and is entitled to the same protections under Federal law. Such laws include the Emergency Medical Treatment and Labor Act (EMTALA), 42 U.S.C. 1395dd, which guarantees, in hospitals that have an emergency department, each individual’s right to an appropriate medical screening examination and to either stabilizing treatment or an appropriate transfer. They also include section 504 of the Rehabilitation Act (Rehab Act), 29 U.S.C. 794, which prohibits discrimination against individuals with disabilities by programs and activities receiving Federal funding. In addition, the Born-Alive Infants Protection Act, 1 U.S.C. 8, makes clear that all infants born alive are individuals for purposes of these and other Federal laws and are therefore afforded the same legal protections as any other person. Together, these laws help protect infants born alive from discrimination in the provision of medical treatment, including infants who require emergency medical treatment, who are premature, or who are born with disabilities. Such infants are entitled to meaningful and non-discriminatory access to medical examination and services, with the consent of a parent or guardian, when they present at hospitals receiving Federal funds.
Despite these laws, some hospitals refuse the required medical screening examination and stabilizing treatment or otherwise do not provide potentially lifesaving medical treatment to extremely premature or disabled infants, even when parents plead for such treatment. Hospitals might refuse to provide treatment to extremely premature infants—born alive before 24 weeks of gestation—because they believe these infants may not survive, may have to live with long-term disabilities, or may have a quality-of-life deemed to be inadequate. Active treatment of extremely premature infants has, however, been shown to improve their survival rates. And the denial of such treatment, or discouragement of parents from seeking such treatment for their children, devalues the lives of these children and may violate Federal law.
Sec. 2. Policy. It is the policy of the United States to recognize the human dignity and inherent worth of every newborn or other infant child, regardless of prematurity or disability, and to ensure for each child due protection under the law.
Sec. 3. (a) The Secretary of Health and Human Services (Secretary) shall ensure that individuals responsible for all programs and activities under his jurisdiction that receive Federal funding are aware of their obligations toward infants, including premature infants or infants with disabilities, who have an emergency medical condition in need of stabilizing treatment, under EMTALA and section 504 of the Rehab Act, as interpreted consistent with the Born-Alive Infants Protection Act. In particular, the Secretary shall ensure that individuals responsible for such programs and activities are aware that they are not excused from complying with these obligations, including the obligation to provide an appropriate medical screening examination and stabilizing treatment or transfer, when extremely premature infants are born alive or infants are born with disabilities. The Secretary shall also ensure that individuals responsible for such programs and activities are aware that they may not unlawfully discourage parents from seeking medical treatment for their infant child solely because of their infant child’s disability. The Secretary shall further ensure that individuals responsible for such programs and activities are aware of their obligations to provide stabilizing treatment that will allow the infant patients to be transferred to a more suitable facility if appropriate treatment is not possible at the initial location.
(b) The Secretary shall, as appropriate and consistent with applicable law, ensure that Federal funding disbursed by the Department of Health and Human Services is expended in full compliance with EMTALA and section 504 of the Rehab Act, as interpreted consistent with the Born-Alive Infants Protection Act, as reflected in the policy set forth in section 2 of this order.
(i) The Secretary shall, as appropriate and to the fullest extent permitted by law, investigate complaints of violations of applicable Federal laws with respect to infants born alive, including infants who have an emergency medical condition in need of stabilizing treatment or infants with disabilities whose parents seek medical treatment for their infants. The Secretary shall also clarify, in an easily understandable format, the process by which parents and hospital staff may submit such complaints for investigation under applicable Federal laws.
(ii) The Secretary shall take all appropriate enforcement action against individuals and organizations found through investigation to have violated applicable Federal laws, up to and including terminating Federal funding for non-compliant programs and activities.
(c) The Secretary shall, as appropriate and consistent with applicable law, prioritize the allocation of Department of Health and Human Services discretionary grant funding and National Institutes of Health research dollars for programs and activities conducting research to develop treatments that may improve survival—especially survival without impairment—of infants born alive, including premature infants or infants with disabilities, who have an emergency medical condition in need of stabilizing treatment.
(d) The Secretary shall, as appropriate and consistent with applicable law, prioritize the allocation of Department of Health and Human Services discretionary grant funding to programs and activities, including hospitals, that provide training to medical personnel regarding the provision of life-saving medical treatment to all infants born alive, including premature infants or infants with disabilities, who have an emergency medical condition in need of stabilizing treatment.
(e) The Secretary shall, as necessary and consistent with applicable law, issue such regulations or guidance as may be necessary to implement this order.
[378] Webpage: “Parental Involvement in Minors’ Abortions.” Guttmacher Institute. Accessed September 16, 2023 at <www.guttmacher.org>
As of September 1, 2023 …
Parental Involvement in Minors’ Abortions … Consent only … Notification and consent …
|
Alabama |
Massachusetts‡ |
Pennsylvania |
|
Arizona* |
Michigan |
Rhode Island |
|
Arkansas* |
Mississippi |
South Carolina† ‡ |
|
Florida |
Missouriϴ |
Tennessee |
|
Idaho |
Nebraska* |
Texas* |
|
Indiana* |
North Carolina |
Utah |
|
Kansas* |
North Dakota |
Virginia* |
|
Kentucky |
Ohio |
Wisconsin† |
|
Louisiana* |
Oklahoma* |
Wyoming |
* Parental consent documentation must be notarized, which requires the parent to provide government-issued identification. In Louisiana and Oklahoma, the parent must also provide identification to the abortion provider.
† Allows specified health professionals to waive parental involvement in limited circumstances.
‡ … In Massachusetts, applies to patients younger than 16; in South Carolina, applies to those younger than 17.
ϴ Missouri law requires the consenting parent or guardian to notify any other custodial parent or guardian that the minor is having an abortion.
[379] Webpage: “Parental Involvement in Minors’ Abortions.” Guttmacher Institute. Accessed September 16, 2023 at <www.guttmacher.org>
As of September 1, 2023 …
Parental Involvement in Minors’ Abortions … Consent only …
|
California # |
New Mexico # |
|
Montana § |
# Permanently enjoined by court order; policy not in effect.
§ Temporarily enjoined by court order; policy not in effect.
[380] Webpage: “Parental Involvement in Minors’ Abortions.” Guttmacher Institute. Accessed September 16, 2023 at <www.guttmacher.org>
As of September 1, 2023 …
Parental Involvement in Minors’ Abortions … Notification only …
|
Colorado |
Montana‡ |
|
Delaware† ‡ |
New Hampshire |
|
Georgia |
South Dakota |
|
Iowa |
West Virginia |
|
Maryland† |
† Allows specified health professionals to waive parental involvement in limited circumstances.
‡ In Delaware … and Montana, applies to patients younger than 16….
[381] Webpage: “Parental Involvement in Minors’ Abortions.” Guttmacher Institute. Accessed September 16, 2023 at <www.guttmacher.org>
As of September 1, 2023 …
Parental Involvement in Minors’ Abortions … Notification only …
|
Alaska # |
New Jersey # |
|
Nevada # |
# Permanently enjoined by court order; policy not in effect.
[382] Webpage: “Parental Involvement in Minors’ Abortions.” Guttmacher Institute. Accessed September 16, 2023 at <www.guttmacher.org>
As of September 1, 2023 …
Parental Involvement in Minors’ Abortions … State …
NOTE: The following states are not listed among those with parental involvement laws:
|
Connecticut |
Maine |
Oregon |
|
Hawaii |
Minnesota |
Vermont |
|
Illinois |
New York |
Washington |
[383] NOTE: The sum of states above totals 51 due to Montana having both a temporarily enjoined consent law and a notification law (in effect.)
Webpage: “Parental Involvement in Minors’ Abortions.” Guttmacher Institute. Accessed September 16, 2023 at <www.guttmacher.org>
“As of September 1, 2023 … Parental Involvement in Minors’ Abortions … Consent only … Montana § … § Temporarily enjoined by court order; policy not in effect. … Notification only … Montana‡ … ‡ … applies to patients younger than 16”
[384] Revised Code of Washington, Title 26, Chapter 28, Section 085: “Applying Tattoo to a Minor—Penalty.” Accessed October 23, 2023 at <apps.leg.wa.gov>
Every person who applies a tattoo to any minor under the age of eighteen is guilty of a misdemeanor. It is not a defense to a violation of this section that the person applying the tattoo did not know the minor’s age unless the person applying the tattoo establishes by a preponderance of the evidence that he or she made a reasonable, bona fide attempt to ascertain the true age of the minor by requiring production of a driver’s license or other picture identification card or paper and did not rely solely on the oral allegations or apparent age of the minor.
[385] California Code Division 8, Chapter 23, Section 22706: “Special Business Regulations, Tanning Facilities.” Accessed October 23, 2023 at <law.justia.com>
(b) … (3) Persons under 18 years of age are prohibited from using an ultraviolet tanning device.
(4) Proof of age shall be satisfied with a driver’s license or other government issued identification containing the date of birth and a photograph of the individual.
(Amended by Stats. 2011, Ch. 664, Sec. 2. (SB 746) Effective January 1, 2012.)
[386] New Jersey Statute 2C:40-21: “Tattooing of a Minor; Parental Permission, Required.” New Jersey Code of Criminal Justice. Accessed October 23, 2023 at <law.justia.com>
“A person commits a disorderly persons offense if he knowingly tattoos or engages in body piercing of a minor under the age of 18 years without first having obtained the written permission of the minor’s parent or legal guardian or, if neither exists, a person who stands in place of a parent.”
[387] Connecticut General Statutes, Title 19a, Chapter 368a, Section 19a–92g: “Public Health and Well-Being, Body Piercing.” Accessed October 23, 2023 at <law.justia.com>
(a) No person may perform body piercing on an unemancipated minor under eighteen years of age without the written permission of the minor’s parent. For purposes of this subsection, “body piercing” means piercing or creating a channel through any part of the body other than the ear lobe for the purpose of inserting a decorative object, and “ear lobe” means the lower portion of the auricle having no cartilage.
[388] Webpage: “Parental Involvement in Minors’ Abortions.” Guttmacher Institute. Accessed October 23, 2023 at <www.guttmacher.org>
NOTE: As of September 1, 2023, there are no notification or consent laws in effect for Washington, California, New Jersey, or Connecticut.
[389] Ruling: Hodgson v. Minnesota. U.S. Supreme Court, June 25, 1990. <caselaw.findlaw.com>
Subdivision 2 of Minn. Stat. 144.343 provides that no abortion shall be performed on a woman under 18 years of age until at least 48 hours after both of her parents have been notified. The two-parent notice requirement is mandatory unless, inter alia, the woman declares that she is a victim of parental abuse or neglect, in which event notice of her declaration must be given to the proper authorities.
[390] Brief submitted to the U.S. Supreme Court: Hodgson v. Minnesota. American Psychological Association, September 1, 1989. <www.apa.org>
Page 18: “Psychological theory and research about cognitive, social and moral development strongly supports the conclusion that most adolescents are competent to make informed decisions about important life situations.”
[391] Brief submitted to the U.S. Supreme Court: Hodgson v. Minnesota. American Psychological Association, September 1, 1989. <www.apa.org>
Pages 19–20:
In fact, by middle adolescence (age 14–15) young people develop abilities similar to adults in reasoning about moral dilemmas,46 understanding social rules and laws,47 reasoning about interpersonal relationships48 and interpersonal problems,40 and reasoning about custody preference during divorce.50 … Thus, by age 14 most adolescents have developed adult-like intellectual and social capacities including specific abilities outlined in the law as necessary for understanding treatment alternatives, considering risks and benefits, and giving legally competent consent.
[392] Brief submitted to the U.S. Supreme Court: Hodgson v. Minnesota. American Psychological Association, March 16, 1987. <www.apa.org>
Page 10: “In sum, the unvarying and highly significant findings of numerous scientific studies indicate that with respect to the capacity to understand and reason logically, there is no qualitative or quantitative difference between minors in mid-adolescence, i.e., about 14–15 years of age, and adults.”
[393] Ruling: Roper v. Simmons. U.S. Supreme Court, March 1, 2005. <caselaw.findlaw.com>
At age 17, respondent Simmons planned and committed a capital murder. After he had turned 18, he was sentenced to death. His direct appeal and subsequent petitions for state and federal postconviction relief were rejected. … This Court then held, in Atkins v. Virginia, 536 U.S. 304, that the Eighth Amendment, applicable to the States through the Fourteenth Amendment, prohibits the execution of a mentally retarded person. Simmons filed a new petition for state postconviction relief, arguing that Atkins’ reasoning established that the Constitution prohibits the execution of a juvenile who was under 18 when he committed his crime.
[394] Brief submitted to the U.S. Supreme Court: Roper v. Simmons. American Psychological Association, July 19, 2004. <www.apa.org>
Pages 7–8:
Adolescent Decision-Makers on Average Are Less Future-Oriented and Less Likely to Consider Properly the Consequences of Their Actions.
In comparison with adults, studies show that adolescents are less likely to consider alternative courses of action, understand the perspective of others, or restrain impulses. In a study of more than 1,000 adolescents and adults, researchers investigated the relationships among the factors of age, maturity, and antisocial decisionmaking. Elizabeth Cauffman & Laurence Steinberg, “(Im)maturity and Judgment in Adolescence: Why Adolescents May be Less Culpable Than Adults,” 18 Behav. Sci. & L. 741 (2000). Adolescents, on average, were “less responsible, more myopic, and less temperate than the average adult.” Id. at 757. In this study, the most dramatic change in behavior occurred sometime between 16 and 19 years of age, especially with respect to “perspective” (i.e., the consideration of different viewpoints and broader contexts of decisions), and “temperance” (i.e., the ability to limit impulsivity and evaluate situations before acting). Id. at 756. And it was not until age 19 that this development of responsible decisionmaking plateaued. Ibid. These findings indicate “that once the developmental changes of adolescence are complete, maturity of judgment may stabilize.” Ibid.
In another analysis of decision-making competence, adolescents performed more poorly than adults. Bonnie L. Halpern-Felsher & Elizabeth Cauffman, “Costs and Benefits of a Decision: Decision-Making Competence in Adolescents and Adults,” 22 J. Applied Developmental Psycholog. 257, 268 (2001). Although even greater differences prevailed between younger adolescents and adults, the researchers concluded “it is clear that important progress in the development of decision-making competence occurs sometime during late adolescence.” Id. at 271. The researchers explained that “these changes have a profound effect on their ability to make consistently mature decisions.” Ibid. Adults, for example, were better able to weigh the options available to resolve an issue. Id. at 268; see also Lita Furby & Ruth Beyth-Marom, “Risk Taking in Adolescence: A Decision-Making Perspective,” 12 Developmental Rev. 1, 1 (1992) (highlighting how adolescents seek different outcomes than adults from decision-making).
[395] Webpage: “Abortion.” Gallup, February 17, 2012. <bit.ly>
A law requiring women under 18 to get parental consent for any abortion
|
Favor (%) |
Oppose (%) |
No opinion (%) |
|
|
2011 Jul 15–17 |
71 |
27 |
2 |
|
2005 Nov 11–13 |
69 |
28 |
3 |
|
2003 Jan 10–12 |
73 |
24 |
3 |
|
1996 Jul 25–28 |
74 |
23 |
3 |
|
1992 Jan 16–19 |
70 |
23 |
7 |
[396] Webpage: “Abortion and Birth Control (Page 2).” Polling Report. Accessed February 24, 2017 at <www.pollingreport.com>
CBS News Poll. July 13–14, 2005. N=632 adults nationwide. …
“Would you favor or oppose requiring that at least one parent be told before a girl under 18 years of age could have an abortion?”
Favor [=] 80% … Oppose [=] 17% … Unsure [=] 3%
[397] Webpage: “Abortion and Birth Control (Page 2).” Polling Report. Accessed February 24, 2017 at <www.pollingreport.com>
Pew Research Center survey. Aug. 11–17, 2009. N=2,010 adults nationwide …
“Do you strongly favor, favor, oppose, or strongly oppose requiring that women under the age of 18 get the consent of at least one parent before they are allowed to have an abortion?”
Strongly Favor [=] 45% … Favor [=] 31% … Oppose [=] 11% … Strongly Oppose [=] 8% … Unsure [=] 5%
[398] “2020 Democratic Party Platform.” Democratic National Committee, August 17, 2020. <www.presidency.ucsb.edu>
[399] “Resolution Regarding the Republican Party Platform.” Republican National Committee, August 24, 2020. <www.presidency.ucsb.edu>
WHEREAS, The Republican National Committee (RNC) has significantly scaled back the size and scope of the 2020 Republican National Convention in Charlotte due to strict restrictions on gatherings and meetings, and out of concern for the safety of convention attendees and our hosts. …
RESOLVED, That the 2020 Republican National Convention will adjourn without adopting a new platform until the 2024 Republican National Convention.
[400] “2016 Republican Platform.” Republican National Convention, July 2016. <www.presidency.ucsb.edu>
We salute the many states that now protect women and girls through laws requiring informed consent, parental consent, waiting periods, and clinic regulation. …
… We support the right of parents to consent to medical treatment for their minor children and urge enactment of legislation that would require parental consent for their daughter to be transported across state lines for abortion.
[401] Report: “Sexual Assault of Young Children as Reported to Law Enforcement: Victim, Incident, and Offender Characteristics.” By Howard N. Snyder. Bureau of Justice Statistics, U.S. Department of Justice, July 2000. <www.bjs.gov>
Page 1: “The 1991 through 1996 NIBRS [National Incident-Based Reporting System] master files contain reports from law enforcement agencies in 12 States: Alabama, Colorado, Idaho, Illinois, Iowa, Massachusetts, Michigan, North Dakota, South Carolina, Utah, Vermont, and Virginia. These reports were scanned to identify incidents of sexual assault.”
Page 3: “Age profiles of sexual assault victims, by offense category: Forcible rape.”
Page 13:
Forcible rape (except “statutory rape”) The carnal knowledge of a person, forcibly and/or against that person’s will; or not forcibly or against the person’s will where the victim is incapable of giving consent because of his/her temporary or permanent mental or physical incapacity. If force was used or threatened, the crime should be classified as forcible rape regardless of the age of the victim. If no force was used or threatened and the victim was under the statutory age of consent, the crime should be classified as statutory rape.
[402] Dataset: “Figure 2. Age Profiles of Sexual Assault Victims, by Offense Category.” Bureau of Justice Statistics, U.S. Department of Justice, July 2000. <www.bjs.gov>
NOTE: An Excel file containing the data is available upon request.
[403] Book: Sex and America’s Teenagers. By Patricia Donovan and others. Alan Guttmacher Institute, 1994.
Page 28:
Forced Sex …
Some 74% of women who had intercourse before age 14 and 60% of those who had sex before age 15 report having had sex involuntarily. …
Those who answered affirmatively to the question “Was there ever a time when you were forced to have sex against your will, or were raped?” were classified as having had involuntary intercourse. …
|
Age at First Intercourse |
Involuntary Only |
Both Voluntary and Involuntary |
Voluntary Only |
|
13 and younger |
61% |
13% |
26% |
|
14 and younger |
43% |
17% |
40% |
|
15 and younger |
26% |
14% |
60% |
|
16 and younger |
10% |
14% |
76% |
|
17 and younger |
5% |
13% |
82% |
|
18 and younger |
3% |
12% |
85% |
|
19 and younger |
1% |
14% |
85% |
Adapted by AGI [Alan Guttmacher Institute] from tabulations by K. A. Moore, C. W. Nord, and J. A. Peterson of data from the 1987 National Survey of Children. See K. A. Moore, C. W. Nord, and J. A. Peterson, : “Nonvoluntary Sexual Activity Among Adolescents,” Family Planning Perspectives, 21: 110–114, 1989, Table 2, p. 111.
CALCULATIONS:
[404] Paper: “Nonvoluntary Sexual Activity Among Adolescents.” By Kristin Anderson Moore, Christine Winquist Nord, and James L. Peterson. Family Planning Perspectives, May–June, 1989. Pages 110–114. <www.jstor.org>
Pages 110–111:
Data from the 1987 round of the National Survey of Children [NSC] indicate that seven percent of Americans aged 18–22 have experienced at least one episode of nonvoluntary sexual intercourse. Women were more likely than men to report having had such an experience, with just under half of all nonvoluntary experiences among women occurring before age 14. …
In this article, we use nationally representative data to estimate the proportion of Americans who experience nonvoluntary intercourse during childhood and adolescence, according to race and gender.
The analyses in this article are based on data from the third wave of interviews, which were conducted by telephone in 1987. These interviews sought to follow up on experiences documented in the first two waves of the survey and collected data on early sexual and fertility behavior, educational progress, employment and welfare experience, and psychological wellbeing.1 The vast majority of respondents were aged 18–22; 30 respondents were 17, and 47 had turned 23. The response rate was 82 percent of the second wave sample.
Accumulated attrition from the NSC over the three waves has been considerable and, as in most longitudinal surveys, it has been greatest among youths from disadvantaged backgrounds. Although the data presented here are weighted to correct for the initial oversampling of blacks, for the subsampling by family type in the second wave of interviews, and for differing rates of sample attrition, the possibility exists that our analyses underestimate the true incidence of nonvoluntary sex among children and adolescents. Among respondents, nonresponse to individual items used in the analyses was virtually nil, and therefore cannot be considered a source of bias. …
Nonvoluntary Sexual Activity
Overall, seven percent of all respondents interviewed in the 1987 NSC responded affirmatively to the question: “Was there ever a time when you were forced to have sex against your will, or were raped?” Because of the sensitive nature of this question, it is likely that respondent reports underestimate the true incidence of non-voluntary sex. However, some respondents may also have redefined their voluntary sexual experiences with hindsight and reported them as having been non-voluntary. With the exception of one white female, all respondents who reported having experienced nonvoluntary intercourse also reported having had sex voluntarily. Hence, we consider overreporting of non-voluntary intercourse to be unlikely and believe this estimate to be a lower limit.
Table 2. Cumulative proportions of young people who had experienced intercourse prior to given ages, by gender and race. according to life-table estimates based on three surveys
Page 112:
Clearly, among both black and white women at younger ages, the proportions who had experienced intercourse are considerably higher when nonvoluntary sex is included in the estimate. Seven percent of white women reported having experienced intercourse by their 14th birthday, but only two percent reported having had a voluntary sexual experience by that age.
[405] For facts about what constitutes a scientific survey and the factors that impact their accuracy, visit Just Facts’ research on Deconstructing Polls & Surveys.
[406] Paper: “Extent, Nature, and Consequences of Rape Victimization: Findings From the National Violence Against Women Survey.” By Patricia Tjaden and Nancy Thoennes. U.S. Department of Justice, June 2006. <www.ncjrs.gov>
Page 1:
Rape is a significant social and health problem in the United States. Results from the National Violence Against Women Survey (NVAWS) revealed that 17.7 million women and 2.8 million men in the United States were forcibly raped at some time in their lives, with 302,091 women and 92,748 men forcibly raped in the year preceding the survey.
Page 3:
In the National Violence Against Women Survey (NVAWS), rape was defined as an event that occurred without the victim’s consent that involved the use or threat of force in vaginal, anal, or oral intercourse. This definition closely resembles that used in the National Women’s Study (NWS).a However, unlike NWS, NVAWS includes both attempted and completed rape. Thus, unless otherwise noted in this report, “rape” refers to both attempted and completed rape.
Pages 5–6:
Survey Methodology
The National Violence Against Women Survey (NVAWS) was conducted from November 1995 to May 1996 by interviewers at Schulman, Ronca, Bucuvalas, Inc. (SRBI) under the direction of John Boyle.a The authors of this Special Report designed the survey questionnaire and conducted the analysis.b
The sample was drawn by random-digit dialing of households with a telephone in the 50 States and the District of Columbia. The sample was administered by U.S. Census region. Within each region, a simple random sample of working residential “hundreds banks” of phone numbers was drawn. (A hundreds bank is the first 8 digits of any 10-digit telephone number.) A randomly generated 2-digit number was appended to each randomly sampled hundreds bank to produce the full 10-digit, random-digit number. Separate banks of numbers were generated for male and female respondents. These random-digit numbers were called by SRBI interviewers from their central telephone facility, where nonworking and nonresidential numbers were screened out. When a residential household was reached, eligible adults were identified. In households with more than one eligible adult, the adult with the most recent birthday was selected as the designated respondent.
A total of 8,000 women and 8,005 men age 18 and older were interviewed using a computer assisted telephone interviewing (CATI) system. (Five completed interviews with men were subsequently eliminated from the sample during data editing because of an excessive amount of inconsistent and missing data.) Only female interviewers surveyed female respondents. To test for possible bias introduced by the gender of the interviewer, a split-sample approach was used in the male sample whereby half of the interviews were conducted by female interviewers and half by male interviewers. A Spanish-language translation was administered by bilingual interviewers to Spanish-speaking respondents. …
Moreover, because this version includes separate questions about attempted rape and completed rape, the survey records can be used to ascertain separate victimization rates for attempted rape and completed rape. …
To determine the representativeness of the sample, select demographic characteristics of the NVAWS sample were compared with demographic characteristics of the general population from the U.S. Census Bureau’s 1995 Current Population Survey of adult men and women.d
Page 18:
Survey results show that rape occurs at an early age for many rape victims—21.6 percent of women and 48 percent of men were younger than 12 years old when they were first raped, and 32.4 percent of women and 23 percent of men were between ages 12 and 17. Thus, more than half (54 percent) of female victims and nearly three-quarters (71 percent) of male victims were first raped before their 18th birthday. In comparison, 29.4 percent of female victims and 16.6 percent of male victims were 18 to 24 years old when they were first raped, and 16.6 percent of female victims and 12.3 percent of male victims were age 25 or older (see exhibit 10). These findings are consistent with findings from the National Women’s Study, which shows that many U.S. women are raped as children and adolescents.19
Page 39:
2 For example, rape victimization estimates generated from the Bureau of Justice Statistics’ National Crime Victimization Survey are substantially lower than rape victimization estimates generated from the National Women’s Study (see National Victim Center and Crime Victims Research and Treatment Center, Rape in America: A Report to the Nation, Arlington, VA: National Victim Center and Charleston, SC: Crime Victims Research and Treatment Center, 1992).]
19 The National Women’s Study (see note 2) found that 29 percent of all forcible rapes of females occurred when the victim was younger than 11 years old, and another 32 percent occurred when the victim was between ages 11 and 17.
[407] For facts about what constitutes a scientific survey and the factors that impact their accuracy, visit Just Facts’ research on Deconstructing Polls & Surveys.
[408] Report: “Prevalence and Characteristics of Sexual Violence, Stalking, and Intimate Partner Violence Victimization—National Intimate Partner and Sexual Violence Survey, United States, 2011.” By Matthew J. Breiding and others. U.S. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention, September 5, 2014. <www.cdc.gov>
Page 1:
NISVS [National Intimate Partner and Sexual Violence Survey] is a national random-digit–dial telephone survey of the noninstitutionalized English- and Spanish-speaking U.S. population aged ≥18 years. NISVS gathers data on experiences of sexual violence, stalking, and intimate partner violence among adult women and men in the United States by using a dual-frame sampling strategy that includes both landline and cellular telephones. The survey was conducted in 50 states and the District of Columbia; in 2011, the second year of NISVS data collection, 12,727 interviews were completed, and 1,428 interviews were partially completed.
Pages 11–12:
Among female victims of completed rape (completed forced penetration and completed alcohol- or drug-facilitated penetration), this form of sexual violence was first experienced by an estimated 78.7% before age 25 years, by an estimated 40.4% before age 18 years (28.3% at ages 11–17 years and 12.1% at age ≤10 years), and by an estimated 38.3% at age 18–24 years (Figure 3).
Page 17:
The findings of this report are subject to at least five limitations. First, the overall response rate for the 2011 NISVS survey was relatively low (33.1%). However, the cooperation rate was high (83.5%), and multiple efforts were made to reduce the likelihood of nonresponse and noncoverage bias. These included a nonresponse follow-up in which randomly selected nonresponders were contacted again and offered an increased incentive for participation as well as the inclusion of a cellular telephone sample. Second, although NISVS captures a broad range of self-reported victimization experiences, it is likely that the estimates presented underestimate the prevalence of sexual violence, stalking, and intimate partner violence.18 Victims who are involved in violent relationships or who have recently experienced severe forms of violence might be less likely to participate in surveys or might not be willing to disclose their experiences because of unresolved emotional trauma or concern for their safety, among other reasons. Third, a telephone survey might be less likely to capture some populations that could be at higher risk for victimization (e.g., persons living in nursing homes, military bases, prisons, or shelters, or those who are homeless). Fourth, self-reported data are vulnerable to recall bias because respondents might believe that events occurred closer in time than they did in actuality (i.e., telescoping), and this type of bias might particularly affect 12-month prevalence estimates. Finally, follow-up questions were designed to reflect the victim’s experience with each perpetrator across the victim’s lifetime and there were limitations associated with how these questions were asked. Respondents were asked about the impact from any of the violence inflicted by each perpetrator. Therefore, the impact of specific intimate partner violence behaviors cannot be assessed. Also, because victims’ reports of the age and relationship at the time any violence began with each perpetrator were used, it was not always possible to assess the age or relationship at the time specific types of intimate partner violence occurred.
[409] For facts about what constitutes a scientific survey and the factors that impact their accuracy, visit Just Facts’ research on Deconstructing Polls & Surveys.
[410] Act 537: “An Act to Require Parental Consent Before Performing an Abortion on a Minor; and for Other Purposes.” State of Arkansas, 85th General Assembly (2005). Signed into law by Mike Huckabee on March 4, 2005. <www.arkleg.state.ar.us>
Except as otherwise provided in §§ 20-16-804 and 20-16-805, no person may perform an abortion upon an unemancipated minor, or upon a woman for whom a guardian or custodian has been appointed because of a finding of incompetency, unless the person or the person’s agent first obtains the written consent of either parent or the legal guardian or custodian. …
“Parent” shall mean both parents either parent of the pregnant woman if they are both living; one (1) parent of the pregnant woman if only one (1) is living or if the second one (1) cannot be located through reasonably diligent effort; or the court-appointed guardian or custodian if the pregnant woman has one.
[411] Act 934: “An Act to Establish the Parental Involvement Enhancement Act; to Repeal the Parental Notification Provisions; and for Other Purposes.” State of Arkansas, 90th General Assembly (2015). Signed into law by Asa Hutchinson on April 4, 2015. <www.arkleg.state.ar.us>
“Consent” means: (A) In the case of a pregnant woman who is less than eighteen (18) years of age, a notarized written statement signed by the pregnant woman and her mother, father, or legal guardian declaring that the pregnant woman intends to seek an abortion and that her mother, father, or legal guardian consents to the abortion. …
“Parent” means: (A) Either parent of the pregnant woman if both parents are living; (B) One (1) parent of the pregnant woman if only one (1) is living or if the second parent cannot be located through reasonably diligent effort; or (C) The court-appointed guardian or custodian if the pregnant woman has one.
[412] Arkansas State Code, Title 20, Subtitle 2, Chapter 16, Subchapter 8: “Abortion – Parental Involvement Enhancement Act.” Arkansas General Assembly. Accessed July 23, 2021 at <law.justia.com>
Section 805: “Manner of Consent”
(a) A physician shall not perform an abortion upon a pregnant woman unless:
(1) In the case of a woman who is less than eighteen (18) years of age, he or she obtains the notarized written consent of both the pregnant woman and one (1) of her parents or her legal guardian; or
(2) In the case of woman who is an incompetent person, the physician first obtains the notarized written consent of her legal guardian.
(b) The notarized written consent shall include without limitation the following information:
(1) The name and birthdate of the minor or incompetent woman;
(2) The name of the parent or legal guardian;
(3) A statement from the parent or legal guardian that he or she is aware that the minor or incompetent woman desires an abortion and that he or she does consent to the abortion; and
(4) The date.
Section 803: “Definitions”
(7) “Minor” means an individual under eighteen (18) years of age;
(8) “Parent” means:
(A) Either parent of the pregnant woman if both parents are living;
(B) One (1) parent of the pregnant woman if only one (1) is living or if the second parent cannot be located through reasonably diligent effort; or
(C) The court-appointed guardian or custodian if the pregnant woman has one….
[413] Article: “Granite City Abortion Clinic Part of Rape Investigation.” By Cordell Whitlock. Channel 5, KDSK, St. Louis, November 16, 2006. <www.ksdk.com>
Police in Arkansas say a Granite City [IL] abortion clinic is part of a rape investigation involving a juvenile. Jeffery Cheshier, 41, is accused of raping a 15-year-old girl. Officers say he then forced the victim to have an abortion in Granite City.
Police in Bryant, Ark., say Cheshier began assaulting the juvenile last year. In October, he was arrested and charged with rape. The victim told police Cheshier had gotten her pregnant and forced her to have an abortion.
[414] Article: “Protesters’ Photos May Be Clue in Rape Case.” By Shane Graber. St. Louis Post-Dispatch, November 17, 2006. <www.stltoday.com>
“The teen told police he got her pregnant and took her to a St. Louis-area abortion clinic in March, the affidavit said.”
[415] Article: “Federal Judge Rejects Request to Enforce Illinois Abortion Law.” Associated Press, March 2, 2008.
“The Parental Notice of Abortion Act was passed in 1984 and updated in 1995 but never enforced because the Illinois Supreme Court refused to issue rules spelling out how judges should handle appeals of the notification requirement.”
[416] Brief: “Parental Involvement in Minors’ Abortions.” Guttmacher Institute, June 1, 2008. <www.guttmacher.org>
“Illinois … Enforcement permanently or temporarily enjoined by a court order; policy not in effect.”
[417] Article: “Granite City Abortion Clinic Part of Rape Investigation.” By Cordell Whitlock. Channel 5, KDSK, St. Louis, November 16, 2006. <www.ksdk.com>
“Angela Michael frequently protests outside the clinic and police used a photo she took of Cheshier’s car to prove he was there in March.”
[418] Phone call from Just Facts to the arresting officer of Jeffrey Cheshier, June 12, 2008.
The officer stated that:
• Cheshier committed suicide.
• Cheshier was the alleged victim’s stepfather.
• The girl kept detailed records on her calendar, and as such, Cheshier was facing about 12 counts of rape.
[419] Death Certificate:
Jeffery Cheshier
Birth Date: 14 Oct 1965
Death Date: 17 Jul 2007
Social Security Number: XXX-XX-XXXX
State or Territory Where Number Was Issued: Arkansas
[420] House of Representatives Amendment to Senate Bill 403: “Child Interstate Abortion Notification Act.” 109th Congress (2005–2006), September 26, 2006. <www.congress.gov>
Sec. 2431. Transportation of Minors in Circumvention of Certain Laws Relating to Abortion
(a) Offense—
(1) Generally—Except as provided in subsection (b), whoever knowingly transports a minor across a State line, with the intent that such minor obtain an abortion, and thereby in fact abridges the right of a parent under a law requiring parental involvement in a minor’s abortion decision, in force in the State where the minor resides, shall be fined under this title or imprisoned not more than one year, or both.
(b) Exceptions—
(1) The prohibition of subsection (a) does not apply if the abortion was necessary to save the life of the minor because her life was endangered by a physical disorder, physical injury, or physical illness, including a life endangering physical condition caused by or arising from the pregnancy itself.
(2) A minor transported in violation of this section, and any parent of that minor, may not be prosecuted or sued for a violation of this section, a conspiracy to violate this section, or an offense under section 2 or 3 based on a violation of this section. …
Sec. 2435. Child Interstate Abortion Notification
(a) Offense—
(1) Generally—A physician who knowingly performs or induces an abortion on a minor in violation of the requirements of this section shall be fined under this title or imprisoned not more than one year, or both.
(2) Parental Notification—A physician who performs or induces an abortion on a minor who is a resident of a State other than the State in which the abortion is performed must provide, or cause his or her agent to provide, at least 24 hours actual notice to a parent of the minor before performing the abortion. If actual notice to such parent is not possible after a reasonable effort has been made, 24 hours constructive notice must be given to a parent.
(b) Exceptions—The notification requirement of subsection (a)(2) does not apply if
(1) the abortion is performed or induced in a State that has, in force, a law requiring parental involvement in a minor’s abortion decision and the physician complies with the requirements of that law;
(2) the physician is presented with documentation showing with a reasonable degree of certainty that a court in the minor’s State of residence has waived any parental notification required by the laws of that State, or has otherwise authorized that the minor be allowed to procure an abortion;
(3) the minor declares in a signed written statement that she is the victim of sexual abuse, neglect, or physical abuse by a parent, and, before an abortion is performed on the minor, the physician notifies the authorities specified to receive reports of child abuse or neglect by the law of the State in which the minor resides of the known or suspected abuse or neglect;
(4) the abortion is necessary to save the life of the minor because her life was endangered by a physical disorder, physical injury, or physical illness, including a life endangering physical condition caused by or arising from the pregnancy itself, or because in the reasonable medical judgment of the minor’s attending physician, the delay in performing an abortion occasioned by fulfilling the prior notification requirement of subsection (a)(2) would cause a substantial and irreversible impairment of a major bodily function of the minor arising from continued pregnancy, not including psychological or emotional conditions, but an exception under this paragraph does not apply unless the attending physician or an agent of such physician, within 24 hours after completion of the abortion, notifies a parent in writing that an abortion was performed on the minor and of the circumstances that warranted invocation of this paragraph; or
(5) the minor is physically accompanied by a person who presents the physician or his agent with documentation showing with a reasonable degree of certainty that he or she is in fact the parent of that minor.
[421] Calculated with data from vote 479: “Child Custody Protection Act.” U.S. House of Representatives, September 26, 2006. <clerk.house.gov>
|
Party |
Voted “Yes” |
Voted “No” |
Voted “Present” or Did Not Vote† |
|||
|
Number |
Portion |
Number |
Portion |
Number |
Portion |
|
|
Republican |
215 |
93% |
9 |
4% |
6 |
3% |
|
Democrat |
49 |
24% |
143 |
71% |
9 |
4% |
|
Independent |
0 |
0% |
1 |
100% |
0 |
0% |
|
NOTE: †Voting “Present” is effectively the same as not voting. |
||||||
[422] Calculated with data from vote 263: “Motion to Invoke Cloture on the Motion to Concur in House Amendment to S.403.” U.S. Senate, September 29, 2006. <www.senate.gov>
|
Party |
Voted “Yes” |
Voted “No” |
Voted “Present” or Did Not Vote† |
|||
|
Number |
Portion |
Number |
Portion |
Number |
Portion |
|
|
Republican |
51 |
93% |
4 |
7% |
0 |
0% |
|
Democrat |
6 |
14% |
37 |
84% |
1 |
2% |
|
Independent |
0 |
0% |
1 |
100% |
0 |
0% |
|
NOTE: †Voting “Present” is effectively the same as not voting. |
||||||
“Alphabetical by Senator Name … Biden (D-DE), Nay … Clinton (D-NY), Nay … Collins (R-ME), Nay … Menendez (D-NJ), Nay … Obama (D-IL), Nay … Schumer (D-NY), Nay”
[423] Report: “Statutory Rape: A Guide to State Laws and Reporting Requirements.” By Asaph Glosser, Karen Gardiner & Mike Fishman. Prepared for the U.S. Department of Health and Human Services by the Lewin Group, December 15, 2004. <aspe.hhs.gov>
Page 5: “As the first column in Table 1 shows, the age of consent varies by state. In the majority of states (34), it is 16 years of age. In the remaining states, the age of consent is either 17 or 18 years old (6 and 11 states, respectively).”
Pages 6–7: “Table 1: State Age Requirements.”
[424] Report: “Statutory Rape: A Guide to State Laws and Reporting Requirements.” By Asaph Glosser, Karen Gardiner & Mike Fishman. Prepared for the U.S. Department of Health and Human Services by the Lewin Group, December 15, 2004. <aspe.hhs.gov>
Page 12: “Each state’s reporting requirements identify certain individuals who are required to notify the authorities of suspected abuse. Although it varies by state, mandated reporters are typically individuals who encounter children through their professional capacity.”
NOTES:
[425] Webpage: “About Us.” Life Dynamics. Accessed April 12, 2017 at <lifedynamics.com>
Our mission is simple: to end legalized abortion in America and restore legal protection to the unborn. Life Dynamics have always striven to be the most innovative and the cutting edge of the pro-life movement because, “We are not here to just put up a good fight, we are here to win—because winning is how this killing is going to stop.” We believe in being Pro-Life, without compromise, without exceptions, and without apology.
[426] Report: “Child Predators.” By Mark Crutcher. Life Dynamics, 2002. <www.childpredators.com>
With the information we now have, it is simply undeniable that Planned Parenthood and the National Abortion Federation have made a conscious decision to conceal the sexual exploitation of children and protect the men who commit these crimes.
We have uncovered an overwhelming body of statistical evidence showing that the rate at which these two organizations fail to comply with mandatory reporting laws is in excess of 90 percent. This data was obtained from government sources, medical journals, independent researchers and the abortion industry itself.26
To test this conclusion we conducted a covert survey in which we called over 800 Planned Parenthood and National Abortion Federation facilities across the country. Our caller portrayed a 13-year-old girl who was pregnant by her 22-year-old boyfriend. Her story was that she wanted an abortion because she and her boyfriend did not want her parents to find out about the sexual relationship. In every call the ages of the girl and her boyfriend were made perfectly clear. It was also made clear that the motivation for the abortion was to conceal this illicit sexual activity from the girl’s parents and the authorities. Additionally, our caller never said a single thing that might suggest that her parents would become abusive if they discovered her sexual activity.
[427] Article: “Pro-Life Group Launches Undercover Sting.” Fox News, May 31, 2002. Updated 1/13/15. <www.foxnews.com>
“What she learned is that more than 90 percent of the clinic employees handling the calls said they would conceal the information provided by the caller, according to Life Dynamics president Mark Crutcher.”
NOTE: Tapes were made of the phone calls and some have been circulated to the media, who confirmed their authenticity. See details of their authentication in the following footnotes.
[428] Report: “Child Predators.” By Mark Crutcher. Life Dynamics, 2002. <www.childpredators.com>
“Some employees of these organizations even coached our caller on how to avoid detection, how to circumvent parental involvement laws and what to say or not say when she came to the clinic. In a significant number of instances she was encouraged to lie about—or conceal—her age or her boyfriend’s age or to give false names.”
[429] Report: “Child Predators.” By Mark Crutcher. Life Dynamics, 2002. <www.childpredators.com>
“The results of this survey were appalling. Even though many of these clinic workers openly acknowledged to our caller that this situation was illegal and that they were required to report it to the state, the overwhelming majority readily agreed to conceal this illegal sexual activity.”
[430] Report: “Child Predators.” By Mark Crutcher. Life Dynamics, 2002. <www.childpredators.com>
In some calls she was given instructions on how to circumvent the parental involvement requirement altogether, even to the point of suggesting that she bring someone along to sign for her who looked old enough to impersonate one of her parents. In one particularly egregious case, the clinic worker lamented the fact that because our caller’s boyfriend was only 22 he wouldn’t look old enough to pass as her father. She went on to suggest that our caller look for an older person to help her out. When our caller said her boyfriend had a 50-year-old uncle who would do it, the employee said that would be okay as long as the uncle was instructed to not say anything while at the clinic to indicate he was not really her father. The employee stated that the uncle could even drop by, sign the papers, and leave before she actually came in for the abortion, and that the clinic’s notary public would notarize the uncle’s signature for the state’s required documentation—despite knowing that it was a fraudulent representation.
[431] Article: “Connecticut Abortion Clinics Look The Other Way.” By Ted Greenberg. WTIC–TV, May 22, 2002.
So what does Planned Parenthood have to say about all this? Not much. As we did with the child advocate, we wanted to play the tapes for them and get their reaction, but they refused unless they could hear them first. We agreed to play the tapes over the phone for them, but still they refused an on-camera interview.
Instead, they issued this short statement. “Planned Parenthood questions the reliability of staged tapes of supposed telephone conversations surreptitiously prepared by Life Dynamics, an organization with a notorious anti-Planned Parenthood agenda.”
[432] Article: “Connecticut Abortion Clinics Look The Other Way.” By Ted Greenberg. WTIC–TV, May 22, 2002.
We wanted to be sure of their authenticity, too. So we made some calls to Connecticut Planned Parenthood centers and we asked for the names we heard. Some were not overly common names, like Heidi and Glenda. We found they indeed worked there.
Also, the tones placing the calls on the tape match the Planned Parenthood phone numbers.
NOTE: This article contains transcripts of phone calls with Planned Parenthood offices in Bridgeport, Norwich, New London, Willimantic, and West Hartford. For one example:
Caller: “I’m going to be 14 later on this month…. My boyfriend is 22.”
Willimantic Planned Parenthood: “I’m not going to—I’m going to pretend I didn’t hear that, okay?”
Caller: “Okay.”
Planned Parenthood: “Don’t even bring that up, okay.”
Caller: “Even if he’s taking me there?”
Planned Parenthood: “No, no, don’t even go there, don’t even bring it up.”
[433] Article: “In Debate on Abortion, 2 Girls Make It Real.” By Tamar Lewin. New York Times, October 27, 1991. <www.nytimes.com>
“They have appeared on ‘60 Minutes,’ walking through their daughter’s graveyard and talking about how they blame the law for their daughter’s death.”
[434] Book: Choices: Women Speak Out About Abortion. Edited by Karen A Schneider. NARAL Foundation, 1997.
Chapter: “Becky Bell.” By Karen Bell (Becky’s mother). Pages 24–27.
Page 26: “One day, we got a letter from Peter Jennings. He wanted us to be on the news to talk about Becky, who was the first teenager known to die because of a parental consent law.”
[435] Webpage: “Peter Jennings.” ABC News. Accessed June 13, 2019 at <abcnews.go.com>
“Peter Jennings was the anchor and senior editor of ABC’s “World News Tonight,” where he established a reputation for independence and excellence in broadcast journalism. He was the network’s principal anchor for breaking news, election coverage and special events.”
[436] Article: “Teen-Agers Face Reality On Both Sides of Screen.” By John J. O’Connor. New York Times, October 13, 1992. <www.nytimes.com>
… Home Box Office has been noticeably more vigorous lately in its pursuit of original programming. …
… A good case in point is this evening’s abortion essay: “Public Law 106: The Becky Bell Story.”
… Becky ends up having an illegal abortion and dying of a resultant infection. The story begins with her being rushed to the hospital by her distraught, helpless parents.
[437] Transcript: Larry King Live. Hosted by Larry King. CNN, December 24, 1990.
[Cybill Shepherd:] Abortion will continue, whether it’s legal or not. It’s not the question of whether abortion will be around, it’s just a question of whether you’re going to have women—women are already dying of illegal abortions. Becky Bell in Indiana couldn’t go to her parents, there was a parental consent law. She had a good relationship with her parents, but she could not face up to going to her parents and asking permission to get consent to have an abortion. She went and had an illegal abortion, she died of it. Her parents are traveling around the country talking to state legislatures trying to get through to these people what parental consent means.
[438] Article: “In Debate on Abortion, 2 Girls Make It Real.” By Tamar Lewin. New York Times, October 27, 1991. <www.nytimes.com>
“Since Becky’s death, her parents, Karen and Bill, have traveled to 23 states to testify or lobby against parental notification laws…. Their story has appeared in a variety of publications, including Seventeen magazine and Rolling Stone.”
[439] Article: “In Debate on Abortion, 2 Girls Make It Real.” By Tamar Lewin. New York Times, October 27, 1991. <www.nytimes.com>
“Since Becky’s death, her parents, Karen and Bill, have traveled to 23 states to testify or lobby against parental notification laws…. Their story has appeared in a variety of publications, including Seventeen magazine and Rolling Stone.”
[440] Article: “Teenagers and Abortion.” By Eloise Salholz and others. Newsweek, January 8, 1990. <www.newsweek.com>
Late in the summer of ‘88, the Indianapolis high-school junior made her way to Planned Parenthood to figure out her options. She chose abortion, but not on Indiana’s terms: rather than seek the consent of one parent, as state law required, she planned to have the procedure performed on a Saturday in Kentucky. But in the interim, desperate, she tried a home remedy. By Friday she was dead.
[441] Pamphlet: “No Way Out: Young, Pregnant and Trapped by the Law.” Reproductive Freedom Project of the American Civil Liberties Union Foundation, 1991.
In the prime of her life, Becky Bell, a 17-year-old Indiana teenager, died of a massive septic infection from a botched illegal abortion. At the time, Indiana required that a young woman obtain the consent of a parent or a judge before having an abortion. To avoid “disappointing” her parents by telling them that she was pregnant, Becky did what hundreds of thousands of women did before legalized abortion—she bought “medical care” in the back alley.1 [Footnote 1: CBS 60 Minutes, February 24, 1991.]
[442] Results from a search performed September 9, 2008:
NOTE: For specific examples, see the next three footnotes.
[443] Commentary: “When the Parents Can’t Know.” By Judith Warner. New York Times, July 29, 2006. <select.nytimes.com>
“I think, first, of Becky Bell, who in 1988 died of an illegal abortion because she was too ashamed to comply with Indiana’s requirement that she notify her parents of her intent to end her pregnancy.”
[444] Article: “Pros, Cons of Parental Notification of Abortion Debated.” By Jennifer Bundy, Associated Press, February 21, 2006.
“Indiana had a parental notification law in 1988. But Bell’s daughter, Becky, did not want to tell her parents, so she had an illegal abortion. She died a week later from complications caused by dirty instruments used in the procedure, her father said after a news conference preceding the hearing.”
[445] Paper: “Parental Involvement Laws for Abortion in the United States and the United Nations Conventions on the Rights of the Child: Can International Law Secure the Right to Choose for Minors?” By Katie Hatziavramidis. Texas Journal of Women and the Law, Spring 2007. Pages 185–202. <heinonline.org>
Becky Bell, a teenager who became pregnant in Indiana, a state that requires parental consent for an abortion, was too embarrassed to tell her parents of her pregnancy.36 Instead, Becky sought an illegal abortion.37 She died of complications a week later, at the age of seventeen.38 …
Thus, the argument that parental involvement laws are beneficial because they prevent abortions rings hollow; they merely increase the possibility that a minor may delay or reject safe, legal healthcare in favor of more clandestine but potentially dangerous procedures. …
The author is an attorney in the greater Chicago area, and her interests center on human and civil rights matters, particularly employment discrimination. She has testified before the Texas Senate on parental involvement laws and been active in the fields of gender and reproductive rights for over a decade.
[446] Coroner’s report: “Rebecca Suzanne Bell.” By Dennis J. Nicholas, M.D. (Coroner of Marion County, Indiana). Case number 88-0880. October 3, 1988.
“She was somewhat improved on Wednesday but was found on Friday, September 16 when her father went home at about noon and she was ill. He took her for an x-ray which showed pneumonia bilaterally. She was hospitalized where she went into cardiopulmonary arrest later that night.”
[447] Autopsy report: “Rebecca Suzanne Bell.” By Jesse C. Giles. Forensic Division, Department of Pathology, Indiana University School of Medicine, September 17, 1988, 7:30 A.M. Signatories: John E. Pless, M.D. (Forensic Pathologist, Division of Forensic Pathology) & Jesse C. Giles, M.D. (Fellow in Forensic Pathology, Division of Forensic Pathology).
Page 1: “CAUSE OF DEATH Septic Abortion with Pneumonia … MANNER OF DEATH Undetermined”
Pages 5–6: “REPRODUCTIVE SYSTEM: … There is evidence of recent pregnancy with recent partial abortion. The uterus is enlarged consistent with current pregnancy of age approximately 2–3 months.”
[448] Entry: “septic abortion.” Merriam-Webster’s Medical Dictionary. Accessed July 1, 2019 at <www.merriam-webster.com>
“spontaneous or induced abortion associated with bacterial infection (as by E. coli, beta-hemolytic streptococci, or Clostridium perfringens)”
[449] Entry: “pneumonia.” Merriam-Webster’s Medical Dictionary. Accessed July 1, 2019 at <www.merriam-webster.com>
“an acute disease that is marked by inflammation of lung tissue accompanied by infiltration of alveoli and often bronchioles with white blood cells (as neutrophils) and fibrinous exudate, is characterized by fever, chills, cough, difficulty in breathing, fatigue, chest pain, and reduced lung expansion, and is typically caused by an infectious agent (as a bacterium, virus, or fungus)”
[450] Article: “Abortion Debate Shifting; Individuals Become Symbols in Dispute.” By Joe Frolik. Cleveland Plain Dealer, September 9, 1990. <www.cleveland.com>
“With Clark in tow, she went to a Planned Parenthood clinic where a counselor listed her options. She was told an Indiana minor has to get a parent’s written consent for an abortion.”
[451] 2022 Indiana Code, Title 16, Article 34, Chapter 2: “Requirements for Performance of Abortion; Criminal Penalties.” Accessed September 19, 2023 at <law.justia.com>
IC 16-34-2-4. Consent of parent or legal guardian or custodian; notification; waiver of consent or notification; representation by attorney; confidentiality; emergency abortions; medical records; penalties
Sec. 4. (a) No physician shall perform an abortion on an unemancipated pregnant minor less than eighteen (18) years of age without first having obtained from one (1) of the parents, a legal guardian, or a custodian accompanying the unemancipated pregnant minor:
(1) the notarized written consent of the parent, legal guardian, or custodian of the unemancipated pregnant minor;
(2) government issued proof of identification of the parent or the legal guardian or custodian of the unemancipated pregnant minor; and
(3) some evidence, which may include identification or other written documentation that provides an articulable basis for a reasonably prudent person to believe that the person is the parent or legal guardian or custodian of the unemancipated pregnant minor.
The physician shall keep records of the documents required under this subsection in the unemancipated pregnant minor’s medical file for at least seven (7) years.
(b) A minor:
(1) who objects to having to obtain the written consent of her parent or legal guardian or custodian under this section; or
(2) whose parent or legal guardian or custodian refuses to consent to an abortion;
may petition, on her own behalf or by next friend, the juvenile court in the county in which the pregnant minor resides or in which the abortion is to be performed, for a waiver of the parental consent requirement under subsection (a) and the parental notification requirement under subsection (d). A next friend may not be a physician or provider of abortion services, representative of the physician or provider, or other person that may receive a direct financial benefit from the performance of an abortion.
(c) A physician who feels that compliance with the parental consent requirement in subsection (a) would have an adverse effect on the welfare of the pregnant minor or on her pregnancy may petition the juvenile court within twenty-four (24) hours of the abortion request for a waiver of the parental consent requirement under subsection (a) and the parental notification requirement under subsection (d).
(d) Unless the juvenile court finds that it is in the best interests of an unemancipated pregnant minor to obtain an abortion without parental notification following a hearing on a petition filed under subsection (b) or (c), a parent, legal guardian, or custodian of a pregnant unemancipated minor is entitled to receive notice of the emancipated minor’s intent to obtain an abortion before the abortion is performed on the unemancipated pregnant minor. The attorney representing the unemancipated pregnant minor shall serve the notice required by this subsection by certified mail or by personal service and provide the court with documentation of the attorney’s good faith effort to serve the notice, including any return receipt for a certified mailing. The court shall retain the documentation provided in the confidential records of the waiver proceedings held under this section.
[452] Coroner’s report: “Rebecca Suzanne Bell.” By Dennis J. Nicholas, M.D. (Coroner of Marion County, Indiana). Case number 88-0880. October 3, 1988.
Investigation disclosed that REBECCA BELL became pregnant in mid-May 1988 (according to Planned Parenthood referral receipt). She did not confide this information to her parents. According to her friend, HEATHER CLARK, REBECCA BELL told the father of the unborn child about the pregnancy and he broke off all contact with her in mid-July. REBECCA BELL told HEATHER CLARK that she intended to have an abortion.
[453] Article: “Abortion Debate Shifting; Individuals Become Symbols in Dispute.” By Joe Frolik. Cleveland Plain Dealer, September 9, 1990. <www.cleveland.com>
“… Heather Clark, a neighbor and Becky’s closest friend at the time of her death. … With Clark in tow, she went to a Planned Parenthood clinic where a counselor listed her options. … Most minors, she was told, simply go out of state. Louisville is less than 100 miles away.”
[454] Coroner’s report: “Rebecca Suzanne Bell.” By Dennis J. Nicholas, M.D. (Coroner of Marion County, Indiana). Case number 88-0880. October 3, 1988.
“REBECCA BELL also reportedly has a history of substance abuse for which she was hospitalized from mid-February through April, 1988.”
[455] Article: “Abortion Debate Shifting; Individuals Become Symbols in Dispute.” By Joe Frolik. Cleveland Plain Dealer, September 9, 1990. <www.cleveland.com>
In February 1988, Becky came to her parents and said she had a drug problem. They put her in a residential program. Everyone agrees that when Becky emerged she seemed changed, more like her old self. At a family pow-wow, Bill Bell says that in a raised, firm voice, he told Becky, “We don’t want to go through that again.”
To Becky, that sounded like an ultimatum: mess up again and you’re out of the house. Clark thinks her friend was wrong—”They’re good people. They’d have stuck by her”—but that perception apparently shaped what happened next.
[456] Coroner’s report: “Rebecca Suzanne Bell.” By Dennis J. Nicholas, M.D. (Coroner of Marion County, Indiana). Case number 88-0880. October 3, 1988.
“She had told conflicting stories about abortion plans and the exact circumstances of the abortion are not known.”
[457] Article: “Abortion Debate Shifting; Individuals Become Symbols in Dispute.” By Joe Frolik. Cleveland Plain Dealer, September 9, 1990. <www.cleveland.com>
“For a time, Clark says, she was going to have an abortion. Then she was going to have the baby and put it up for adoption. Or run away to California. ‘She was just really confused,’ Clark said.”
[458] Article: “Abortion Debate Shifting; Individuals Become Symbols in Dispute.” By Joe Frolik. Cleveland Plain Dealer, September 9, 1990. <www.cleveland.com>
“According to Dr. Dennis J. Nicholas, the coroner here in Marion County, Becky Bell was killed by pneumonia brought on by the use of unsterile instruments during an illegal abortion.”
[459] Book: Choices: Women Speak Out About Abortion. Edited by Karen A Schneider. NARAL Foundation, 1997.
Chapter: “Becky Bell.” By Karen Bell (Becky’s mother). Pages 24–27.
Page 26: “The coroner performed an autopsy and called us. ‘Your Rebecca Suzanne died from an illegal, botched abortion; dirty instruments had been used.’ ”
NOTE: The county coroner did not perform the autopsy and was not present for it. See next footnote.
[460] Autopsy report: “Rebecca Suzanne Bell.” By Jesse C. Giles. Forensic Division, Department of Pathology, Indiana University School of Medicine, September 17, 1988, 7:30 A.M. Signatories: John E. Pless, M.D. (Forensic Pathologist, Division of Forensic Pathology) & Jesse C. Giles, M.D. (Fellow in Forensic Pathology, Division of Forensic Pathology).
Page 2: “IDENTIFICATION … Persons present for the autopsy included Dr. John E. Pless, Evidence Technician Jim Floyd, Mr. Steven O’Neal and David Becsey.”
Page 4: “LUNGS … Bronchopneumonia is bilateral with the left lower lobe being severe and the left and right upper lobes being moderate.”
[461] Phone call from Just Facts to Marion County Coroner’s Office, August 21, 2008.
“Dr. Dennis Nicholas is no longer a coroner and he has passed.”
[462] Article: “In Debate on Abortion, 2 Girls Make It Real.” By Tamar Lewin. New York Times, October 27, 1991. <www.nytimes.com>
“Since Becky’s death, her parents, Karen and Bill, have traveled to 23 states to testify or lobby against parental notification laws…. They have appeared on ‘60 Minutes,’ walking through their daughter’s graveyard and talking about how they blame the law for their daughter’s death.”
[463] Book: Choices: Women Speak Out About Abortion. Edited by Karen A Schneider. NARAL Foundation, 1997.
Chapter: “Becky Bell.” By Karen Bell (Becky’s mother). Pages 24–27.
Page 26: “One day, we got a letter from Peter Jennings. He wanted us to be on the news to talk about Becky, who was the first teenager known to die because of a parental consent law.”
[464] Article: “Abortion Debate Shifting; Individuals Become Symbols in Dispute.” By Joe Frolik. Cleveland Plain Dealer, September 9, 1990. <www.cleveland.com>
“This summer, Bill Bell quit his job. For the next year, he and Karen will tour the country talking against parental involvement laws, their expenses paid by Smeal’s Fund for the Feminist Majority.”
[465] Article: “A Rush to Blame in Becky Bell’s Death.” By Cal Thomas. Washington Times, August 9, 1990. Page G1.
“Miss Bell’s parents have announced plans to use their daughter’s death as a rallying cry against such laws. They also have participated in the creation of a video they want to show in public schools and universities that they hope will lead to the repeal of parental consent legislation.”
[466] Article: “In Debate on Abortion, 2 Girls Make It Real.” By Tamar Lewin. New York Times, October 27, 1991. <www.nytimes.com>
Since Becky’s death, her parents, Karen and Bill, have traveled to 23 states to testify or lobby against parental notification laws, and advocates say it was largely the power of the Bells’ personal appearances that persuaded Oregon voters to defeat a referendum on such a law last year. …
The Fund [Fund for the Feminist Majority] credits the Bells for the defeat of the Oregon referendum last year, the nation’s first state referendum on parental notification. A few months before the election, polls had shown opposition at 22 percent to requiring parental notification, but after the Bells’ tour, including rallies, television appearances and talk shows, 52 percent of the voters supported teen-agers’ free access to abortion.
[467] Article: “In Debate on Abortion, 2 Girls Make It Real.” By Tamar Lewin. New York Times, October 27, 1991. <www.nytimes.com>
Since Becky’s death, her parents, Karen and Bill, have traveled to 23 states to testify or lobby against parental notification laws, and advocates say it was largely the power of the Bells’ personal appearances that persuaded Oregon voters to defeat a referendum on such a law last year. …
The Fund [Fund for the Feminist Majority] credits the Bells for the defeat of the Oregon referendum last year, the nation’s first state referendum on parental notification. A few months before the election, polls had shown opposition at 22 percent to requiring parental notification, but after the Bells’ tour, including rallies, television appearances and talk shows, 52 percent of the voters supported teen-agers’ free access to abortion.
[468] Webpage: “60 Minutes (Waiting to Go Home, Becky’s Story, Kuwait Update).” The Paley Center for Media, February 24, 1991. <www.paleycenter.org>
Morely Safer examines the story of seventeen-year-old Becky Bell, who died from an illegal abortion she sought out after learning of the very strict parental-consent laws in her home state, Indiana. Safer finds that the young woman has become an icon for the pro-choice movement; its representatives feel that the consent laws are “predicated on the perfect situation-comedy idea of the American family,” as one protester puts it. Safer also talks with members of a few pro-life groups, who have come under fire for attacking Becky’s character in the aftermath of her death.
[469] Webpage: “The Mission of Human Life International.” Accessed September 8, 2008 at <www.hli.org>
“The mission of HLI [Human Life International] is to promote and defend the sanctity of life and family around the world according to the teachings of the Roman Catholic Church through prayer, service and education.”
[470] Commentary: “In Indiana and Maryland, a Tale of Two Abortions.” By James A. Miller. Baltimore Evening Sun, February 15, 1991. <www.baltimoresun.com>
“James A. Miller is director of research for Human Life International, an anti-abortion group in Gaithersburg.”
[471] Autopsy report: “Rebecca Suzanne Bell.” By Jesse C. Giles. Forensic Division, Department of Pathology, Indiana University School of Medicine, September 17, 1988, 7:30 A.M. Signatories: John E. Pless, M.D. (Forensic Pathologist, Division of Forensic Pathology) & Jesse C. Giles, M.D. (Fellow in Forensic Pathology, Division of Forensic Pathology).
[472] Entry: “abortion.” American Heritage Dictionary of Science. Houghton Mifflin, 1986.
Definition a: “birth that occurs before the embryo or fetus develops enough to live on its own, usually during the first twelve weeks of pregnancy (spontaneous abortion) … SYN: miscarriage.”
Pages ix–xi:
The expert help of the Editorial Committee [of Contributing Scientists] has enabled us to formulate definitions and explanations that correspond to recent findings of scientists working in their various disciplines. Precise editorial review in the offices of the publisher has contributed to a standard of excellence.
This is a dictionary of the basic terms of the physical and the biological sciences. …
The compiling of a specialized dictionary is, perhaps more than in most other reference books, the result of many scholars and editors working together. We are fortunate to have an outstanding group of active scientists, who read, commented upon and corrected the entire manuscript, and we are indented to them for their thorough work.
[473] Commentary: “In Indiana and Maryland, a Tale of Two Abortions.” By James A. Miller. Baltimore Evening Sun, February 15, 1991. Page A21. <www.baltimoresun.com>
I tracked down the doctor who performed Becky Bell’s autopsy, Jesse Giles. Incredibly enough, Becky Bell’s parents … never bothered to talk to the doctor who wrote the report.
When Giles wrote the word “abortion” in his autopsy report, he never imagined that abortion advocates would one day look over his shoulder and seize upon that word to promote their agenda. Giles used the word “abortion” in the way it had always been used in medicine prior to the national debate. He meant a spontaneous abortion. In short, he meant a miscarriage.
If Giles had meant a deliberate, surgical abortion, he would have used the word “induced” to describe it. Giles told me that there is no evidence of an induced abortion, and in his professional opinion Becky Bell suffered a miscarriage.
Unfortunately, another pathologist stuck the word “septic” immediately before the word “abortion” on the report’s cover page.
[474] Press release: “Human Life International Comments on HBO’s ‘Pro-Abortion Fraud’: The Becky Bell Story.” PR Newswire, October 20, 1992. <www.prnewswire.com>
Giles believes Becky Bell “underwent a spontaneous abortion, a miscarriage.”3
Moreover, Giles has flatly stated that “I am astounded that they would assert that my (autopsy) report proves that there was an instrumented, illegal abortion.”4 …
3 Personal communications, Dr. Jesse C. Giles with James A. Miller, HLI [Human Life International] Director of Research, fall and winter of 1990, spring 1991.
4 Personal communication, Dr. Jesse C. Giles, Feb. 25, 1991, the day after CBS’s “60 Minutes” broadcast of “The Becky Bell Story.” The “they” referred to by Giles was “60 Minutes” and the Bell parents.
[475] Emails from Just Facts to Dr. Giles on July 31, 2008 and August 11, 2008.
NOTE: Giles did not reply.
[476] Phone call from Just Facts to Dr. Giles, August 11th, 2008.
Dr. Giles replied, “I don’t really want to talk about the case.”
[477] Phone call to Just Facts from Marion County Coroner’s Office, August 21, 2008.
“Dr. Dennis Nicholas is no longer a coroner and he has passed.”
[478] Autopsy report: “Rebecca Suzanne Bell.” By Jesse C. Giles. Forensic Division, Department of Pathology, Indiana University School of Medicine, September 17, 1988, 7:30 A.M. Signatories: John E. Pless, M.D. (Forensic Pathologist, Division of Forensic Pathology) & Jesse C. Giles, M.D. (Fellow in Forensic Pathology, Division of Forensic Pathology).
[479] Email from Dr. Pless to Just Facts on August 4, 2008:
“Jesse Giles … was a fellow in training at the time of the autopsy. He was present for the autopsy—but he was operating under my supervision.”
[480] Article: “Abortion Debate Shifting; Individuals Become Symbols in Dispute.” By Joe Frolik. Cleveland Plain Dealer, September 9, 1990. <www.cleveland.com>
While performing an autopsy on her, Dr. John Pless, head of forensic pathology at Indiana University Medical Center, found fetal material and evidence of an infection in Becky’s genital tract. To him, that indicated a botched abortion.† …
Pathologist Pless says, “we can’t determine” precisely how Bell died. He found no evidence of internal injury, which he felt ruled out a self-induced abortion. Nor were there any marks on Becky’s cervix that would be left by the instruments commonly used for clinic abortions. He theorizes someone pushed something up her cervix without leaving a sign. …
“I cannot prove she had an illegal abortion. I cannot prove she had anything but a spontaneous abortion,” said Pless, who said he based his conclusions on “the percentages” of what would most likely to produce the results he observed.
† NOTE: When asked by Just Facts if this was an accurate representation of his view, Dr. Pless responded, “I did not say that it was a botched abortion. Those are not my words. I would never use the work ‘botched’. It could have been an abortion performed correctly by all standards that got infected. If Becky Bell’s parents knew that she had had surgery then they could have taken her to the doctor for antibiotic therapy which would have saved her life if administered when she first developed symptoms.” [Email from Dr. Pless to Just Facts, August 1, 2008.]
[481] Autopsy report: “Rebecca Suzanne Bell.” By Jesse C. Giles. Forensic Division, Department of Pathology, Indiana University School of Medicine, September 17, 1988, 7:30 A.M. Signatories: John E. Pless, M.D. (Forensic Pathologist, Division of Forensic Pathology) & Jesse C. Giles, M.D. (Fellow in Forensic Pathology, Division of Forensic Pathology). Pages 5–6:
REPRODUCTIVE SYSTEM … There is evidence of recent pregnancy with recent partial abortion. The uterus is enlarged consistent with current pregnancy of age approximately 2–3 months. … The lower third of the uterine cavity has only the usual flat mucosa without obvious evidence of instrumentation. However, the upper 2/3 of the uterine cavity has a mixture of blood clot and necrotic [dead] and hemorrhagic [bloody] products of conception. … The serosa [outer lining] of the uterus is smooth and glistening and without exudate [anything oozing from it], and there are no areas of perforation or pus in or around the uterus.
[482] Emails from Dr. Pless to Just Facts:
August 1, 2008: “The infection spread through the blood stream from the uterus to the lungs. The source of the infection was the tissue products from the pregancy [sic] that had been incompletely removed.”
August 4, 2008: “I can not rule out a spontaneous abortion. The presence of infection suggests that it was not spontaneous.”
August 11, 2008: “The same micro-organism was cultured in the uterus and the lung. It is unlikely that the infection originated in the lung and then went to the uterus.”
[483] Autopsy report: “Rebecca Suzanne Bell.” By Jesse C. Giles. Forensic Division, Department of Pathology, Indiana University School of Medicine, September 17, 1988, 7:30 A.M. Signatories: John E. Pless, M.D. (Forensic Pathologist, Division of Forensic Pathology) & Jesse C. Giles, M.D. (Fellow in Forensic Pathology, Division of Forensic Pathology). Page 6:
SPECIMENS FOR CULTURE: Blood bacterial culture, lung tissue swabs for bacterial culture and bilateral pleural [membrane surrounding the lungs and chest cavity] fluid swabs for bacterial culture.
MICROSCOPIC EXAMINATION: Tissue samples representative of the major organs have been processed onto glass slides for microscopic examination. These histologic specimens have been examined and there are no additional significant pathologic findings other than those noted on the Anatomic Findings.
[484] Autopsy report: “Rebecca Suzanne Bell.” By Jesse C. Giles. Forensic Division, Department of Pathology, Indiana University School of Medicine, September 17, 1988, 7:30 A.M. Signatories: John E. Pless, M.D. (Forensic Pathologist, Division of Forensic Pathology) & Jesse C. Giles, M.D. (Fellow in Forensic Pathology, Division of Forensic Pathology). Pages 3–4:
“NECK ORGANS: The mucosa of the hypopharynx, larynx and trachea is smooth and glistening without ulceration or tumor.”
[485] Email from Dr. Pless to Just Facts, August 21, 2008.
“There was no upper airway disease—so the only possiblity [sic] was spread from the uterus. Yes, my memory could be faulty after 20 years.”
[486] Autopsy report: “Rebecca Suzanne Bell.” By Jesse C. Giles. Forensic Division, Department of Pathology, Indiana University School of Medicine, September 17, 1988, 7:30 A.M. Signatories: John E. Pless, M.D. (Forensic Pathologist, Division of Forensic Pathology) & Jesse C. Giles, M.D. (Fellow in Forensic Pathology, Division of Forensic Pathology).
Page 2: “Circumstantial Summary … Blood culture from the hospital showed no growth, but sputum [mucus and other matter from the lungs] cultures grew streptococcus pneumoniae.”
[487] Paper: “Role of Two-Component Systems in the Virulence of Streptococcus Pneumoniae.” By G. K. Paterson and others. Journal of Medical Microbiology, 2006. Pages 355–363. <www.microbiologyresearch.org>
Page 355:
Understanding of how the human pathogen Streptococcus pneumoniae perceives and responds to its environment in the host offers insight into the pathogenesis of disease caused by this important bacterium and the potential for improved interventions. …
… S. pneumoniae is normally found as a harmless commensal of the human upper respiratory tract. However, depending on host and bacterial factors that are not fully understood, the pneumococcus is also a major cause of diseases such as pneumonia, meningitis, septicaemia, bronchitis and otitis media. …
Page 357: “[T]he importance of genes to virulence varies with the site of infection….”
Page 361: “Pneumococcal [Streptococcus pneumoniae] TCSs [two-component systems] are important virulence factors of this significant human pathogen. Interestingly, their contribution to virulence can vary depending on pneumococcal strain and infection site.”
[488] Autopsy report: “Rebecca Suzanne Bell.” By Jesse C. Giles. Forensic Division, Department of Pathology, Indiana University School of Medicine, September 17, 1988, 7:30 A.M. Signatories: John E. Pless, M.D. (Forensic Pathologist, Division of Forensic Pathology) & Jesse C. Giles, M.D. (Fellow in Forensic Pathology, Division of Forensic Pathology).
Page 2: “Circumstantial Summary … Blood culture from the hospital showed no growth, but sputum [mucus and other matter from the lungs] cultures grew streptococcus pneumoniae.”
[489] Book: Case Files: Microbiology (2nd edition). By Eugene C. Toy and others. McGraw-Hill Medical, 2008.
Page 150: “Streptococcus pneumoniae (pneumococcus) … commonly colonizes the upper airway in humans, more frequently in children than adults. … Pneumococcal pneumonia typically follows a milder upper respiratory infection.”
[490] Book: School Nurse Emergency Care Course (2nd edition). Loyola University Medical Center, 2003.
Page 146:
In viral pneumonia, the history includes an upper respiratory infection of gradual onset. Bacterial pneumonia has a more sudden onset; the student will usually appear ill, with fever, chills, cough, and chest pain.
The signs and symptoms that accompany pneumonia in older children include a nonproductive cough, fever, pleural pain, dyspnea, and an increased respiratory rate.
NOTE: Observe that there is no mention of upper airway disease in the quote above.
[491] Email from Dr. Pless to Just Facts, September 2, 2008:
I suppose that you could make an arguement (sic) for almost anything. The absence of gross pus in the uterus does not rule it out as the source of the infection. You would expect the serosa of the uterus to be smooth and glistening since the source of the infection was the instrumentation of the intrauterine cavity. Thank you for seeking my opinion. I have no reason to modify the report.
Note: Just Facts did not ask Dr. Pless to modify the report. Just Facts only asked him to explain the discrepancy between his statement to the media and the report.
[492] Article: “Teen-Agers Face Reality On Both Sides of Screen.” By John J. O’Connor. New York Times, October 13, 1992. <www.nytimes.com>
“Becky ends up having an illegal abortion and dying of a resultant infection. … ‘The Becky Bell Story’ is tough and persuasive.”
[493] Press release: “Human Life International Comments on HBO’s ‘Pro-Abortion Fraud’: The Becky Bell Story.” PR Newswire, October 20, 1992. <www.prnewswire.com>
“Becky, accompanied by best friend ‘Kelly,’ is shown entering a small building in a seedy part of town and then walking upstairs to meet her illegal, ‘back-alley’ abortionists.”
[494] Coroner’s report: “Rebecca Suzanne Bell.” By Dennis J. Nicholas, M.D. (Coroner of Marion County, Indiana). Case number 88-0880. October 3, 1988.
[495] Autopsy report: “Rebecca Suzanne Bell.” By Jesse C. Giles. Forensic Division, Department of Pathology, Indiana University School of Medicine, September 17, 1988, 7:30 A.M. Signatories: John E. Pless, M.D. (Forensic Pathologist, Division of Forensic Pathology) & Jesse C. Giles, M.D. (Fellow in Forensic Pathology, Division of Forensic Pathology).
[496] Book: Choices: Women Speak Out About Abortion. Edited by Karen A Schneider. NARAL Foundation, 1997.
Chapter: “Becky Bell.” By Karen Bell (Becky’s mother). Pages 24–27.
[497] Article: “Abortion Debate Shifting; Individuals Become Symbols in Dispute.” By Joe Frolik. Cleveland Plain Dealer, September 9, 1990. <www.cleveland.com>
… Heather Clark, a neighbor and Becky’s closest friend at the time of her death.
… With Clark in tow, she went to a Planned Parenthood clinic where a counselor listed her options. …
Heather Clark fought back anger—she didn’t believe then her friend had had an abortion and still doesn’t. …
Thursday night, Clark stopped by to visit. She says Becky asked her to schedule an abortion in Louisville for Saturday.
[498] Coroner’s report: “Rebecca Suzanne Bell.” By Dennis J. Nicholas, M.D. (Coroner of Marion County, Indiana). Case number 88-0880. October 3, 1988.
“REBECCA BELL reportedly was at a party where various drugs were being used (cocaine, ‘speed’ and LSD) on the week-end of September 10–11, claimed that someone had put ‘speed’ or cocaine in her drink.”
[499] Book: Choices: Women Speak Out About Abortion. Edited by Karen A Schneider. NARAL Foundation, 1997.
Chapter: “Becky Bell.” By Karen Bell (Becky’s mother). Pages 24–27.
Page 25: “I was laying awake in bed waiting for her to come home. At 12:45 in the morning, I heard her trying to open the door. She was crying and said, ‘Mom, it was a horrible party. I feel like I’ve got the flu like Dad.’ ”
[500] Article: “Abortion Debate Shifting; Individuals Become Symbols in Dispute.” By Joe Frolik. Cleveland Plain Dealer, September 9, 1990. <www.cleveland.com>
“On Tuesday, she fainted at work.”
[501] Article: “Abortion Debate Shifting; Individuals Become Symbols in Dispute.” By Joe Frolik. Cleveland Plain Dealer, September 9, 1990. <www.cleveland.com>
“On Tuesday, she fainted at work. She stayed home the next two days, resisting her parents’ pleas that she go to the doctor.”
NOTE: Observe that there is a possible disparity with the next footnote regarding the first day in which she stayed home from school.
[502] Coroner’s report: “Rebecca Suzanne Bell.” By Dennis J. Nicholas, M.D. (Coroner of Marion County, Indiana). Case number 88-0880. October 3, 1988.
“On Tuesday, September 13, she awoke with a neck ache, stayed home from school and developed an elevated temperature. She was somewhat improved on Wednesday….”
[503] Book: Choices: Women Speak Out About Abortion. Edited by Karen A Schneider. NARAL Foundation, 1997.
Chapter: “Becky Bell.” By Karen Bell (Becky’s mother). Pages 24–27.
Page 25:
After school on Monday, she still felt sick. By Wednesday she had a fever of 104 and a strange cough. I told her we were going to the doctor. She turned white. She said, “Mom, oh, Mom, please, oh, please, I don’t want to go. Just give me some aspirin and I’ll be okay, please, please.”
She was nearly hysterical, so I respected her wishes.
[504] Article: “Abortion Debate Shifting; Individuals Become Symbols in Dispute.” By Joe Frolik. Cleveland Plain Dealer, September 9, 1990. <www.cleveland.com>
“Thursday night, Clark stopped by to visit. She says Becky asked her to schedule an abortion in Louisville for Saturday.”
[505] Article: “Abortion Debate Shifting; Individuals Become Symbols in Dispute.” By Joe Frolik. Cleveland Plain Dealer, September 9, 1990. <www.cleveland.com>
Friday morning, Becky staggered to the bathroom. Bleeding. Her mom assumed she was having her period. After helping Becky back to bed, she insisted they go to the doctor. At last, Becky agreed.
The family physician diagnosed severe pneumonia and sent her to the hospital.
[506] Coroner’s report: “Rebecca Suzanne Bell.” By Dennis J. Nicholas, M.D. (Coroner of Marion County, Indiana). Case number 88-0880. October 3, 1988.
“She was somewhat improved on Wednesday but was found on Friday, September 16 when her father went home at about noon and she was ill. He took her for an x-ray which showed pneumonia bilaterally.”
[507] Autopsy report: “Rebecca Suzanne Bell.” By Jesse C. Giles. Forensic Division, Department of Pathology, Indiana University School of Medicine, September 17, 1988, 7:30 A.M. Signatories: John E. Pless, M.D. (Forensic Pathologist, Division of Forensic Pathology) & Jesse C. Giles, M.D. (Fellow in Forensic Pathology, Division of Forensic Pathology).
Page 2: “Circumstantial Summary … She was taken to St. Vincent hospital approximately 4:00 PM on Friday, September 16, 1988.”
[508] Book: Choices: Women Speak Out About Abortion. Edited by Karen A Schneider. NARAL Foundation, 1997.
Chapter: “Becky Bell.” By Karen Bell (Becky’s mother). Pages 24–27.
Page 26: “Late that night, with grandma, grandpa, and other relatives gathered, the doctor said, ‘We don’t know if we can save the baby.’ And I thought, ‘The baby? My God, Becky was pregnant.’ ”
[509] Autopsy report: “Rebecca Suzanne Bell.” By Jesse C. Giles. Forensic Division, Department of Pathology, Indiana University School of Medicine, September 17, 1988, 7:30 A.M. Signatories: John E. Pless, M.D. (Forensic Pathologist, Division of Forensic Pathology) & Jesse C. Giles, M.D. (Fellow in Forensic Pathology, Division of Forensic Pathology).
Page 2: “Circumstantial Summary … She subsequently experienced an unexpected cardiopulmonary arrest, and was transferred to the Intensive Care Unit where she died at 11:29 PM on September 16, 1988.”
[510] Autopsy number 89-593: “Erica Richardson.” By Julia C. Goodin & others. Office of the Chief Medical Examiner, State of Maryland, June 28, 1989. Autopsy performed on March 3, 1989. <health.maryland.gov>
Page 1: “Description of Injury … Close examination of the anterior portion of the uterus showed a large irregular perforation of the anterior lower uterine wall which extended into a portion of the cervix.”
Page 5:
Opinion: This, 16 year old black female, Erica Richardson, died from rupture of lower uterus and cervix with complications, including hemorrhage into the pelvic cavity surrounding the uterus and air embolism (air escaping into the vasculature and heart). According to police reports, the deceased was known to have been pregnant and this is consistent with autopsy findings. However, she had undergone an evacuation [abortion] procedure which resulted in perforation of the uterus.
[511] Article: “Teen’s Death After Abortion Brings Suit.” By Larry Perl. Prince George’s Journal Weekly, May 30–31, 1990.
The malpractice suit claims that on the evening of March 1, 1989, Dr. Gene Crawford punctured 16-year-old Erica Kae Richardson’s uterus and cervix—then left her “bleeding to death” on an operating table in his Laurel office for four hours, without monitoring vital signs.
At 10:45 p.m., Crawford carried Richardson to her aunt’s car and told the aunt to “take [her] home and out her to bed,” the suit states. … The aunt, deciding that her niece needed “emergency treatment,” drove to Bowie Health Center, where Richardson was rushed into the emergency room at 11 p.m., in respiratory arrest, and died shortly after midnight the suit states. …
Richardson’s mother … referred questions to the attorneys. … Donald McLaughlin said Richardson’s aunt, Denise Crarey, helped Richardson get an abortion without telling Richardson’s mother. McLaughlin added that though Crarey and Richardson’s mother are sisters, they have “a very strained relationship.” Crarey, a registered nurse, took Richardson first to Washington Hospital Center, which wouldn’t perform the abortion because Richardson was too far along in her pregnancy [19 weeks], McLaughlin said.
[512] Article: “Mother Is Suing Doctor: Daughter Died After Abortion.” By Melanie Mader. Maryland Laurel Leader, June 29, 1990. Pages A1, 3.
Page 1: “[T]he 16-year-old Cheltenham girl….”
Page 3: “Richardson-Smith was unaware that her daughter was having an abortion until the Bowie medical center called her, McLaughlin said.”
[513] Press release: “Human Life International Claims Maryland Health Department ‘Ignores, Covers-Up’ Abortion Deaths.” PR Newswire, November 21, 1991. <www.prnewswire.com>
“Erica Richardson, 16, died March 2, 1989, just hours after an abortion was performed upon her by Dr. Gene O. Crawford at his Metropolitan Women’s Center, 9811 Mallard Dr., Laurel, Md.”
[515] Maryland Code, Title 20, Subtitle 1, Part I, Section 103: “Abortion.” State of Maryland. Accessed September 19, 2023 at <law.justia.com>
(a) Except as provided in subsections (b) and (c) of this section, a physician may not perform an abortion on an unmarried minor unless the physician first gives notice to a parent or guardian of the minor.
(b) The physician may perform the abortion without notice to a parent or guardian if:
(1) The minor does not live with a parent or guardian; and
(2) A reasonable effort to give notice to a parent or guardian is unsuccessful.
(c) (1) The physician may perform the abortion, without notice to a parent or guardian of a minor if, in the professional judgment of the physician:
(i) Notice to the parent or guardian may lead to physical or emotional abuse of the minor;
(ii) The minor is mature and capable of giving informed consent to an abortion; or
(iii) Notification would not be in the best interest of the minor.
(2) The physician is not liable for civil damages or subject to a criminal penalty for a decision under this subsection not to give notice.
(d) The postal receipt that shows an article of mail was sent by certified mail, return receipt requested, bearing a postmark from the United States Postal Service, to the last known address of a parent or guardian and that is attached to a copy of the notice letter that was sent in that article of mail shall be conclusive evidence of notice or a reasonable effort to give notice, as the case may be.
(e) A physician may not provide notice to a parent or guardian if the minor decides not to have the abortion.
[516] “Illinois General Assembly Questionnaire.” Independent Voters of Illinois—Independent Precinct Organization, 1996. <www.justfacts.com>
Page 9 (of PDF):
24. Do you support:
a. Medicaid funding for abortions?
Yes.
b. insurance coverage of abortions for state employees?
Yes.
c. parental consent notification for minors seeking abortions?
No.
d. any other restrictions on abortions?
No.
[517] “Illinois General Assembly Questionnaire.” Independent Voters of Illinois—Independent Precinct Organization, 1996. Fax transmittal date/time stamp: “Sep-10-96 TUE 05:26”. <www.justfacts.com>
Page 6 (of PDF):
24. Do you support:
a. Medicaid funding for abortions? Yes.
b. insurance coverage of abortions for state employees? Yes.
c. parental consent/notification for minors seeking abortions? Depends on how young – possibly for extremely young teens, i.e. 12 or 13 year olds.
d. any other restrictions on abortions. No.
[518] Article: “Liberal Views Could Haunt Obama.” By Mike Allen and Ben Smith. Politico, December 12, 2007. <www.politico.com>
“A week after Politico provided the questionnaire to the Obama campaign for comment, an aide called Monday night to say that Obama had said he did not fill out the form, and provided a contact for his campaign manager at the time, who said she filled it out.”
[519] Article: “Obama Had Greater Role on Liberal Survey.” By Kenneth P. Vogel. Politico, March 31, 2008. <www.politico.com>
“ ‘Sen. Obama didn’t fill out these state Senate questionnaires—a staffer did—and there are several answers that didn’t reflect his views then or now,’ Tommy Vietor, a spokesman for Obama’s campaign, said in an e-mailed statement.”
[520] Article: “Obama Had Greater Role on Liberal Survey.” By Kenneth P. Vogel. Politico, March 31, 2008. <www.politico.com>
But a Politico examination determined that Obama was actually interviewed about the issues on the questionnaire by the liberal Chicago nonprofit group that issued it. And it found that Obama—the day after sitting for the interview—filed an amended version of the questionnaire, which appears to contain Obama’s own handwritten notes added to one answer. …
Tommy Vietor, a spokesman for Obama’s campaign, said in an e-mailed statement. “He may have jotted some notes on the front page of the questionnaire at the meeting, but that doesn’t change the fact that some answers didn’t reflect his views. His 11 years in public office do.”
[521] “Illinois General Assembly Questionnaire.” Independent Voters of Illinois—Independent Precinct Organization, 1996. <www.justfacts.com>
Page 1 (of PDF):
Candidate Report Sheet for Interviews
Candidate Name: Barack Obama [In handwriting] …
Date of Interview: 9/9/96 [In handwriting] …
Place of Interview: 5623 S. Drexel—House of Alan and Lois Dobry [In handwriting]
[522] “Illinois General Assembly Questionnaire.” Independent Voters of Illinois—Independent Precinct Organization, 1996. Fax transmittal date/time stamp: “Sep-10-96 TUE 05:26”. <www.justfacts.com>
Page 1 (of PDF):

[523] Senate Bill 562: “Parental Notice of Abortion Act of 2001.” State of Illinois Senate, 92nd General Assembly, 2001–2002. <www.ilga.gov>
Section 10. Definitions…. “Minor” means any person under 18 years of age who is not or has not been married or who has not been emancipated under the Emancipation of Mature Minors Act. …
Section 15. Notice to adult family member. No person shall knowingly perform an abortion upon a minor or upon an incompetent person unless the person or his or her agent has given at least 48 hours actual notice to an adult family member of the pregnant minor or incompetent person of his or her intention to perform the abortion….
Section 20. Exceptions. Notice is not required under this Act if … (3) the attending physician certifies in the patient’s medical record that a medical emergency exists and there is insufficient time to provide the required notice; or the minor declares in writing that she is a victim of sexual abuse, neglect, or physical abuse by an adult family member as defined in this Act….
Section 25. Procedure for judicial waiver of notice. … A minor or incompetent person may petition any circuit court for a waiver of the parental notice of abortion requirement under this Act and may participate in proceedings on her own behalf. … All court proceedings under this Section shall be sealed. … These proceedings shall be given precedence over other pending matters to the extent necessary to ensure that the court reaches a decision promptly. … Notice under this Act shall be waived if the court finds by clear and convincing evidence either:
(1) that the minor or incompetent person is sufficiently mature and well-enough informed to decide intelligently whether to have an abortion; or
(2) that notification under Section 15 of this Act would not be in the best interests of the minor or incompetent person. …
No fees shall be required of any minor or incompetent person who avails herself of the procedures provided by this Section. …
Section 40. Penalties.
(a) A physician who willfully fails to provide notice as required under this Act before performing an abortion on a minor or an incompetent person shall be referred to the Illinois State Medical Disciplinary Board for action in accordance with Section 22 of the Medical Practice Act of 1987.
(b) A person, not authorized under this Act, who signs any waiver of notice under this Act for a minor or incompetent person seeking an abortion is guilty of a Class C misdemeanor.
[524] Vote: “Senate Bill 562, Parental Notice of Abortion Act of 2001.” State of Illinois Senate, 92nd General Assembly, April 6, 2001. <www.ilga.gov>
“P [Present] Obama”
[525] Resolution 2: “Rules of the Senate.” Senate of the 92nd General Assembly, State of Illinois, 2001–2002. <www.ilga.gov>
Article 1-12:
Majority of Those Elected. “Majority of those elected” means an absolute majority of the total number of Senators entitled to be elected to the Senate, irrespective of the number of elected or appointed Senators actually serving in office. So long as 59 Senators are entitled to be elected to the Senate, “majority of those elected” shall mean 30 affirmative votes.
Article 5-1(f): “No bill shall be passed by the Senate except on a roll call vote of a majority of those elected.”
NOTE: This rule was effective at the time of Obama’s vote. The same rule was still in effect as of June 2008.
[526] Article: “Obama Abortion Dodges Blessed by Planned Parenthood.” By Teddy Davis. ABC News, July 17, 2007. <bit.ly>
“We at Planned Parenthood view those as leadership votes,” Pam Sutherland, the president and CEO of the Illinois Planned Parenthood Council, told ABC News. “We worked with him specifically on his strategy. The Republicans were in control of the Illinois Senate at the time. They loved to hold votes on ‘partial birth’ and ‘born alive’. They put these bills out all the time … because they wanted to pigeonhole Democrats.” …
“What it did,” she continued, “was give cover to moderate Democrats who wanted to vote with us but were afraid to do so” because of how their votes would be used against them electorally. “A ‘present’ vote would protect them. Your senator voted ‘present.’ Most of the electorate is not going to know what that means.”
NOTE: The next footnote independently confirms Sutherland’s assertion that she and Obama worked together on abortion-related legislation.
[527] Speech: “Barack Obama Before Planned Parenthood Action Fund.” July 17, 2007. Transcribed by Laura Echevarria. <bit.ly>
I’m happy to see so many good friends here today, including Steve Trombley and Pam Sutherland from my home state of Illinois. We had a number of battles down in Springfield for many many years and it is wonderful to see that they are here today. …
Steve and Pam will tell you that we fought together in the Illinois State Senate against restrictive choice legislation—laws just like the federal abortion laws, the federal abortion bans that are cropping up.
[528] Questionnaire: “2004 U.S. Senate Candidates.” Independent Voters of Illinois—Independent Precinct Organization, December 15, 2003. Submitted by Barack Obama on January 5, 2004. <www.suntimes.com>
Question 28b: “Do you support parental or spousal notification or consent to obtain an abortion? I oppose spousal notification or consent. Regarding parental notification, I would oppose any legislation that does not include a bypass provision for minors who have been victims of, or have reason to fear, physical or sexual abuse.”
[529] Senate Bill 562: “Parental Notice of Abortion Act of 2001.” State of Illinois Senate, 92nd General Assembly, 2001–2002. <www.ilga.gov>
Section 10. Definitions…. “Minor” means any person under 18 years of age who is not or has not been married or who has not been emancipated under the Emancipation of Mature Minors Act. …
Section 15. Notice to Adult Family Member. No person shall knowingly perform an abortion upon a minor or upon an incompetent person unless the person or his or her agent has given at least 48 hours actual notice to an adult family member of the pregnant minor or incompetent person of his or her intention to perform the abortion….
Section 20. Exceptions. Notice is not required under this Act if … (3) the attending physician certifies in the patient’s medical record that a medical emergency exists and there is insufficient time to provide the required notice; or the minor declares in writing that she is a victim of sexual abuse, neglect, or physical abuse by an adult family member as defined in this Act….
Section 25. Procedure for Judicial Waiver of Notice. … A minor or incompetent person may petition any circuit court for a waiver of the parental notice of abortion requirement under this Act and may participate in proceedings on her own behalf. … All court proceedings under this Section shall be sealed. … These proceedings shall be given precedence over other pending matters to the extent necessary to ensure that the court reaches a decision promptly. … Notice under this Act shall be waived if the court finds by clear and convincing evidence either:
(1) that the minor or incompetent person is sufficiently mature and well-enough informed to decide intelligently whether to have an abortion; or
(2) that notification under Section 15 of this Act would not be in the best interests of the minor or incompetent person. …
No fees shall be required of any minor or incompetent person who avails herself of the procedures provided by this Section. …
Section 40. Penalties.
(a) A physician who willfully fails to provide notice as required under this Act before performing an abortion on a minor or an incompetent person shall be referred to the Illinois State Medical Disciplinary Board for action in accordance with Section 22 of the Medical Practice Act of 1987.
(b) A person, not authorized under this Act, who signs any waiver of notice under this Act for a minor or incompetent person seeking an abortion is guilty of a Class C misdemeanor.
[530] Vote: “Senate Bill 562, Parental Notice of Abortion Act of 2001.” State of Illinois Senate, 92nd General Assembly, April 6, 2001. <www.ilga.gov>
“P [Present] Obama”
[531] Article: “Sen. Barack Obama’s RH [Reproductive Health] Issues Questionnaire.” By Andrea Lynch. RH Reality Check, December 21, 2007. <www.rhrealitycheck.org>
Does Sen. Obama Believe Adolescents Should Have the Right to Choose Abortion, or Should They Be Required to Seek Their Parents’ Consent? Why or Why Not? Are There Any Circumstances That Might Make a Compelling Case for Waiving the Parental Consent Requirement?
As a parent, Obama believes that young women, if they become pregnant, should talk to their parents before considering an abortion. But he realizes not all girls can turn to their mother or father in times of trouble, and in those instances, we should want these girls to seek the advice of trusted adults—an aunt, a grandmother, a pastor.
Unfortunately, instead of encouraging pregnant teens to seek the advice of adults, most parental consent bills that come before Congress or state legislatures criminalize adults who attempt to help a young woman in need and lack judicial bypass and other provisions that would permit exceptions in compelling cases.
[532] Bypass Provisions for State Abortion Parental Consent and Notification Laws. This table was made through research conducted on July 28–29, 2008 of each state’s codes/statutes. Most of these provisions are for judicial bypass, although some states allow doctors to invoke them.
|
State |
Code/Statute |
Operative Language for Exceptions |
|
AL* |
§26-21 |
“best interest of the minor” |
|
AK |
§18.16 |
“physical abuse, sexual abuse, or a pattern of emotional abuse … minor’s best interest” |
|
AZ |
§36-2152 |
“her best interests … sexual conduct with a minor by the minor’s parent, stepparent, uncle, grandparent, sibling …” |
|
AR |
§20-16-804 |
“her best interests” |
|
CA* |
§123450 |
“minor’s best interest” |
|
CO |
§12-37.5-105, §12-37.5-107 |
“child abuse or neglect”, “best interest of the minor” |
|
DE |
Title 24, §1784 |
“best interest of the minor” |
|
FL |
Title 29, §390.01114 |
“child abuse or sexual abuse of the petitioner by one or both of her parents or her guardian … best interest of the petitioner” |
|
GA |
§15-11-112 |
“best interests of the minor” |
|
ID |
§18-609A |
“best interests of the minor” |
|
IL* |
Chap. 750, §70/20, §70/25 |
“victim of sexual abuse, neglect, or physical abuse by an adult family member”, “best interests of the minor” |
|
IN |
§16-34-2-4 |
“minor’s best interests” |
|
IA |
§135L.3 |
“best interest of the pregnant minor” |
|
KS |
§65-6705 |
“best interest of the minor” |
|
KY |
§311.732 |
“best interest of the minor” |
|
LA |
§40.1299.35.5 |
“best interest of the minor” |
|
MD |
§20-103 |
“physical or emotional abuse of the minor … best interest of the minor” |
|
MA |
Chapter 112, §12s |
“in her best interests” |
|
MI |
§722.904 |
“best interests of the minor” |
|
MN* |
§144.343 |
“victim of sexual abuse, neglect, or physical abuse” |
|
MS |
§41-41-55 |
“best interests of the minor” |
|
MO |
§188.028. 2 |
“best interest of the minor” |
|
MT |
§50-20-212 |
“physical, sexual, or emotional abuse of the petitioner by one or both parents, a guardian, or a custodian … best interests of the petitioner” |
|
NE |
§71-6903, §71-6906 |
“best interests of the pregnant woman”, “victim of abuse … sexual abuse … child abuse” |
|
NV* |
§442.255 |
“her best interests” |
|
NJ* |
§9:17A-1.7 |
“physical, sexual or emotional abuse of the minor by the parent, guardian or legal custodian … best interests of the minor” |
|
NM* |
§30-5-1 |
[No exceptions] |
|
NC |
§90-21.8 |
“minor’s best interests” |
|
ND |
§14-02.1-03.1 |
“best interests of the minor” |
|
OH |
§2919.121 |
“best interests of the minor” |
|
OK |
Title 63, §1-740.2, §1-740.3 |
“victim of sexual abuse”, “her best interest” |
|
PA |
§3206 |
“best interests of the woman” |
|
RI |
§23-4.7-6 |
“her best interests” |
|
SC |
§44-41-30, §44-41-32 |
“pregnancy is the result of incest”, “best interest of the minor” |
|
SD |
§34-23A-7 |
“her best interests” |
|
TN |
§37-10-304 |
“minor’s best interests” |
|
TX |
§33.003 |
“minor’s best interest … physical, sexual, or emotional abuse of the minor” |
|
UT |
§76-7-304.4, §76-7-304.5 |
“incest … parent or guardian has abused the minor … parent or guardian has not assumed responsibility for the minor’s care and upbringing”, “minor’s best interest” |
|
VA |
§16.1-241 |
“her best interest … abused or neglected” |
|
WV |
§16-2F-3 |
“minor’s best interest” |
|
WI |
§48.375 |
“sexual assault … pregnancy is the result of sexual intercourse with a caregiver … minor’s best interests” |
|
WY |
§35-6-118 |
“best interest of the minor” |
* Law blocked by court order or ruling.
[533] Vote 263: “Motion to Invoke Cloture on the Motion to Concur in House Amendment to S.403.” U.S. Senate, September 29, 2006. <www.senate.gov>
|
Party |
Voted “Yes” |
Voted “No” |
Voted “Present” or Did Not Vote† |
|||
|
Number |
Portion |
Number |
Portion |
Number |
Portion |
|
|
Republican |
51 |
93% |
4 |
7% |
0 |
0% |
|
Democrat |
6 |
14% |
37 |
84% |
1 |
2% |
|
Independent |
0 |
0% |
1 |
100% |
0 |
0% |
|
NOTE: †Voting “Present” is effectively the same as not voting. |
||||||
|
Grouped by Vote Position |
||
|
Yeas — 57 |
||
|
Alexander (R-TN) |
Dole (R-NC) |
McCain (R-AZ) |
|
Allard (R-CO) |
Domenici (R-NM) |
McConnell (R-KY) |
|
Allen (R-VA) |
Ensign (R-NV) |
Murkowski (R-AK) |
|
Bennett (R-UT) |
Enzi (R-WY) |
Nelson (D-NE) |
|
Bond (R-MO) |
Frist (R-TN) |
Pryor (D-AR) |
|
Brownback (R-KS) |
Graham (R-SC) |
Reid (D-NV) |
|
Bunning (R-KY) |
Grassley (R-IA) |
Roberts (R-KS) |
|
Burns (R-MT) |
Gregg (R-NH) |
Santorum (R-PA) |
|
Burr (R-NC) |
Hagel (R-NE) |
Sessions (R-AL) |
|
Byrd (D-WV) |
Hatch (R-UT) |
Shelby (R-AL) |
|
Chambliss (R-GA) |
Hutchison (R-TX) |
Smith (R-OR) |
|
Coburn (R-OK) |
Inhofe (R-OK) |
Stevens (R-AK) |
|
Cochran (R-MS) |
Isakson (R-GA) |
Sununu (R-NH) |
|
Coleman (R-MN) |
Johnson (D-SD) |
Talent (R-MO) |
|
Cornyn (R-TX) |
Kyl (R-AZ) |
Thomas (R-WY) |
|
Craig (R-ID) |
Landrieu (D-LA) |
Thune (R-SD) |
|
Crapo (R-ID) |
Lott (R-MS) |
Vitter (R-LA) |
|
DeMint (R-SC) |
Lugar (R-IN) |
Voinovich (R-OH) |
|
DeWine (R-OH) |
Martinez (R-FL) |
Warner (R-VA) |
|
Nays — 42 |
||
|
Akaka (D-HI) |
Dorgan (D-ND) |
Menendez (D-NJ) |
|
Baucus (D-MT) |
Durbin (D-IL) |
Mikulski (D-MD) |
|
Bayh (D-IN) |
Feingold (D-WI) |
Murray (D-WA) |
|
Biden (D-DE) |
Feinstein (D-CA) |
Nelson (D-FL) |
|
Bingaman (D-NM) |
Harkin (D-IA) |
Obama (D-IL) |
|
Boxer (D-CA) |
Inouye (D-HI) |
Reed (D-RI) |
|
Cantwell (D-WA) |
Jeffords (I-VT) |
Rockefeller (D-WV) |
|
Carper (D-DE) |
Kerry (D-MA) |
Salazar (D-CO) |
|
Chafee (R-RI) |
Kohl (D-WI) |
Sarbanes (D-MD) |
|
Clinton (D-NY) |
Lautenberg (D-NJ) |
Schumer (D-NY) |
|
Collins (R-ME) |
Leahy (D-VT) |
Snowe (R-ME) |
|
Conrad (D-ND) |
Levin (D-MI) |
Specter (R-PA) |
|
Dayton (D-MN) |
Lieberman (D-CT) |
Stabenow (D-MI) |
|
Dodd (D-CT) |
Lincoln (D-AR) |
Wyden (D-OR) |
|
Not Voting — 1 |
||
|
Kennedy (D-MA) |
||
[534] House of Representatives Amendment to Senate Bill 403: “Child Interstate Abortion Notification Act.” 109th Congress (2005–2006), September 26, 2006. <www.congress.gov>
Sec. 2431. Transportation of Minors in Circumvention of Certain Laws Relating to Abortion
(a) Offense—
(1) Generally—Except as provided in subsection (b), whoever knowingly transports a minor across a State line, with the intent that such minor obtain an abortion, and thereby in fact abridges the right of a parent under a law requiring parental involvement in a minor’s abortion decision, in force in the State where the minor resides, shall be fined under this title or imprisoned not more than one year, or both.
(b) Exceptions—
(1) The prohibition of subsection (a) does not apply if the abortion was necessary to save the life of the minor because her life was endangered by a physical disorder, physical injury, or physical illness, including a life endangering physical condition caused by or arising from the pregnancy itself.
(2) A minor transported in violation of this section, and any parent of that minor, may not be prosecuted or sued for a violation of this section, a conspiracy to violate this section, or an offense under section 2 or 3 based on a violation of this section. …
Sec. 2435. Child Interstate Abortion Notification
(a) Offense—
(1) Generally—A physician who knowingly performs or induces an abortion on a minor in violation of the requirements of this section shall be fined under this title or imprisoned not more than one year, or both.
(2) Parental Notification—A physician who performs or induces an abortion on a minor who is a resident of a State other than the State in which the abortion is performed must provide, or cause his or her agent to provide, at least 24 hours actual notice to a parent of the minor before performing the abortion. If actual notice to such parent is not possible after a reasonable effort has been made, 24 hours constructive notice must be given to a parent.
(b) Exceptions—The notification requirement of subsection (a)(2) does not apply if
(1) the abortion is performed or induced in a State that has, in force, a law requiring parental involvement in a minor’s abortion decision and the physician complies with the requirements of that law;
(2) the physician is presented with documentation showing with a reasonable degree of certainty that a court in the minor’s State of residence has waived any parental notification required by the laws of that State, or has otherwise authorized that the minor be allowed to procure an abortion;
(3) the minor declares in a signed written statement that she is the victim of sexual abuse, neglect, or physical abuse by a parent, and, before an abortion is performed on the minor, the physician notifies the authorities specified to receive reports of child abuse or neglect by the law of the State in which the minor resides of the known or suspected abuse or neglect;
(4) the abortion is necessary to save the life of the minor because her life was endangered by a physical disorder, physical injury, or physical illness, including a life endangering physical condition caused by or arising from the pregnancy itself, or because in the reasonable medical judgment of the minor’s attending physician, the delay in performing an abortion occasioned by fulfilling the prior notification requirement of subsection (a)(2) would cause a substantial and irreversible impairment of a major bodily function of the minor arising from continued pregnancy, not including psychological or emotional conditions, but an exception under this paragraph does not apply unless the attending physician or an agent of such physician, within 24 hours after completion of the abortion, notifies a parent in writing that an abortion was performed on the minor and of the circumstances that warranted invocation of this paragraph; or
(5) the minor is physically accompanied by a person who presents the physician or his agent with documentation showing with a reasonable degree of certainty that he or she is in fact the parent of that minor.
[535] “Opinion Number 90-19 of the Attorney General of New Mexico (Hal Stratton).” By Paul Farley (Assistant Attorney General). October 3, 1990. <www.justfacts.com>
Page 2: “New Mexico’s current criminal abortion statute, NMSA [New Mexico Statutes Annotated] 1978, §§ 30-5-1 to 30-5-3 (Supp.) 1990 was passed in 1969. … The statute further requires that any abortion either be performed only with the women’s consent or, if she is under eighteen years of age, then at the request of the minor and then her living parent or guardian.”
Page 4: “New Mexico’s criminal abortion law does not provide for such a bypass, as required by existing U.S. Supreme Court precedent.”
Page 7: “We further conclude that New Mexico’s parental consent provision may become enforceable either through legislative enactment of the amendments discussed above or, under certain circumstances, through modification of federal abortion jurisprudence.”
[536] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] II:
Jane Roe,4 a single woman who was residing in Dallas County, Texas, instituted this federal action in March 1970 against the District Attorney of the county. She sought a declaratory judgment that the Texas criminal abortion statutes were unconstitutional on their face, and an injunction restraining the defendant from enforcing the statutes.
Roe alleged that she was unmarried and pregnant; that she wished to terminate her pregnancy by an abortion “performed by a competent, licensed physician, under safe, clinical conditions”; that she was unable to get a “legal” abortion in Texas because her life did not appear to be threatened by the continuation of her pregnancy; and that she could not afford to travel to another jurisdiction in order to secure a legal abortion under safe conditions. …
4 The name is a pseudonym.
[537] Book: I Am Roe. By Norma McCorvey. Harper Collins, 1994.
NOTE: Norma McCorvey first made her identity public in the mid 1980s. Pages 172–173 contain information about her first appearance on television, but no date is given. However, the events in the book are chronologically arranged, and the context of the book indicates that this event took place sometime between 1984 and 1986.
[538] Article: “Henry Wade, Prosecutor in National Spotlight, Dies at 86.” By Wolfgang Saxon. New York Times, March 2, 2001. <www.nytimes.com>
“Henry Wade … is perhaps best remembered for the prosecution of Jack Ruby and as the Wade in Roe v. Wade….”
[539] Transcript: “Roe v. Wade—Oral Arguments before the United States Supreme Court.” December 13, 1971. <www.oyez.org>
Time marker 17:33:
Sarah R. Weddington
Your Honors, in the lower court, as I’m sure you’re aware, the court held that the right to determine whether or not to continue a pregnancy rested upon the Ninth Amendment which, of course, reserves those rights not specifically enumerated to the Government, to the people. …
I do feel that it is—that the Ninth Amendment is an appropriate place for the freedom to rest. I think the Fourteenth Amendment is equally an appropriate place, under the rights of persons to life, liberty, and the pursuit of happiness.
[540] Ninth Amendment to the Constitution of the United States. Ratified December 15, 1791. <justfacts.com>
“The enumeration in the Constitution, of certain rights, shall not be construed to deny or disparage others retained by the people.”
[541] Fourteenth Amendment to the Constitution of the United States. Ratified July 9, 1868. <justfacts.com>
Section 1. All persons born or naturalized in the United States, and subject to the jurisdiction thereof, are citizens of the United States and of the State wherein they reside. No State shall make or enforce any law which shall abridge the privileges or immunities of citizens of the United States; nor shall any State deprive any person of life, liberty, or property, without due process of law; nor deny to any person within its jurisdiction the equal protection of the laws.
[542] Transcript: “Roe v. Wade—Oral Arguments before the United States Supreme Court.” December 13, 1971. <www.oyez.org>
Time marker 18:49:
Sarah R. Weddington
I think the Fourteenth Amendment is equally an appropriate place, under the rights of persons to life, liberty, and the pursuit of happiness. I think that in as far as ‘liberty’ is meaningful, that liberty to these women would mean liberty from being forced to continue the unwanted pregnancy.
[543] Transcript: “Roe v. Wade—Oral Arguments before the United States Supreme Court.” October 11, 1972. <www.oyez.org>
Time marker 23:19:
Harry A. Blackmun
Well, do I get from this then that your case depends primarily on the proposition that the fetus has no constitutional rights?
Sarah R. Weddington
It depends on saying that the woman has a fundament constitutional right and that the state has not proved any compelling interest for regulation in the area. Even—even if the Court, at some point, determined the fetus to be entitled to constitutional protection, you would still get back into the weighing of one life against another.
[544] Transcript: “Roe v. Wade—Oral Arguments before the United States Supreme Court.” October 11, 1972. <www.oyez.org>
Time marker 24:15:
Potter Stewart
You certainly would because you’d have the same kind of thing you’d have to say that this would be the equivalent to after the child was born, if uh …
Sarah R. Weddington
That’s right.
Potter Stewart
If the mother thought that it bothered her health having the child around, she would, she could have it killed. Isn’t that correct?
[545] Transcript: “Roe v. Wade—Oral Arguments before the United States Supreme Court.” October 11, 1972. <www.oyez.org>
Time marker 24:28: “Sarah R. Weddington: That’s correct. That …”
[546] Transcript: “Roe v. Wade—Oral Arguments before the United States Supreme Court.” October 11, 1972. <www.oyez.org>
Time marker 24:30:
Warren E. Burger
Could Texas constitutionally—did you want to respond further to Justice Stewart? Did you want to respond further to him?
Sarah R. Weddington
No, your Honor.
[547] Transcript: “Roe v. Wade—Oral Arguments before the United States Supreme Court.” October 11, 1972. <www.oyez.org>
Time marker 24:30:
Warren E. Burger
Could Texas constitutionally—did you want to respond further to Justice Stewart? Did you want to respond further to him?
Sarah R. Weddington
No, your Honor.
[548] Transcript: “Roe v. Wade—Oral Arguments before the United States Supreme Court.” October 11, 1972. <www.oyez.org>
Time marker 28:32: “Robert C. Flowers: I understand, but the Fifth Amendment—I know the Fifth Amendment, no one shall be deprived of rights to life, liberty, and property without the due process of law.”
[549] Fifth Amendment to the Constitution of the United States. Ratified December 15, 1791. <justfacts.com>
No person shall be held to answer for a capital, or otherwise infamous crime, unless on a presentment or indictment of a Grand Jury, except in cases arising in the land or naval forces, or in the Militia, when in actual service in time of War or public danger; nor shall any person be subject for the same offence to be twice put in jeopardy of life or limb; nor shall be compelled in any criminal case to be a witness against himself, nor be deprived of life, liberty, or property, without due process of law; nor shall private property be taken for public use, without just compensation.
[550] Transcript: “Roe v. Wade—Oral Arguments before the United States Supreme Court.” October 11, 1972. <www.oyez.org>
Time marker 28:42: “Potter Stewart: Yes, but then the Fourteenth Amendment defines ‘person’ and it defines ‘person’ as somebody who is born, doesn’t it?”
[551] Fourteenth Amendment to the Constitution of the United States. Ratified July 9, 1868. <justfacts.com>
Section 1. All persons born or naturalized in the United States, and subject to the jurisdiction thereof, are citizens of the United States and of the State wherein they reside. No State shall make or enforce any law which shall abridge the privileges or immunities of citizens of the United States; nor shall any State deprive any person of life, liberty, or property, without due process of law; nor deny to any person within its jurisdiction the equal protection of the laws.
[552] Transcript: “Roe v. Wade—Oral Arguments before the United States Supreme Court.” October 11, 1972. <www.oyez.org>
Time marker 28:42:
Potter Stewart
Yes, but then the Fourteenth Amendment defines “person” and it defines “person” as somebody who is born, doesn’t it?
Robert C. Flowers
I’m not sure about that, Your Honor.
Potter Stewart
I know it does. Any person born or naturalized in the United States doesn’t—oh, that’s not a definition of a person, but that’s a definition of a citizen.
[553] Transcript: “Roe v. Wade—Oral Arguments before the United States Supreme Court.” October 11, 1972. <www.oyez.org>
Time marker 29:11:
Robert C. Flowers
Your Honor, it’s our position that the definition of a person is so basic. It’s so fundamental that it is—the framers of the constitution had not even set out to define. We can only go to what the teachings at the time that the constitution was framed. We have numerous listings in the brief by Mr. Joe Witherspoon, a professor at the University of Texas, that tries to trace back what was in their mind when they had the person concept when they drew up the constitution. He quoted Blackstone in 1765, and he observed in his commentaries that life, “this right is inherent by nature in every individual and exists even before the child is born.” I submit to you that the Declaration of Independence, we hold, is—
[554] Article: “Blackstone, Sir William.” New Millennium Encyclopedia. Simon & Shuster, 1999.
“British jurist and legal scholar, whose work Commentaries on the Laws of England was used for more than a century as the foundation of all legal education in Great Britain and the U.S.”
[555] Book: Commentaries on the Laws of England. By Sir William Blackstone. Edited by WM. Hardcastle Browne, 1892.
Preface:
Nearly a century and a half ago, the students of Oxford University listened to the lectures of Sir William Blackstone on the subject of English law; which literary and historical compilations were subsequently embodied in the four volumes of his commentaries. From that time to the present day, wherever the English language is spoken, these commentaries have been adopted by jurists, lawyers, students and literary men generally, as an epitome of the fundamental principles of our jurisprudence.
[556] Transcript: “Roe v. Wade—Oral Arguments before the United States Supreme Court.” October 11, 1972. <www.oyez.org>
Time marker 29:11:
Robert C. Flowers
Your Honor, it’s our position that the definition of a person is so basic. It’s so fundamental that it is—the framers of the constitution had not even set out to define. We can only go to what the teachings at the time that the constitution was framed. We have numerous listings in the brief by Mr. Joe Witherspoon, a professor at the University of Texas, that tries to trace back what was in their mind when they had the person concept when they drew up the constitution. He quoted Blackstone in 1765, and he observed in his commentaries that life, “this right is inherent by nature in every individual and exists even before the child is born.” I submit to you that the Declaration of Independence, we hold, is—
[557] Book: Commentaries on the Laws of England. By Sir William Blackstone. Edited by WM. Hardcastle Browne, 1892.
Page 40:
1 . Life. This right is inherent by nature in every individual, and exists even before the child is actually born.
Rights of Unborn Child. The offence of abortion of a quick child is not murder, but homicide or manslaughter. An infant in ventre sa mere [“in his mother’s womb”†] is supposed in law to be born for many purposes. It is capable of having a legacy made to it. It may have a guardian assigned to it, and may have an estate limited to its use, and to take afterwards by such limitation, as if it were then actually born. The same ruling holds in the civil law.
NOTE: † Bouvier’s Law Dictionary: A Concise Encyclopedia of the Law (Volume 2). By John Bouvier. Third Revision by Francis Rawle. Vernon Law Book Company, West Publishing Company, 1914. Page 1525: “In Ventre Sa Mere (L.[atin] F.[rench] In his mother’s womb.”
[558] Book: Commentaries on the Laws of England (3rd edition, 1st volume). By William Blackstone. Clarendon Press, 1768.
Page 129:
Life is the immediate gift of God, a right inherent by nature in every individual; and it begins in contemplation of law as soon as an infant is able to stir in the mother’s womb. For if a woman is quick with child, and by a potion, or otherwise, killeth it in her womb; or if any one beat her, whereby the child dieth in her body, and she is delivered of a dead child; this, though not murder, was by the antient [ancient] law homicide or manslaughter.o But Sir Edward Coke doth not look upon this offence in quite so atrocious a light, but merely as a heinous misdemesnor.P
An infant in ventre sa mere, or in the mother’s womb, is supposed in law to be born for many purposes. It is capable of having a legacy, or a surrender of a copyhold estate made to it. It may have a guardian assigned to itq; and it is enabled to have an estate limited to its use, and to take afterwards by such limitation, as if it were then actually born.r And in this point the civil law agrees with ours.s
[559] Transcript: “Roe v. Wade—Oral Arguments before the United States Supreme Court.” October 11, 1972. <www.oyez.org>
Time marker 29:11:
Robert C. Flowers
Your Honor, it’s our position that the definition of a person is so basic. It’s so fundamental that it is—the framers of the constitution had not even set out to define. … I submit to you that the Declaration of Independence, we hold, is—
Harry A. Blackmun
When you quote Blackstone, is it not true that in Blackstone’s time abortion was not a felony?
Robert C. Flowers
That’s true, Your Honor, but what my point there was to see the thinking of the framers of the constitution from the people they’ve learned from and the general attitude of the time.
[560] Declaration of Independence. Action of Second Continental Congress, July 4, 1776. <www.loc.gov>
“We hold these truths to be self-evident, that all men are created equal, that they are endowed by their Creator with certain unalienable Rights, that among these are Life, Liberty and the pursuit of Happiness.”
[561] Ruling: Gulf v. Ellis. U.S. Supreme Court, January 18, 1897. Decided 5–3. <caselaw.findlaw.com>
Majority:
The first official action of this nation declared the foundation of government in these words: “We hold these truths to be self-evident that all men are created equal, that they are endowed by their Creator with certain unalienable rights, that among these are life, liberty, and the pursuit of happiness.” While such declaration of principles may not have the force of organic law, or be made the basis of judicial decision as to the limits of right and duty, and while in all cases reference must be had to the organic law of the nation for such limits, yet the latter is but the body and the letter of which the former is the thought and the spirit, and it is always safe to read the letter of the constitution in the spirit of the Declaration of Independence. No duty rests more imperatively upon the courts than the enforcement of those constitutional provisions intended to secure that equality of rights which is the foundation of free government.
[562] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] I:
The Texas statutes that concern us here are Arts. 1191–1194 and 1196 of the State’s Penal Code.1 These make it a crime to “procure an abortion,” as therein [410 U.S. 113, 118] defined, or to attempt one, except with respect to “an abortion procured or attempted by medical advice for the purpose of saving the life of the mother.” Similar statutes are in existence in a majority of the States.2 [410 U.S. 113, 119] …
1 Article 1191. Abortion
If any person shall designedly administer to a pregnant woman or knowingly procure to be administered with her consent any drug or medicine, or shall use towards her any violence or means whatever externally or internally applied, and thereby procure an abortion, he shall be confined in the penitentiary not less than two nor more than five years; if it be done without her consent, the punishment shall be doubled. By “abortion” is meant that the life of the fetus or embryo shall be destroyed in the woman’s womb or that a premature birth thereof be caused.
Art. 1192. Furnishing the means
Whoever furnishes the means for procuring an abortion knowing the purpose intended is guilty as an accomplice.
Art. 1193. Attempt at abortion
If the means used shall fail to produce an abortion, the offender is nevertheless guilty of an attempt to produce abortion, provided [410 U.S. 113, 118] it be shown that such means were calculated to produce that result, and shall be fined not less than one hundred nor more than one thousand dollars.
Art. 1194. Murder in producing abortion
If the death of the mother is occasioned by an abortion so produced or by an attempt to effect the same it is murder.
Art. 1196. By medical advice
Nothing in this chapter applies to an abortion procured or attempted by medical advice for the purpose of saving the life of the mother.
The foregoing Articles, together with Art. 1195, compose Chapter 9 of Title 15 of the Penal Code. Article 1195, not attacked here, reads:
Art. 1195. Destroying unborn child
Whoever shall during parturition of the mother destroy the vitality or life in a child in a state of being born and before actual birth, which child would otherwise have been born alive, shall be confined in the penitentiary for life or for not less than five years.
2 Ariz. Rev. Stat. Ann. 13-211 (1956); Conn. Pub. Act No. 1 (May 1972 special session) (in 4 Conn. Leg. Serv. 677 (1972)), and Conn. Gen. Stat. Rev. 53-29, 53-30 (1968) (or unborn child); Idaho Code 18-601 (1948); Ill. Rev. Stat., c. 38, 23-1 (1971); Ind. Code 35-1-58-1 (1971); Iowa Code 701.1 (1971); Ky. Rev. Stat. 436.020 (1962); La. Rev. Stat. 37:1285 (6) (1964) (loss of medical license) (but see 14:87 (Supp. 1972) containing no exception for the life of the mother under the criminal statute); Me. Rev. Stat. Ann., Tit. 17, 51 (1964); Mass. Gen. Laws Ann., c. 272, 19 (1970) (using the term “unlawfully,” construed to exclude an abortion to save the mother’s life, Kudish v. Bd. of Registration, 356 Mass. 98, 248 N. E. 2d 264 (1969)); Mich. Comp. Laws 750.14 (1948); Minn. Stat. 617.18 (1971); Mo. Rev. Stat. 559.100 (1969); Mont. Rev. Codes Ann. 94-401 (1969); Neb. Rev. Stat. 28-405 (1964); Nev. Rev. Stat. 200.220 (1967); N. H. Rev. Stat. Ann. 585:13 (1955); N. J. Stat. Ann. 2A:87-1 (1969) (“without lawful justification”); N. D. Cent. Code 12-25-01, 12-25-02 (1960); Ohio Rev. Code Ann. 2901.16 (1953); Okla. Stat. Ann., Tit. 21, 861 (1972-1973 Supp.); Pa. Stat. Ann., Tit. 18, [410 U.S. 113, 119] 4718, 4719 (1963) (“unlawful”); R. I. Gen. Laws Ann. 11-3-1 (1969); S. D. Comp. Laws Ann. 22-17-1 (1967); Tenn. Code Ann. 39-301, 39-302 (1956); Utah Code Ann. 76-2-1, 76-2-2 (1953); Vt. Stat. Ann., Tit. 13, 101 (1958); W. Va. Code Ann. 61-2-8 (1966); Wis. Stat. 940.04 (1969); Wyo. Stat. Ann. 6-77, 6-78 (1957).
[563] Webpage: “Members of the Supreme Court of the United States.” U.S. Supreme Court. Accessed June 8, 2019 at <www.supremecourt.gov>
|
Name |
Appointed By |
Judicial Oath Taken |
Date Service Terminated |
Decision in Roe v. Wade |
|
Chief Justices |
||||
|
Burger, Warren Earl |
Nixon |
June 23, 1969 |
September 26, 1986 |
Concurrence |
|
Associate Justices |
||||
|
Douglas, William Orville |
Roosevelt, F. |
April 17, 1939 |
November 12, 1975 |
Concurrence |
|
Brennan, William J., Jr. |
Eisenhower |
October 16, 1956 |
July 20, 1990 |
Majority |
|
Stewart, Potter |
Eisenhower |
October 14, 1958 |
July 3, 1981 |
Concurrence |
|
White, Byron Raymond |
Kennedy |
April 16, 1962 |
June 28, 1993 |
Dissenting |
|
Marshall, Thurgood |
Johnson, L. |
October 2, 1967 |
October 1, 1991 |
Majority |
|
Blackmun, Harry A. |
Nixon |
June 9, 1970 |
August 3, 1994 |
Majority |
|
Powell, Lewis F., Jr. |
Nixon |
January 7, 1972 |
June 26, 1987 |
Majority |
|
Rehnquist, William H. |
Nixon |
January 7, 1972 |
September 3, 2005 |
Dissenting |
[564] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
3. State criminal abortion laws, like those involved here, that except from criminality only a life-saving procedure on the mother’s behalf without regard to the stage of her pregnancy and other interests involved violate the Due Process Clause of the Fourteenth Amendment, which protects against state action the right to privacy, including a woman’s qualified right to terminate her pregnancy. Though the State cannot override that right, it has legitimate interests in protecting both the pregnant woman’s health and the potentiality of human life, each of which interests grows and reaches a “compelling” point at various stages of the woman’s approach to term. Pp. 147–164. …
Mr. Justice Stewart, concurring. …
2 There is no constitutional right of privacy, as such. “[The Fourth] Amendment protects individual privacy against certain kinds of governmental intrusion, but its protections go further, and often have nothing to do with privacy at all. Other provisions of [410 U.S. 113, 168] the Constitution protect personal privacy from other forms of governmental invasion. But the protection of a person’s general right to privacy—his right to be let alone by other people—is, like the protection of his property and of his very life, left largely to the law of the individual States.” Katz v. United States, 389 U.S. 347, 350–351 (footnotes omitted).
[565] Fourteenth Amendment to the Constitution of the United States. Ratified July 9, 1868. <justfacts.com>
Section 1. All persons born or naturalized in the United States, and subject to the jurisdiction thereof, are citizens of the United States and of the State wherein they reside. No State shall make or enforce any law which shall abridge the privileges or immunities of citizens of the United States; nor shall any State deprive any person of life, liberty, or property, without due process of law; nor deny to any person within its jurisdiction the equal protection of the laws.
[566] Just Facts searched the 14th Amendment for all words in the entry: “privacy.” Collins English Thesaurus. Accessed September 7, 2018 at <www.collinsdictionary.com>
1. seclusion, isolation, solitude
You can try them on in the privacy of your own home.
seclusion They love the seclusion of their garden.
isolation the isolation he endured while he was in captivity
solitude Imagine long golden beaches where you can wander in solitude.
retirement retirement in the countryside
retreat He spent yesterday in his country retreat.
separateness
sequestration
privateness
2. secrecy, confidentiality, concealment
secrecy the secrecy of the confessional
confidentiality
concealment
clandestineness
[567] Fourteenth Amendment to the Constitution of the United States. Ratified July 9, 1868. <justfacts.com>
Section 1. All persons born or naturalized in the United States, and subject to the jurisdiction thereof, are citizens of the United States and of the State wherein they reside. No State shall make or enforce any law which shall abridge the privileges or immunities of citizens of the United States; nor shall any State deprive any person of life, liberty, or property, without due process of law; nor deny to any person within its jurisdiction the equal protection of the laws.
Section 2. Representatives shall be apportioned among the several States according to their respective numbers, counting the whole number of persons in each State, excluding Indians not taxed. But when the right to vote at any election for the choice of electors for President and Vice President of the United States, Representatives in Congress, the Executive and Judicial officers of a State, or the members of the Legislature thereof, is denied to any of the male inhabitants of such State, being twenty-one years of age,(See Note 15) and citizens of the United States, or in any way abridged, except for participation in rebellion, or other crime, the basis of representation therein shall be reduced in the proportion which the number of such male citizens shall bear to the whole number of male citizens twenty-one years of age in such State.
Section 3. No person shall be a Senator or Representative in Congress, or elector of President and Vice President, or hold any office, civil or military, under the United States, or under any State, who, having previously taken an oath, as a member of Congress, or as an officer of the United States, or as a member of any State legislature, or as an executive or judicial officer of any State, to support the Constitution of the United States, shall have engaged in insurrection or rebellion against the same, or given aid or comfort to the enemies thereof. But Congress may by a vote of two-thirds of each House, remove such disability.
Section 4. The validity of the public debt of the United States, authorized by law, including debts incurred for payment of pensions and bounties for services in suppressing insurrection or rebellion, shall not be questioned. But neither the United States nor any State shall assume or pay any debt or obligation incurred in aid of insurrection or rebellion against the United States, or any claim for the loss or emancipation of any slave; but all such debts, obligations and claims shall be held illegal and void.
Section 5. The Congress shall have power to enforce, by appropriate legislation, the provisions of this article.
[568] Book: The American Constitution: Its Origins and Development (3rd edition). By Alfred H. Kelly & Winfred A. Harbison. W. W. Norton & Company, 1963.
Page 454:
Well before the war ended, this block, which came to be known as Radicals or Radical Republicans, assumed a more positive role in opposing the reconstruction program and favoring more extreme measures. This group objected to Lincoln’s program on several counts. First, while the program implied the abolition of slavery, it guaranteed neither Negro suffrage nor Negro civil rights. Many Radicals were convinced that the Negro ought to be elevated forcibly to a position of civil, social and political equality with the whites.
Page 458:
By early January of 1866, the Radicals [Radical Republicans] were openly formulating their own program, and so preparing for a decisive conflict with the President [Andrew Johnson]. … A series of tentative Radical measures eventually led to the formulation of the Fourteenth Amendment to the Constitution, adopted by Congress in June 1866.
[569] Book: Processes of Constitutional Decision-Making: Cases and Materials (5th edition). By Paul Brest and others. Aspen Publishers, 2006.
Senator Jacob Howard, Speech Introducing the Fourteenth Amendment
Speech delivered in the U.S. Senate, May 23, 1866
[Senator Jacob Howard of Michigan was a member of the Joint Committee on Reconstruction that drafted the Fourteenth Amendment. He was the floor manager for the Amendment in the Senate. In this speech, he introduces the Amendment on the floor of the Senate and explains its purposes.]
I can only promise to present to the Senate, in a very succinct way, the views and the motives which influenced th[e] committee, so far as I understand those views and motives, in presenting the report which is now before us for consideration, and the ends it aims to accomplish. …
The first section [of the 14th Amendment] … relates to the privileges and immunities of citizens of the several States, and to the rights and privileges of all persons, whether citizens or others, under the laws of the United States. …
To these privileges and immunities, whatever they may be—for they are not and cannot be fully defined in their entire extent and precise nature—to these should be added the personal rights guarantied and secured by the first eight amendments of the Constitution; such as the freedom of speech and of the press; the right of the people peaceably to assemble and petition the Government for a redress of grievances, a right appertaining to each and all the people; the right to keep and to bear arms; the right to be exempted from the quartering of soldiers in a house without the consent of the owner; the right to be exempt from unreasonable searches and seizures, and from any search or seizure except by virtue of a warrant issued upon a formal oath or affidavit; the right of an accused person to be informed of the nature of the accusation against him, and his right to be tried by an impartial jury of the vicinage; and also the right to be secure against excessive bail and against cruel and unusual punishments.
Now, sir, here is a mass of privileges, immunities, and rights, some of them secured by the second section of the fourth article of the Constitution, which I have recited, some by the first eight amendments of the Constitution; and it is a fact well worthy of attention that the course of decision of our courts and the present settled doctrine is, that all these immunities, privileges, rights, thus guarantied by the Constitution or recognized by it, are secured to the citizen solely as a citizen of the United States and as a party in their courts. They do not operate in the slightest degree as a restraint or prohibition upon State legislation. States are not affected by them, and it has been repeatedly held that the restriction contained in the Constitution against the taking of private property for public use without just compensation is not a restriction upon State legislation, but applies only to the legislation of Congress.
Now, sir, there is no power given in the Constitution to enforce and to carry out any of these guarantees. They are not powers granted by the Constitution to Congress, and of course do not come within the sweeping clause of the Constitution authorizing Congress to pass all laws necessary and proper for carrying out the foregoing or granted powers, but they stand simply as a bill of rights in the Constitution, without power on the part of Congress to give them full effect; while at the same time the States are not restrained from violating the principles embraced in them except by their own local constitutions, which may be altered from year to year. The great object of the first section of this amendment is, therefore, to restrain the power of the States and compel them at all times to respect these great fundamental guarantees….
[570] 14th Amendment to the U.S. Constitution. Ratified July 9, 1868. <www.justfacts.com>
Section 1. All persons born or naturalized in the United States, and subject to the jurisdiction thereof, are citizens of the United States and of the State wherein they reside. No State shall make or enforce any law which shall abridge the privileges or immunities of citizens of the United States; nor shall any State deprive any person of life, liberty, or property, without due process of law; nor deny to any person within its jurisdiction the equal protection of the laws.
Section 2. Representatives shall be apportioned among the several States according to their respective numbers, counting the whole number of persons in each State, excluding Indians not taxed. But when the right to vote at any election for the choice of electors for President and Vice President of the United States, Representatives in Congress, the Executive and Judicial officers of a State, or the members of the Legislature thereof, is denied to any of the male inhabitants of such State, being twenty-one years of age, and citizens of the United States, or in any way abridged, except for participation in rebellion, or other crime, the basis of representation therein shall be reduced in the proportion which the number of such male citizens shall bear to the whole number of male citizens twenty-one years of age in such State.
Section 3. No person shall be a Senator or Representative in Congress, or elector of President and Vice President, or hold any office, civil or military, under the United States, or under any State, who, having previously taken an oath, as a member of Congress, or as an officer of the United States, or as a member of any State legislature, or as an executive or judicial officer of any State, to support the Constitution of the United States, shall have engaged in insurrection or rebellion against the same, or given aid or comfort to the enemies thereof. But Congress may by a vote of two-thirds of each House, remove such disability.
Section 4. The validity of the public debt of the United States, authorized by law, including debts incurred for payment of pensions and bounties for services in suppressing insurrection or rebellion, shall not be questioned. But neither the United States nor any State shall assume or pay any debt or obligation incurred in aid of insurrection or rebellion against the United States, or any claim for the loss or emancipation of any slave; but all such debts, obligations and claims shall be held illegal and void.
Section 5. The Congress shall have power to enforce, by appropriate legislation, the provisions of this article.
[571] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] IX: “We need not resolve the difficult question of when life begins. When those trained in the respective disciplines of medicine, philosophy, and theology are unable to arrive at any consensus, the judiciary, at this point in the development of man’s knowledge, is not in a position to speculate as to the answer.”
[Section] X: “In view of all this, we do not agree that, by adopting one theory of life, Texas may override the rights of the pregnant woman that are at stake.”
[Section] IX: “Texas urges that, apart from the Fourteenth Amendment, life begins at conception and is present throughout pregnancy….”
[572] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] IX: “Viability is usually placed at about seven months (28 weeks) but may occur earlier, even at 24 weeks.”
[Section] XI: “For the stage subsequent to viability, the State in promoting its interest in the potentiality of human life….”
NOTE: The terms “potential life” and “potentiality of life” are used throughout the ruling in reference to pre-birth humans at all stages of development.
[573] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] IX:
[T]he word “person,” as used in the Fourteenth Amendment, does not include the unborn.
NOTE: Section IX lists all places where the word “person” appears in the Constitution and its amendments and then states: “But in nearly all these instances, the use of the word is such that it has application only postnatally. None indicates, with any assurance, that it has any possible pre-natal application.”
[574] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] XI:
For the stage prior to approximately the end of the first trimester, the abortion decision and its effectuation must be left to the medical judgment of the pregnant woman’s attending physician. … The State may define the term “physician” to mean only a physician currently licensed by the State, and may proscribe any abortion by a person who is not a physician as so defined.
[575] Memorandum: “Re: No. 70-18—Roe v. Wade.” By Justice Harry A. Blackmun. Supreme Court of the United States, November 21, 1972. <www.justfacts.com>
Herewith is a memorandum (1972 fall edition) on the Texas abortion case.
This has proved for me to be both difficult and elusive. In its present form it contains dictum, but I suspect that in this area some dictum is indicated and not to be avoided.
You will observe that I have concluded that the end of the first trimester is critical. This is arbitrary, but perhaps any other selected point, such as quickening or viability, is equally arbitrary.
[576] Article: “The Abortion Papers.” By Bob Woodward. Washington Post, January 22, 1989. Page D1. <www.washingtonpost.com>
The opinion’s author, Justice Harry A. Blackmun, said in one internal court memo that he was drawing “arbitrary” lines about the times during pregnancy when a woman could legally receive an abortion. In another memo, Justice Potter Stewart, who joined the Blackmun opinion, said the determination in the opinion about these lines was “legislative.”
The Roe v. Wade memos were found among the personal papers of the late Justice William O. Douglas, which became available to the public at the Library of Congress last year.
[577] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] XI:
(a) For the stage prior to approximately the end of the first trimester, the abortion decision and its effectuation must be left to the medical judgment of the pregnant woman’s attending physician.
(b) For the stage subsequent to approximately the end of the first trimester, the State, in promoting its interest in the health of the mother, may, if it chooses, regulate the abortion procedure in ways that are reasonably related to maternal health.
(c) For the stage subsequent to viability, the State in promoting its interest in the potentiality of human life may, if it chooses, regulate, and even proscribe, abortion except where it is necessary, in appropriate medical judgment, for the preservation of the life or health of the mother.
[Section] X:
With respect to the State’s important and legitimate interest in the health of the mother, the “compelling” point, in the light of present medical knowledge, is at approximately the end of the first trimester. This is so because of the now-established medical fact, referred to above at 149, that until the end of the first trimester mortality in abortion may be less than mortality in normal childbirth. It follows that, from and after this point, a State may regulate the abortion procedure to the extent that the regulation reasonably relates to the preservation and protection of maternal health. Examples of permissible state regulation in this area are requirements as to the qualifications of the person who is to perform the abortion; as to the licensure of that person; as to the facility in which the procedure is to be performed, that is, whether it must be a hospital or may be a clinic or some other place of less-than-hospital status; as to the licensing of the facility; and the like.
[578] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.lp.findlaw.com>
Majority:
[Section] XI: “For the stage subsequent to viability the State, in promoting its interest in the potentiality of human life, may, if it chooses, regulate, and even proscribe, abortion except where necessary, in appropriate medical judgment, for the preservation of the life or health of the mother.”
[579] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] VIII:
Specific and direct harm medically diagnosable even in early pregnancy may be involved. Maternity, or additional offspring, may force upon the woman a distressful life and future. Psychological harm may be imminent. Mental and physical health may be taxed by child care. There is also the distress, for all concerned, associated with the unwanted child, and there is the problem of bringing a child into a family already unable, psychologically and otherwise, to care for it. In other cases, as in this one, the additional difficulties and continuing stigma of unwed motherhood may be involved. All these are factors the woman and her responsible physician necessarily will consider in consultation.
[580] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority: …
[Section] IV: “[T]he medical judgment may be exercised in the light of all factors—physical, emotional, psychological, familial, and the woman’s age—relevant to the wellbeing of the patient. All these factors may relate to health.”
[581] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] XI: “On the basis of elements such as these, appellant and some amici argue that the woman’s right is absolute and that she is entitled to terminate her pregnancy at whatever time, in whatever way, and for whatever reason she alone chooses. With this we do not agree.”
[582] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] VIII: “The privacy right … cannot be said to be absolute.”
[Section] VIII: “[M]ost of these courts have agreed that the right of privacy … is not absolute and is subject to some limitations; and that at some point the state interests as to protection of … prenatal life, become dominant. We agree with this approach.”
[Section] IX: “As we have intimated above, it is reasonable and appropriate for a State to decide that at some point in time … potential human life, becomes significantly involved. The woman’s privacy is no longer sole and any right of privacy she possesses must be measured accordingly.”
[Section] X: “We repeat, however, that the State does have an important and legitimate interest in … protecting the potentiality of human life.”
[583] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
[584] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] XI: “In Doe v. Bolton, post, p. 179, procedural requirements contained in one of the modern abortion statutes are considered. That opinion and this one, of course, are to be read together.”
[585] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist <supreme.justia.com>
Appendix A to Opinion of the Court
Criminal Code of Georgia
(The italicized portions are those held unconstitutional by the District Court)
Chapter 26-12. Abortion. …
26-1202. Exception. (a) Section 26-1201 shall not apply to an abortion performed by a physician duly licensed to practice medicine and surgery pursuant to Chapter 84-9 or 84-12 of the Code of Georgia of 1933, as amended, based upon his best clinical judgment that an abortion is necessary because:
(1) A continuation of the pregnancy would endanger the life of the pregnant woman or would seriously and permanently injure her health; or
(2) The fetus would very likely be born with a grave, permanent, and irremediable mental or physical defect; or
(3) The pregnancy resulted from forcible or statutory rape. …
(6) If the proposed abortion is considered necessary because the woman has been raped, the woman makes a written statement under oath, and subject to the penalties of false swearing, of the date, time and place of the rape and the name of the rapist, if known. There must be attached to this statement a certified copy of any report of the rape made by any law enforcement officer or agency and a statement by the solicitor general of the judicial circuit where the rape occurred or allegedly occurred that, according to his best information, there is probable cause to believe that the rape did occur. …
(c) Any solicitor General of the judicial circuit in which an abortion is to be performed under this section, or any person who would be a relative of the child within the second degree of consanguinity, may petition the superior court of the county in which the abortion is to be performed for a declaratory judgment whether the performance of such abortion would violate any constitutional or other legal rights of the fetus. Such solicitor General may also petition such court for the purpose of taking issue with compliance with the requirements of this section. The physician who proposes to perform the abortion and the pregnant woman shall be respondents. The petition shall be heard expeditiously, and if the court adjudges that such abortion would violate the constitutional or other legal rights of the fetus, the court shall so declare and shall restrain the physician from performing the abortion.
[586] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority: …
[Section] IV: “C. … We agree with the District Court…. [T]he medical judgment may be exercised in the light of all factors—physical, emotional, psychological, familial, and the woman’s age—relevant to the wellbeing of the patient. All these factors may relate to health.”
NOTE: Contrary to some commentaries on this case, these statements do not constitute a new ruling. This aspect of the law was not before the court in this instance. It was before the lower court and ruled upon, and the appeal was not accepted by the Supreme Court. In the quote above, the Supreme Court was simply restating their decision in Roe v. Wade. As Section II of Doe v. Bolton states: “The extent, therefore, to which the District Court decision was adverse to the defendants, that is, the extent to which portions of the Georgia statutes were held to be unconstitutional, technically is not now before us.”
[587] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] I:
[F]or an abortion to be authorized [410 U.S. 179, 184] or performed as a noncriminal procedure, additional conditions must be fulfilled. These are… (3) reduction to writing of the performing physician’s medical judgment that an abortion is justified for one or more of the reasons specified by 26-1202 (a), with written concurrence in that judgment by at least two other Georgia-licensed physicians, based upon their separate personal medical examinations of the woman … (5) advance approval by an abortion committee of not less than three members of the hospital’s staff….
[588] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority: …
[Section] II: “The [District] court, however, held that Georgia’s interest in protection of health, and the existence of a ‘potential of independent human existence’ … justified state regulation of ‘the manner of performance as well as the quality of the final decision to abort’ … and it refused to strike down the other provisions of the statutes.”
[Section] IV:
D. The appellants next argue that the District Court should have declared unconstitutional three procedural demands of the Georgia statute: (1) that the abortion be performed in a hospital accredited by the Joint Commission on Accreditation of Hospitals:11 (2) that the procedure be approved by the hospital staff abortion committee; and (3) that the performing physician’s judgment be confirmed by the independent examinations of the patient by two other licensed physicians. …
We hold that the JCAH-accreditation [Joint Commission on Accreditation of Hospitals] requirement does not withstand constitutional scrutiny in the present context. …
We conclude that the interposition of the hospital abortion committee is unduly restrictive of the patient’s rights and needs that, at this point, have already been medically delineated and substantiated by her personal physician. …
There remains, however, the required confirmation by two Georgia-licensed physicians in addition to the recommendation of the pregnant woman’s own consultant (making under the statute, a total of six physicians involved, including the three on the hospital’s abortion committee). We conclude that this provision, too, must fall.
The statute’s emphasis, as has been repetitively noted, is on the attending physician’s “best clinical judgment that an abortion is necessary.” That should be sufficient. The reasons for the presence of the confirmation step in the statute are perhaps apparent, but they are insufficient to withstand constitutional challenge. … If a physician is licensed by the State, he is recognized by the State as capable of exercising acceptable clinical judgment.
[589] Article: “Veto-Proof Majority in House Votes to Prohibit Late-Term Procedure.” By Diane M. Gianelli, American Medical News, November 20, 1995. <www.nrlc.org>
“Warren Hern, MD. The author of Abortion Practice, the nation’s most widely used textbook on abortion standards and procedures. Dr. Hern specializes in late-term procedures.”
[590] Webpage: “Biography: Warren M. Hern, M.D., M.P.H., Ph.D., Director.” Boulder Abortion Clinic, April 7, 2004. <www.drhern.com>
Page 2:
In 1976, Dr. Hern was one of the founding institutional members of the National Abortion Federation and served on its Board of Directors for four years. For the first two years of the organization’s existence, Dr. Hern served on the Standards Committee and then chaired that Committee for two years. He prepared for publication the first version of the National Abortion Federation Program Standards for Abortion Services, released in 1981.
Page 3: “During the controversy surrounding the so-called “Partial Birth Abortion” debate, Dr. Hern was one of the experts in late abortion sought out by the national media for comment on this political strategy.”
[591] Article: “Debate Might Be Less About Abortion Than Politicking.” By Mimi Hall. USA Today, May 15, 1997. Page 5A. <www.usatoday.com>
“ ‘I say every pregnancy carries a risk of death,’ says defiant physician Warren Hern of Boulder, Colo., who performs late-term abortions.”
[592] Article: “Daschle Bill May Not Ban Anything; Abortionists Could Use Own Judgment.” By Frank J. Murray. Washington Times, May 15, 1997. <www.washingtontimes.com>
… Dr. Warren Hern, who literally wrote the textbook on “Abortion Practice.”
The Denver gynecologist said the fact of occasional death in childbearing can justify any abortion, no matter how late it is done.
“I will certify that any pregnancy is a threat to a woman’s life and could cause ‘grievous injury’ to her ‘physical health,’ ” Dr. Hern said, using key words from the Daschle bill….
[593] Ruling: Planned Parenthood of Southeastern PA v. Casey. United States Supreme Court. June 29, 1992. <caselaw.findlaw.com>
Majority:
It must be stated at the outset and with clarity that Roe’s essential holding, the holding we reaffirm, has three parts. First is a recognition of the right of the woman to choose to have an abortion before viability and to obtain it without undue interference from the State. Before viability, the State’s interests are not strong enough to support a prohibition of abortion or the imposition of a substantial obstacle to the woman’s effective right to elect the procedure. Second is a confirmation of the State’s power to restrict abortions after fetal viability if the law contains exceptions for pregnancies which endanger the woman’s life or health. And third is the principle that the State has legitimate interests from the outset of the pregnancy in protecting the health of the woman and the life of the fetus that may become a child.
Roe established a trimester framework to govern abortion regulations. Under this elaborate but rigid construct, almost no regulation at all is permitted during the first trimester of pregnancy; regulations designed to protect the woman’s health, but not to further the State’s interest in potential life, are permitted during the second trimester; and, during the third trimester, when the fetus is viable, prohibitions are permitted provided the life or health of the mother is not at stake. …
We reject the trimester framework, which we do not consider to be part of the essential holding of Roe.
[594] Ruling: Planned Parenthood of Southeastern PA v. Casey. United States Supreme Court. June 29, 1992. <caselaw.findlaw.com>
Majority:
It must be stated at the outset and with clarity that Roe’s essential holding, the holding we reaffirm, has three parts. First is a recognition of the right of the woman to choose to have an abortion before viability and to obtain it without undue interference from the State. Before viability, the State’s interests are not strong enough to support a prohibition of abortion or the imposition of a substantial obstacle to the woman’s effective right to elect the procedure. Second is a confirmation of the State’s power to restrict abortions after fetal viability if the law contains exceptions for pregnancies which endanger the woman’s life or health. And third is the principle that the State has legitimate interests from the outset of the pregnancy in protecting the health of the woman and the life of the fetus that may become a child.
[595] Article: “Extreme Preemie, ‘About the Size of a Hand,’ Goes Home in Georgia.” FOX6 Milwaukee News, July 1, 2020. <www.fox6now.com>
Born at just 21 weeks old, Jemarius Harbor’s parents say the chances of him surviving were slim.
“He was about the size of a hand,” Jessica McPherson, Harbor’s mom said. “He had a lot of things that weren’t fully developed.” Harbor weighed 13 ounces when he was born back in December. …
For the past six months, Harbor’s parents have gone back and forth from their Jonesboro home to Emory Decatur Hospital. …
At nine pounds four ounces and about a month after his original due date in May, Harbor went home for the first time on Father’s Day.
[596] Article: “Extreme Preemie Born at 21 Weeks Young at Emory Decatur Hospital.” By George Franco. FOX 5 Atlanta News, December 26, 2019. <www.fox29.com>
Jemarius Jachin Harbor … emerged into the world at only 21 weeks young, weighing only 13 ounces, smaller than the size of a hand on Friday December 20. …
Gina Phillips, Director of Medical Services, with Pregnancy Aid Clinics, which helps at risk mothers said premature babies born at 23 weeks are considered the limit of viability.
“At 22 weeks some are surviving but 21 weeks is a very rarity it would be short of a miracle,” said Phillips.
She said the typical survival rate for a baby born at 21 weeks is less than four percent. …
She remains optimistic because in medicine and technology have improved survival chances of extreme preemie babies. “They did have a 21-week-old and four-day baby girl survived in Europe and without any complications, she’s several years old now,” said Phillips.
NOTE: “Gestation is the period of time between conception and birth. During this time, the baby grows and develops inside the mother’s womb. Gestational age is the common term used during pregnancy to describe how far along the pregnancy is. It is measured in weeks, from the first day of the woman’s last menstrual cycle to the current date.” [Webpage: “Gestational Age.” U.S. National Library of Medicine, National Institutes of Health. Last updated October 8, 2020. <medlineplus.gov>]
[597] Report: “Two-Year Neurodevelopmental Outcome of an Infant Born at 21 Weeks’ 4 Days’ Gestation.” By Kaashif A. Ahmad and others. Pediatrics, December 2017. <pediatrics.aappublications.org>
Page 1:
Recent literature confirms that, at the lower limit of extrauterine survival, substantial intercenter variability exists in resuscitation practice. The reasons for this variability are unclear, but may be related to disagreement on how to apply the best interests standard to extremely premature infants. Currently, both obstetric and pediatric societies recommend against assessing for viability or attempting resuscitation before 22 weeks’ gestation. In this context, we report the unimpaired 2-year outcome of a female infant resuscitated after delivery at 21 weeks’ 4 days’ gestation and 410 g birth weight. She may be the most premature known survivor to date.
Page 2: “We ascertained maturity by last menstrual period dating of 21 weeks 4 days, consistent with 9-week ultrasound dating of 21 weeks 2 days.”
NOTE: A “last menstrual period dating of 21 weeks 4 days” corresponds to 19 weeks and 4 days weeks after fertilization, or about 20 weeks. [Book: Color Atlas of Life Before Birth. By Marjorie A. England. Year Book Medical Publishers, 1983. Page 12: “Most clinicians do not know the fertilization date; the only date available to them is the first day of the last menstrual period. They use this date to define a menstrual age stretching from time 0, which is usually 14 days before fertilization….”]
[598] Ruling: Planned Parenthood of Southeastern PA v. Casey. United States Supreme Court. June 29, 1992. <caselaw.findlaw.com>
Majority:
[T]he State may take measures to ensure that the woman’s choice is informed, and measures designed to advance this interest will not be invalidated as long as their purpose is to persuade the woman to choose childbirth over abortion. These measures must not be an undue burden on the right.
As with any medical procedure, the State may enact regulations to further the health or safety of a woman seeking an abortion. Unnecessary health regulations that have the purpose or effect of presenting a substantial obstacle to a woman seeking an abortion impose an undue burden on the right. [505 U.S. 833, 879]
Our adoption of the undue burden analysis does not disturb the central holding of Roe v. Wade, and we reaffirm that holding. Regardless of whether exceptions are made for particular circumstances, a State may not prohibit any woman from making the ultimate decision to terminate her pregnancy before viability.
[599] Mississippi Code Title 41, Chapter 41, Section 41-41-191: “Gestational Age Act.” Accessed June 27, 2022 at <law.justia.com>
(b) Except in a medical emergency or in the case of a severe fetal abnormality, a person shall not intentionally or knowingly perform, induce, or attempt to perform or induce an abortion of an unborn human being if the probable gestational age of the unborn human being has been determined to be greater than fifteen (15) weeks.
[600] Ruling: Jackson Women’s Health Organization v. Dobbs. U.S. Court of Appeals for the Fifth Circuit, December 13, 2019. Decided 3–0. Majority: Higginbotham, Dennis, Ho. Concurring: Ho. <www.ca5.uscourts.gov>
Majority:
States may regulate abortion procedures prior to viability so long as they do not impose an undue burden on the woman’s right, but they may not ban abortions. The law at issue is a ban. Thus, we affirm the district court’s invalidation of the law, as well as its discovery rulings and its award of permanent injunctive relief.
Concurrence, James C. Ho:
Nothing in the text or original understanding of the Constitution establishes a right to an abortion. … Supreme Court precedent dictates abortion policy in America. So I am duty bound to affirm the judgment of the district court. But I cannot affirm the opinion of the district court.
[601] Report: “Dobbs v. Jackson Women’s Health.” U.S. Supreme Court, May 17, 2021. <www.supremecourt.gov>
Dobbs v. Jackson Women’s Health
Question Presented:
1. Whether all pre-viability prohibitions on elective abortions are unconstitutional.
2. Whether the validity of a pre-viability law that protects women’s health, the dignity of unborn children, and the integrity of the medical profession and society should be analyzed under Casey’s “undue burden” standard or Hellerstedt’s balancing of benefits and burdens.
3. Whether abortion providers have third-party standing to invalidate a law that protects women’s health from the dangers of late-term abortions.
Granted Limited to Question 1.
Cert. [Certiorari] Granted 5/17/2021
[602] Transcript: “Dobbs v. Jackson Women’s Health—Oral Arguments before the United States Supreme Court.” December 1, 2021. <www.supremecourt.gov>
Mr. Stewart …
First of all, I think the vast run of those cases—and some mentioned from time to time are things—you know, Griswold, Lawrence, Obergefell—these are—these are cases that draw clear rules: can‘t ban contraception, can’t ban intimate romantic relationships between consenting adults, can't ban marriage of people of the same sex, clear rules that have engendered strong reliance interests and that have not produced negative consequences or all the many other negative stare decisis considerations we pointed out, Your Honor.
Also, I—I'd add none of them involve the purposeful termination of a human life. So those two—those two features, stare decisis and termination of a human life, Your Honor, puts all of those safely out of reach if the Court overrules here.
[603] Transcript: “Dobbs v. Jackson Women’s Health—Oral Arguments before the United States Supreme Court.” December 1, 2021. <www.supremecourt.gov>
Mr. Stewart
… The viability line discounts and disregards state interests, and the undue burden standard has all—all of the problems that we’ve emphasized.
Justice Sotomayor
How is your interest anything but a religious view? The issue of when life begins has been hotly debated by philosophers since the beginning of time. It’s still debated in religions.
So, when you say this is the only right that takes away from the state the ability to protect a life, that’s a religious view, isn’t it?
[604] Entry: “life.” American Heritage Dictionary of Science. Houghton Mifflin, 1986.
Page 359: “the form of existence that organisms like animals and plants have and that inorganic objects or organic dead bodies lack; animate existence, characterized by growth, reproduction, metabolism, and response to stimuli.”
Pages ix–xi:
The expert help of the Editorial Committee [of Contributing Scientists] has enabled us to formulate definitions and explanations that correspond to recent findings of scientists working in their various disciplines. Precise editorial review in the offices of the publisher has contributed to a standard of excellence.
This is a dictionary of the basic terms of the physical and the biological sciences. …
The compiling of a specialized dictionary is, perhaps more than in most other reference books, the result of many scholars and editors working together. We are fortunate to have an outstanding group of active scientists, who read, commented upon and corrected the entire manuscript, and we are indented to them for their thorough work.
[605] Textbook: Essentials of Human Development: A Life-Span View (6th edition). By Robert Kail and John Cavanaugh. Cengage Learning, 2013.
Page 42:
Period of the Zygote (Weeks 1 and 2) …
Fertilization begins the period of the zygote, the technical term for the fertilized egg. This period ends when the zygote implants itself in the wall of the uterus (see Figure 2.4). During these two weeks, the zygote grows rapidly though cell division (see Figure 2.4). The zygote travels down the Fallopian tube toward the uterus and divides for the first time; it then continues to do so every 12 hours.
[606] Article: “Zygote.” Encyclopaedia Britannica. Accessed March 14, 2018 at <www.britannica.com>
“The joining of haploid gametes to produce a diploid zygote is a common feature in the sexual reproduction of all organisms except bacteria.”
[607] Paper: “The Marks, Mechanisms and Memory of Epigenetic States in Mammals.” By Vardhman K. Rakyan & others. Biochemical Journal, May 15, 2001. <portlandpress.com>
“Sexual reproduction in mammals results in the formation of a zygote, a single cell which contains all the necessary information to produce an entire organism comprised of billions of cells grouped into multitudinous cell types.”
[608] Book: Human Gametes and Preimplantation Embryos: Assessment and Diagnosis. Edited by David K. Gardner, Denny Sakkas, Emre Seli, and Dagan Wells. Springer, 2013.
Chapter 23: “Carbohydrate Analysis and Embryo Viability.” By Michelle Lane and David K. Gardner. Pages 259–266.
Page 260:
Concomitantly with the distinct changes in physiology that occur during development from the zygote to the blastocyst stage are dynamic changes in the metabolism of the embryo. At the zygote stage, the embryo is initially quiescent with a low metabolic and biosynthetic activity. At these early stages, the embryo predominantly uses the carboxylic acids pyruvate and lactate as its preferred energy substrates.14–16 Therefore, at these early stages of development the embryo is completely reliant on mitochondrial-based metabolism for ATP [Adenosine triphosphate] generation. However, the embryo does take up low levels of glucose,14, 15 which are likely metabolized by the pentose-phosphate pathway for the maintenance of reducing power in the cell particularly in the production of reduced glutathione for protection against oxidative stress. Furthermore, there is a recent understanding that the metabolism of glucose by the hexosamine biosynthesis pathway in the early embryo may be important in establishing O-linked glycosylation that is important for later stage development.17, 18 Therefore, it may be that this metabolism of glucose, although at a low level during the early stages of pre-implantation development, is essential for setting the subsequent metabolic program.
[609] Entry: “stimulus.” Oxford Dictionary of Biochemistry and Molecular Biology. Oxford University Press, 1997.
Page 619: “any event or phenomenon, such as radiation, electrical potential, or addition of molecules that leads to excitation of a tissue or cell.”
[610] Entry: “stimulus.” Collins English Dictionary (12th edition). HarperCollins, 2014.
“(Physiology) any drug, agent, electrical impulse, or other factor able to cause a response in an organism.”
[611] Paper: “The Role of PAF in Embryo Physiology.” By Chris O’Neill. Human Reproduction Update, May 2005. Pages 215–228. <humupd.oxfordjournals.org>
Page 215:
Embryo-derived paf [platelet-activating factor] … is produced by de novo synthesis. This synthesis commences soon after fertilization and persists throughout the preimplantation phase. … Paf also acts in an autocrine fashion as a trophic/survival factor for the early embryo. In vitro, supplementation of culture media with paf improves embryo development. …
Paf was the first mediator released by the preimplantation embryo to be identified (O’Neill, 1985a,b). It was subsequently shown that paf stimulated embryo metabolism (Ryan and others, 1989), cell-cycle progression (Roberts and others, 1993) and embryo viability (Spinks and O’Neill, 1988; Ryan and others, 1990b; Spinks and others, 1990) providing evidence for an autocrine loop in the early embryo. Insulin (Wales and others, 1985) also exerts trophic effects on the early embryo, the early embryo expresses a functional receptor for insulin (Harvey and Kaye, 1988; Heyner and others, 1989), but not insulin itself, suggesting that potential endocrine stimulation of embryo development also occurred. The possibility that a range of trophic factors may act on the early embryo was suggested by the detection of mRNA for a range of peptide growth factor ligands and their corresponding receptors (Rappolee and others, 1988). Since these observations, many putative autocrine, paracrine and endocrine factors have been implicated in supporting preimplantation embryo development (Kane and others, 1997; Kaye, 1997; Hardy and Spanos, 2002).
[612] Entry: “embryo.” Van Nostrand’s Scientific Encyclopedia. Edited by Douglas M. Considine. Springer, 2013.
Page 1142: “At the moment the sperm cell of the human male meets the ovum of the female and the union results in a fertilized ovum (zygote), a new life has begun.”
[613] Entry: “fertilization.” Encyclopedia & Dictionary of Medicine, Nursing & Allied Health (7th edition). Edited by Benjamin Frank Miller. W. B. Saunders, 2003.
“in human reproduction, the process by which the male’s sperm unites with the female’s oocyte, creating a new life.”
[614] Textbook: Before We Are Born: Essentials of Embryology and Birth Defects (5th edition). By Keith L. Moore & T.V.N. Persaud. W.B. Saunders Company, 1998.
Page 500: “The zygote and early embryo are living human organisms.”
[615] Textbook: The Developing Human: Clinically Oriented Embryology (7th edition). By Keith L. Moore & T. V. N. Persaud. Saunders, 2003.
Page 2: “Zygote. This cell results from the union of an oocyte and a sperm during fertilization. A zygote is the beginning of a new human being (i.e., an embryo).”
Page 33: “The zygote is genetically unique because half of its chromosomes come from the mother and half from the father. The zygote contains a new combination of chromosomes that is different from that in the cells of either of the parents. This mechanism forms the basis of biparental inheritance and variation of the human species.”
[616] Book: An Atlas of the Human Embryo and Fetus: A Photographic Review of Human Prenatal Development. By Jan E. Jirásek (MD, DSc, Laboratory of Reproductive Embryology, Institute for the Care of Mother and Child, Prague, Czech Republic). Parthenon Publishing Group, 2001.
Page 21: “A human being originates from two living cells: the oocyte (female germ cell) and the spermatozoon (male germ cell), transmitting the torch of life to the next generation.”
[617] Ruling: Dobbs v. Jackson Women’s Health Organization. U.S. Supreme Court, June 24, 2022. Decided 6–3. Majority: Alito, Thomas, Gorsuch, Kavanaugh, Barrett. Concurring: Thomas, Kavanaugh, Roberts. Dissenting: Breyer, Sotomayor, Kagan. <www.supremecourt.gov>
Majority: “We begin by considering the critical question whether the Constitution, properly understood, confers a right to obtain an abortion.”
[618] Ruling: Dobbs v. Jackson Women’s Health Organization. U.S. Supreme Court, June 24, 2022. Decided 6–3. Majority: Alito, Thomas, Gorsuch, Kavanaugh, Barrett. Concurring: Thomas, Kavanaugh, Roberts. Dissenting: Breyer, Sotomayor, Kagan. <www.supremecourt.gov>
Syllabus:
Held: The Constitution does not confer a right to abortion; Roe and Casey are overruled; and the authority to regulate abortion is returned to the people and their elected representatives.
ALITO, J., delivered the opinion of the Court, in which THOMAS, GORSUCH, KAVANAUGH, and BARRETT, JJ., joined. THOMAS, J., and KAVANAUGH, J., filed concurring opinions. ROBERTS, C. J., filed an opinion concurring in the judgment. BREYER, SOTOMAYOR, and KAGAN, JJ., filed a dissenting opinion.
Concurrence (Roberts):
The Court’s decision to overrule Roe and Casey is a serious jolt to the legal system—regardless of how you view those cases. A narrower decision rejecting the misguided viability line would be markedly less unsettling, and nothing more is needed to decide this case.
[619] Ruling: Dobbs v. Jackson Women’s Health Organization. U.S. Supreme Court, June 24, 2022. Decided 6–3. Majority: Alito, Thomas, Gorsuch, Kavanaugh, Barrett. Concurring: Thomas, Kavanaugh, Roberts. Dissenting: Breyer, Sotomayor, Kagan. <www.supremecourt.gov>
Majority:
Together, Roe and Casey represent an error that cannot be allowed to stand. …
We therefore hold that the Constitution does not confer a right to abortion. Roe and Casey must be overruled, and the authority to regulate abortion must be returned to the people and their elected representatives.
[620] Ruling: Dobbs v. Jackson Women’s Health Organization. U.S. Supreme Court, June 24, 2022. Decided 6–3. Majority: Alito, Thomas, Gorsuch, Kavanaugh, Barrett. Concurring: Thomas, Kavanaugh, Roberts. Dissenting: Breyer, Sotomayor, Kagan. <www.supremecourt.gov>
Majority:
The Constitution makes no express reference to a right to obtain an abortion, and therefore those who claim that it protects such a right must show that the right is somehow implicit in the constitutional text.
Roe, however, was remarkably loose in its treatment of the constitutional text. It held that the abortion right, which is not mentioned in the Constitution, is part of a right to privacy, which is also not mentioned.
[621] Ruling: Dobbs v. Jackson Women’s Health Organization. U.S. Supreme Court, June 24, 2022. Decided 6–3. Majority: Alito, Thomas, Gorsuch, Kavanaugh, Barrett. Concurring: Thomas, Kavanaugh, Roberts. Dissenting: Breyer, Sotomayor, Kagan. <www.supremecourt.gov>
Majority:
Roe was on a collision course with the Constitution from the day it was decided, Casey perpetuated its errors, and those errors do not concern some arcane corner of the law of little importance to the American people. Rather, wielding nothing but “raw judicial power,” … the Court usurped the power to address a question of profound moral and social importance that the Constitution unequivocally leaves for the people. Casey described itself as calling both sides of the national controversy to resolve their debate, but in doing so, Casey necessarily declared a winning side. Those on the losing side—those who sought to advance the State’s interest in fetal life—could no longer seek to persuade their elected representatives to adopt policies consistent with their views.
[622] Ruling: Dobbs v. Jackson Women’s Health Organization. U.S. Supreme Court, June 24, 2022. Decided 6–3. Majority: Alito, Thomas, Gorsuch, Kavanaugh, Barrett. Concurring: Thomas, Kavanaugh, Roberts. Dissenting: Breyer, Sotomayor, Kagan. <www.supremecourt.gov>
Majority: “The weaknesses in Roe’s reasoning are well-known. Without any grounding in the constitutional text, history, or precedent, it imposed on the entire country a detailed set of rules much like those that one might expect to find in a statute or regulation.”
[623] Ruling: Dobbs v. Jackson Women’s Health Organization. U.S. Supreme Court, June 24, 2022. Decided 6–3. Majority: Alito, Thomas, Gorsuch, Kavanaugh, Barrett. Concurring: Thomas, Kavanaugh, Roberts. Dissenting: Breyer, Sotomayor, Kagan. <www.supremecourt.gov>
Majority:
Due to the development of new equipment and improved practices, the viability line has changed over the years. In the 19th century, a fetus may not have been viable until the 32nd or 33rd week of pregnancy or even later.51 When Roe was decided, viability was gauged at roughly 28 weeks. … Today, respondents draw the line at 23 or 24 weeks. … So, according to Roe’s logic, States now have a compelling interest in protecting a fetus with a gestational age of, say, 26 weeks, but in 1973 States did not have an interest in protecting an identical fetus. How can that be?
Viability also depends on the “quality of the available medical facilities.” … Thus, a 24-week-old fetus may be viable if a woman gives birth in a city with hospitals that provide advanced care for very premature babies, but if the woman travels to a remote area far from any such hospital, the fetus may no longer be viable. On what ground could the constitutional status of a fetus depend on the pregnant woman’s location?
[624] Ruling: Dobbs v. Jackson Women’s Health Organization. U.S. Supreme Court, June 24, 2022. Decided 6–3. Majority: Alito, Thomas, Gorsuch, Kavanaugh, Barrett. Concurring: Thomas, Kavanaugh, Roberts. Dissenting: Breyer, Sotomayor, Kagan. <www.supremecourt.gov>
Majority:
Roe’s defenders characterize the abortion right as similar to the rights recognized in past decisions involving matters such as intimate sexual relations, contraception, and marriage, but abortion is fundamentally different, as both Roe and Casey acknowledged, because it destroys what those decisions called “fetal life” and what the law now before us describes as an “unborn human being.”13 …
What sharply distinguishes the abortion right from the rights recognized in the cases on which Roe and Casey rely is something that both those decisions acknowledged: Abortion destroys what those decisions call “potential life” and what the law at issue in this case regards as the life of an “unborn human being.” … None of the other decisions cited by Roe and Casey involved the critical moral question posed by abortion.
[625] Ruling: Dobbs v. Jackson Women’s Health Organization. U.S. Supreme Court, June 24, 2022. Decided 6–3. Majority: Alito, Thomas, Gorsuch, Kavanaugh, Barrett. Concurring: Thomas, Kavanaugh, Roberts. Dissenting: Breyer, Sotomayor, Kagan. <www.supremecourt.gov>
Majority: “These attempts to justify abortion through appeals to a broader right to autonomy and to define one’s “concept of existence” prove too much. … Those criteria, at a high level of generality, could license fundamental rights to illicit drug use, prostitution, and the like. … None of these rights has any claim to being deeply rooted in history.”
[626] Ruling: Dobbs v. Jackson Women’s Health Organization. U.S. Supreme Court, June 24, 2022. Decided 6–3. Majority: Alito, Thomas, Gorsuch, Kavanaugh, Barrett. Concurring: Thomas, Kavanaugh, Roberts. Dissenting: Breyer, Sotomayor, Kagan. <www.supremecourt.gov>
Majority:
Roe expressed the “feel[ing]” that the Fourteenth Amendment was the provision that did the work, but its message seemed to be that the abortion right could be found somewhere in the Constitution and that specifying its exact location was not of paramount importance.16 The Casey Court did not defend this unfocused analysis and instead grounded its decision solely on the theory that the right to obtain an abortion is part of the “liberty” protected by the Fourteenth Amendment’s Due Process Clause.
[627] Ruling: Dobbs v. Jackson Women’s Health Organization. U.S. Supreme Court, June 24, 2022. Decided 6–3. Majority: Alito, Thomas, Gorsuch, Kavanaugh, Barrett. Concurring: Thomas, Kavanaugh, Roberts. Dissenting: Breyer, Sotomayor, Kagan. <www.supremecourt.gov>
Majority:
The Constitution makes no reference to abortion, and no such right is implicitly protected by any constitutional provision, including the one on which the defenders of Roe and Casey now chiefly rely—the Due Process Clause of the Fourteenth Amendment. That provision has been held to guarantee some rights that are not mentioned in the Constitution, but any such right must be “deeply rooted in this Nation’s history and tradition” and “implicit in the concept of ordered liberty.” …
The right to abortion does not fall within this category.
[628] Ruling: Dobbs v. Jackson Women’s Health Organization. U.S. Supreme Court, June 24, 2022. Decided 6–3. Majority: Alito, Thomas, Gorsuch, Kavanaugh, Barrett. Concurring: Thomas, Kavanaugh, Roberts. Dissenting: Breyer, Sotomayor, Kagan. <www.supremecourt.gov>
Majority:
In this country during the 19th century, the vast majority of the States enacted statutes criminalizing abortion at all stages of pregnancy. See Appendix A…. By 1868, the year when the Fourteenth Amendment was ratified, three-quarters of the States, 28 out of 37, had enacted statutes making abortion a crime even if it was performed before quickening.34 … Of the nine States that had not yet criminalized abortion at all stages, all but one did so by 1910.
[629] Article: “14th Amendment to the U.S. Constitution: Civil Rights (1868).” National Archives. Last reviewed February 8, 2022. <www.archives.gov>
“On June 16, 1866, the House Joint Resolution proposing the 14th Amendment to the Constitution was submitted to the states. On July 28, 1868, the 14th amendment was declared, in a certificate of the Secretary of State, ratified by the necessary 28 of the 37 States, and became part of the supreme law of the land.”
[630] Ruling: Dobbs v. Jackson Women’s Health Organization. U.S. Supreme Court, June 24, 2022. Decided 6–3. Majority: Alito, Thomas, Gorsuch, Kavanaugh, Barrett. Concurring: Thomas, Kavanaugh, Roberts. Dissenting: Breyer, Sotomayor, Kagan. <www.supremecourt.gov>
Majority:
By the end of the 1950s, according to the Roe Court’s own count, statutes in all but four States and the District of Columbia prohibited abortion “however and whenever performed, unless done to save or preserve the life of the mother.” …
This overwhelming consensus endured until the day Roe was decided. At that time, also by the Roe Court’s own count, a substantial majority—30 States—still prohibited abortion at all stages except to save the life of the mother. … And though Roe discerned a “trend toward liberalization” in about “one-third of the States,” those States still criminalized some abortions and regulated them more stringently than Roe would allow.
[631] Ruling: Dobbs v. Jackson Women’s Health Organization. U.S. Supreme Court, June 24, 2022. Decided 6–3. Majority: Alito, Thomas, Gorsuch, Kavanaugh, Barrett. Concurring: Thomas, Kavanaugh, Roberts. Dissenting: Breyer, Sotomayor, Kagan. <www.supremecourt.gov>
Majority:
No Justice of this Court has ever argued that the Court should never overrule a constitutional decision, but overruling a precedent is a serious matter. It is not a step that should be taken lightly. Our cases have attempted to provide a framework for deciding when a precedent should be overruled, and they have identified factors that should be considered in making such a decision. …
In this case, five factors weigh strongly in favor of overruling Roe and Casey: the nature of their error, the quality of their reasoning, the “workability” of the rules they imposed on the country, their disruptive effect on other areas of the law, and the absence of concrete reliance. …
Roe was also egregiously wrong and deeply damaging. For reasons already explained, Roe’s constitutional analysis was far outside the bounds of any reasonable interpretation of the various constitutional provisions to which it vaguely pointed.
Roe was on a collision course with the Constitution from the day it was decided, Casey perpetuated its errors, and those errors do not concern some arcane corner of the law of little importance to the American people. …
[632] Webpage: “House Resolution 12: Women’s Health Protection Act of 2023.” U.S. House of Representatives, 118th Congress (2023–2024). Accessed October 3, 2023 at <www.congress.gov>
Ms. Chu … introduced the following bill; which was referred to the Committee on Energy and Commerce, and in addition to the Committee on the Judiciary, for a period to be subsequently determined by the Speaker, in each case for consideration of such provisions as fall within the jurisdiction of the committee concerned …
A Bill
To protect a person’s ability to determine whether to continue or end a pregnancy, and to protect a health care provider’s ability to provide abortion services.
[633] Webpage: “Senate Bill 701: Women’s Health Protection Act of 2023.” U.S. Senate, 118th Congress (2023–2024). Accessed October 3, 2023 at <www.congress.gov>
“Ms. Baldwin … introduced the following bill; which was read the first time … A Bill … To protect a person’s ability to determine whether to continue or end a pregnancy, and to protect a health care provider’s ability to provide abortion services.”
[634] Webpage: “House Resolution 12: Women’s Health Protection Act of 2023.” U.S. House of Representatives, 118th Congress (2023–2024). Accessed October 3, 2023 at <www.congress.gov>
(2) Post-Viability.—
(A) In General.—A health care provider has a right under this Act to provide abortion services and a patient has a corresponding right under this Act to terminate a pregnancy after viability when, in the good-faith medical judgement of the treating health care provider, it is necessary to protect the life or health of the patient. This subparagraph shall not otherwise apply after viability.
(B) Additional Circumstances.—A State may provide additional circumstances under which post viability abortions are permitted under this paragraph.
(C) Limitation.—In the case where a termination of a pregnancy after viability, in the good-faith medical judgement of the treating health care provider, is necessary to protect the life or health of the patient, a State shall not impose any of the limitations or requirements described in paragraph (1).
[635] Webpage: “Senate Bill 701: Women’s Health Protection Act of 2023.” U.S. Senate, 118th Congress (2023–2024). Accessed October 3, 2023 at <www.congress.gov>
(2) Post-Viability.—
(A) In General.—A health care provider has a right under this Act to provide abortion services and a patient has a corresponding right under this Act to terminate a pregnancy after viability when, in the good-faith medical judgement of the treating health care provider, it is necessary to protect the life or health of the patient. This subparagraph shall not otherwise apply after viability.
(B) Additional Circumstances.—A State may provide additional circumstances under which post viability abortions are permitted under this paragraph.
(C) Limitation.—In the case where a termination of a pregnancy after viability, in the good-faith medical judgement of the treating health care provider, is necessary to protect the life or health of the patient, a State shall not impose any of the limitations or requirements described in paragraph (1)
[636] Webpage: “House Resolution 12: Women’s Health Protection Act of 2023.” U.S. House of Representatives, 118th Congress (2023–2024). Accessed October 3, 2023 at <www.congress.gov>
(3) Health Care Provider.—The term “health care provider” means any entity (including any hospital, clinic, or pharmacy) or individual (including any physician, certified nurse-midwife, nurse practitioner, pharmacist, or physician assistant) that—
(A) is engaged or seeks to engage in the delivery of health care services, including abortion services; and
(B) if required by law or regulation to be licensed or certified to engage in the delivery of such services—
(i) is so licensed or certified; or
(ii) would be so licensed or certified but for their past, present, or potential provision of abortion services protected by section 4.
[637] Webpage: “Senate Bill 701: Women’s Health Protection Act of 2023.” U.S. Senate, 118th Congress (2023–2024). Accessed October 3, 2023 at <www.congress.gov>
(2) Post-Viability.—
(A) In General.—A health care provider has a right under this Act to provide abortion services and a patient has a corresponding right under this Act to terminate a pregnancy after viability when, in the good-faith medical judgement of the treating health care provider, it is necessary to protect the life or health of the patient. This subparagraph shall not otherwise apply after viability.
(B) Additional Circumstances.—A State may provide additional circumstances under which post viability abortions are permitted under this paragraph.
(C) Limitation.—In the case where a termination of a pregnancy after viability, in the good-faith medical judgement of the treating health care provider, is necessary to protect the life or health of the patient, a State shall not impose any of the limitations or requirements described in paragraph (1)
[638] Webpage: “House Resolution 12: Women’s Health Protection Act of 2023.” U.S. House of Representatives, 118th Congress (2023–2024). Accessed October 3, 2023 at <www.congress.gov>
The purposes of this Act are as follows:
(1) To permit people to seek and obtain abortion services, and to permit health care providers to provide abortion services, without harmful or unwarranted limitations or requirements that single out the provision of abortion services for restrictions that are more burdensome than those restrictions imposed on medically comparable procedures, do not significantly advance reproductive health or the safety of abortion services, or make abortion services more difficult to access. …
(4) To eliminate unwarranted burdens on commerce and the right to travel. Abortion bans and restrictions invariably affect commerce over which the United States has jurisdiction. Health care providers engage in economic and commercial activity when they provide abortion services. Moreover, there is an interstate market for abortion services and, in order to provide such services, health care providers engage in interstate commerce to purchase medicine, medical equipment, and other necessary goods and services; to obtain and provide training; and to employ and obtain commercial services from health care personnel, many of whom themselves engage in interstate commerce, including by traveling across State lines.
[639] Webpage: “Senate Bill 701: Women’s Health Protection Act of 2023.” U.S. Senate, 118th Congress (2023–2024). Accessed October 3, 2023 at <www.congress.gov>
The purposes of this Act are as follows:
(1) To permit people to seek and obtain abortion services, and to permit health care providers to provide abortion services, without harmful or unwarranted limitations or requirements that single out the provision of abortion services for restrictions that are more burdensome than those restrictions imposed on medically comparable procedures, do not significantly advance reproductive health or the safety of abortion services, or make abortion services more difficult to access. …
(4) To eliminate unwarranted burdens on commerce and the right to travel. Abortion bans and restrictions invariably affect commerce over which the United States has jurisdiction. Health care providers engage in economic and commercial activity when they provide abortion services. Moreover, there is an interstate market for abortion services and, in order to provide such services, health care providers engage in interstate commerce to purchase medicine, medical equipment, and other necessary goods and services; to obtain and provide training; and to employ and obtain commercial services from health care personnel, many of whom themselves engage in interstate commerce, including by traveling across State lines.
[640] Webpage: “House Resolution 3755: Women’s Health Protection Act of 2021.” U.S. House of Representatives, 117th Congress (2021–2022). Accessed October 4, 2023 at <www.congress.gov>
“(a) Findings.—Congress finds the following: … (9) Since 2011, States and local governments have passed nearly 500 restrictions singling out health care providers who offer abortion services, interfering with their ability to provide those services and the patients’ ability to obtain those services.”
[641] Webpage: “Senate Bill 1975: Women’s Health Protection Act of 2021.” U.S. Senate, 117th Congress (2021–2022). Accessed October 4, 2023 at <www.congress.gov>
“(a) Findings.—Congress finds the following: … (9) Since 2011, States and local governments have passed nearly 500 restrictions singling out health care providers who offer abortion services, interfering with their ability to provide those services and the patients’ ability to obtain those services.”
[642] Webpage: “Cosponsors: House Resolution 12 — Women’s Health Protection Act of 2023.” U.S. House of Representatives, 118th Congress (2023–2024). Accessed October 3, 2023 at <www.congress.gov>
“Cosponsor statistics: 212 current … Democratic [212]”
[643] Webpage: “Cosponsors: Senate Bill 701 — Women’s Health Protection Act of 2023.” U.S. Senate, 118th Congress (2023–2024). Accessed October 3, 2023 at <www.congress.gov>
“Cosponsor statistics: 48 current … Democratic [212] … Independent [3] … Sen. King, Angus S., Jr. [I-ME], Sen. Sanders, Bernard [I-VT], Sen. Sinema, Kyrsten [I-AZ]”
[644] Webpage: “Our Caucus.” Senate Democrats. Accessed October 5, 2023 at <www.democrats.senate.gov>
“Maine – Senator Angus King … Vermont – Senator Bernie Sanders … Arizona – Kyrsten Sinema”
[645] Webpage: “Senate Bill 4840: Protecting Pain-Capable Unborn Children from Late-Term Abortions Act.” U.S. Senate, 117th Congress (2021–2022). Accessed October 5, 2023 at <www.congress.gov>
Sponsor: Sen. Graham, Lindsey [R-SC] (Introduced 9/13/2022)
(a) Unlawful Conduct.—Subject to subsection (g) and notwithstanding any other provision of law, it shall be unlawful for any person to perform an abortion or attempt to do so, unless in conformity with the requirements set forth in subsection (b). …
(2) Prohibition on Performance of Certain Abortions.—
“(A) Generally for Unborn Children 15 Weeks or Older.—Except as provided in subparagraph (B), the abortion shall not be performed or attempted, if the probable gestational age, as determined under paragraph (1), of the unborn child is 15 weeks or greater.
“(B) Exceptions.—Subparagraph (A) does not apply if—
“(i) in reasonable medical judgment, the abortion is necessary to save the life of a pregnant woman whose life is endangered by a physical disorder, physical illness, or physical injury, including a life-endangering physical condition caused by or arising from the pregnancy itself, but not including psychological or emotional conditions;
“(ii) the pregnancy is the result of rape against an adult woman, and at least 48 hours prior to the abortion—
“(I) she has obtained counseling for the rape; or
“(II) she has obtained medical treatment for the rape or an injury related to the rape; or
“(iii) the pregnancy is a result of rape against a minor or incest against a minor, and the rape or incest has been reported at any time prior to the abortion to either—
“(I) a government agency legally authorized to act on reports of child abuse; or
“(II) a law enforcement agency. …
(c) Criminal Penalty.—Whoever violates subsection (a) shall be fined under this title or imprisoned for not more than 5 years, or both.
[646] Webpage: “Cosponsors: Senate Bill 4840 — Protecting Pain-Capable Unborn Children from Late-Term Abortions Act.” U.S. Senate, 117th Congress (2021–2022). Accessed October 5, 2023 at <www.congress.gov>
“Cosponsor statistics: 9 current … Republican [9]”
[647] House Resolution 962: “Born-Alive Abortion Survivors Protection Act.” U.S. House of Representatives, 116th Congress (2019–2020). Accessed July 6, 2019 at <www.congress.gov>
Sponsor: Rep. Wagner, Ann [R–MO–2] (Introduced 02/05/2019)
(a) Requirements for health care practitioners.—In the case of an abortion or attempted abortion that results in a child born alive:
(1) Degree of Care Required; Immediate Admission to a Hospital.—Any health care practitioner present at the time the child is born alive shall—
(A) exercise the same degree of professional skill, care, and diligence to preserve the life and health of the child as a reasonably diligent and conscientious health care practitioner would render to any other child born alive at the same gestational age; and
(B) following the exercise of skill, care, and diligence required under subparagraph (A), ensure that the child born alive is immediately transported and admitted to a hospital.
(2) Mandatory Reporting of Violations.—A health care practitioner or any employee of a hospital, a physician’s office, or an abortion clinic who has knowledge of a failure to comply with the requirements of paragraph (1) shall immediately report the failure to an appropriate State or Federal law enforcement agency, or to both.
(b) Penalties.—
(1) In General.—Whoever violates subsection (a) shall be fined under this title, imprisoned for not more than 5 years, or both.
(2) Intentional Killing of Child Born Alive.—Whoever intentionally performs or attempts to perform an overt act that kills a child born alive described under subsection (a), shall be punished as under section 1111 of this title for intentionally killing or attempting to kill a human being.
(c) Bar to prosecution.—The mother of a child born alive described under subsection (a) may not be prosecuted for a violation of this section, an attempt to violate this section, a conspiracy to violate this section, or an offense under section 3 or 4 of this title based on such a violation.
[648] Senate Bill 311: “Born-Alive Abortion Survivors Protection Act.” U.S. Senate, 116th Congress (2019–2020). Accessed July 6, 2019 at <www.congress.gov>
Sponsor: Sen. Sasse, Ben [R–NE] (Introduced 01/31/2019) …
(a) Requirements for health care practitioners.—In the case of an abortion or attempted abortion that results in a child born alive:
(1) Degree of Care Required; Immediate Admission to a Hospital.—Any health care practitioner present at the time the child is born alive shall—
(A) exercise the same degree of professional skill, care, and diligence to preserve the life and health of the child as a reasonably diligent and conscientious health care practitioner would render to any other child born alive at the same gestational age; and
(B) following the exercise of skill, care, and diligence required under subparagraph (A), ensure that the child born alive is immediately transported and admitted to a hospital.
(2) Mandatory Reporting of Violations.—A health care practitioner or any employee of a hospital, a physician’s office, or an abortion clinic who has knowledge of a failure to comply with the requirements of paragraph (1) shall immediately report the failure to an appropriate State or Federal law enforcement agency, or to both.
(b) Penalties.—
(1) In General.—Whoever violates subsection (a) shall be fined under this title, imprisoned for not more than 5 years, or both.
(2) Intentional Killing of Child Born Alive.—Whoever intentionally performs or attempts to perform an overt act that kills a child born alive described under subsection (a), shall be punished as under section 1111 of this title for intentionally killing or attempting to kill a human being.
(c) Bar to prosecution.—The mother of a child born alive described under subsection (a) may not be prosecuted for a violation of this section, an attempt to violate this section, a conspiracy to violate this section, or an offense under section 3 or 4 of this title based on such a violation.
[649] Calculated with data from vote 27: “Cloture on the Motion to Proceed: Born-Alive Abortion Survivors Protection Act.” U.S. Senate, February 25, 2019. <www.senate.gov>
Required For Majority: 3/5 … Vote Result: Cloture on the Motion to Proceed Rejected …
|
Party |
Voted “Yes” |
Voted “No” |
Voted “Present” or Did Not Vote † |
|||
|
Number |
Portion |
Number |
Portion |
Number |
Portion |
|
|
Republican |
50 |
94% |
0 |
0% |
3 |
6% |
|
Democrat |
3 |
7% |
42 |
93% |
0 |
0% |
|
Independent |
0 |
0% |
2 |
100% |
0 |
0% |
|
NOTE: † Voting “Present” is effectively the same as not voting. |
||||||
[650] Calculated with data from vote 29: “Born-Alive Abortion Survivors Protection Act.” U.S. House of Representatives, January 11, 2023. <clerk.house.gov>
|
Party |
Voted “Yes” |
Voted “No” |
Voted “Present” or Did Not Vote† |
|||
|
Number |
Portion |
Number |
Portion |
Number |
Portion |
|
|
Republican |
219 |
99% |
0 |
0% |
3 |
1% |
|
Democrat |
1 |
0.5% |
210 |
99% |
1 |
0.5% |
|
NOTE: †Voting “Present” is effectively the same as not voting. |
||||||
[651] Webpage: “Cosponsors of Senate Bill 204: Born-Alive Abortion Survivors Protection Act.” U.S. Senate, 118th Congress (2022–2023). Accessed October 5, 2023 at <www.congress.gov>
“Cosponsor statistics: 38 current … Republican [=] 38”
[652] Webpage: “Actions Overview: S.204 — Born-Alive Abortion Survivors Protection Act.” U.S. Senate, 118th Congress (2022–2022). Accessed October 5, 2023 at <www.congress.gov>
“02/01/2023 — Introduced in Senate”
[653] “2020 Democratic Party Platform.” Democratic National Committee, August 17, 2020. <www.presidency.ucsb.edu>
Democrats are committed to protecting and advancing reproductive health, rights, and justice. We believe unequivocally, like the majority of Americans, that every woman should be able to access high-quality reproductive health care services, including safe and legal abortion. We will repeal the Title X domestic gag rule and restore federal funding for Planned Parenthood, which provides vital preventive and reproductive health care for millions of people, especially low-income people, and people of color, and LGBTQ+ [lesbian, gay, bisexual, transgender, queer, etc.] people, including in underserved areas. …
We strongly and unequivocally support the decision to have a child, including by ensuring a safe and healthy pregnancy and childbirth, and by providing services during pregnancy and after the birth of a child, including adoption and social support services, as well as protections against pregnancy discrimination
[654] “Resolution Regarding the Republican Party Platform.” Republican National Committee, August 22, 2020. <www.presidency.ucsb.edu>
WHEREAS, The Republican National Committee (RNC) has significantly scaled back the size and scope of the 2020 Republican National Convention in Charlotte due to strict restrictions on gatherings and meetings, and out of concern for the safety of convention attendees and our hosts. …
RESOLVED, That the 2020 Republican National Convention will adjourn without adopting a new platform until the 2024 Republican National Convention.
[655] “2016 Republican Platform.” Republican National Convention, July 2016. <www.presidency.ucsb.edu>
The Constitution’s guarantee that no one can “be deprived of life, liberty or property” deliberately echoes the Declaration of Independence’s proclamation that “all” are “endowed by their Creator” with the inalienable right to life. Accordingly, we assert the sanctity of human life and affirm that the unborn child has a fundamental right to life which cannot be infringed. We support a human life amendment to the Constitution and legislation to make clear that the Fourteenth Amendment’s protections apply to children before birth.
We oppose the use of public funds to perform or promote abortion or to fund organizations, like Planned Parenthood, so long as they provide or refer for elective abortions or sell fetal body parts rather than provide healthcare. We urge all states and Congress to make it a crime to acquire, transfer, or sell fetal tissues from elective abortions for research, and we call on Congress to enact a ban on any sale of fetal body parts. In the meantime, we call on Congress to ban the practice of misleading women on so-called fetal harvesting consent forms, a fact revealed by a 2015 investigation. We will not fund or subsidize healthcare that includes abortion coverage.
We support the appointment of judges who respect traditional family values and the sanctity of innocent human life. We oppose the non-consensual withholding or withdrawal of care or treatment, including food and water, from individuals with disabilities, newborns, the elderly, or the infirm, just as we oppose euthanasia and assisted suicide.
We affirm our moral obligation to assist, rather than penalize, women who face an unplanned pregnancy. In order to encourage women who face an unplanned pregnancy to choose life, we support legislation that requires financial responsibility for the child be equally borne by both the mother and father upon conception until the child reaches adulthood. Failure to require a father to be equally responsible for a child places an inequitable burden on the mother, creating a financial and social hardship on both mother and child. We celebrate the millions of Americans who open their hearts, homes, and churches to mothers in need and women fleeing abuse. We thank and encourage providers of counseling, medical services, and adoption assistance for empowering women experiencing an unintended pregnancy to choose life. We support funding for ultrasounds and adoption assistance. We salute the many states that now protect women and girls through laws requiring informed consent, parental consent, waiting periods, and clinic regulation. We condemn the Supreme Court’s activist decision in Whole Woman’s Health v. Hellerstedt striking down commonsense Texas laws providing for basic health and safety standards in abortion clinics.
We applaud the U.S. House of Representatives for leading the effort to add enforcement to the Born-Alive Infant Protection Act by passing the Born-Alive Abortion Survivors Protection Act, which imposes appropriate civil and criminal penalties on healthcare providers who fail to provide treatment and care to an infant who survives an abortion, including early induction delivery whether the death of the infant is intended. We strongly oppose infanticide. Over a dozen states have passed Pain-Capable Unborn Child Protection Acts prohibiting abortion after twenty weeks, the point at which current medical research shows that unborn babies can feel excruciating pain during abortions, and we call on Congress to enact the federal version. Not only is it good legislation, but it enjoys the support of a majority of the American people. We support state and federal efforts against the cruelest forms of abortion, especially dismemberment abortion procedures, in which unborn babies are literally torn apart limb from limb.
We call on Congress to ban sex-selection abortions and abortions based on disabilities—discrimination in its most lethal form. We oppose embryonic stem cell research. We oppose federal funding of embryonic stem cell research. We support adult stem cell research and urge the restoration of the national placental stem cell bank created by President George H.W. Bush but abolished by his Democrat successor, President Bill Clinton. We oppose federal funding for harvesting embryos and call for a ban on human cloning.
The Democratic Party is extreme on abortion. Democrats’ almost limitless support for abortion, and their strident opposition to even the most basic restrictions on abortion, put them dramatically out of step with the American people. Because of their opposition to simple abortion clinic safety procedures, support for taxpayer-funded abortion, and rejection of pregnancy resource centers that provide abortion alternatives, the old Clinton mantra of “safe, legal, and rare” has been reduced to just “legal.” We are proud to be the party that protects human life and offers real solutions for women.
[656] 2022 Libertarian Party Platform”. Libertarian National Convention, May 2022. <www.lp.org>
[657] “2018 Libertarian Party Platform”. Libertarian National Convention, July 2018. <www.lp.org>
“Recognizing that abortion is a sensitive issue and that people can hold good-faith views on all sides, we believe that government should be kept out of the matter, leaving the question to each person for their conscientious consideration.”
NOTE: The 2020 convention made no changes to the platform.
[658] Webpage: “Green Party Platform”. Green Party National Convention, July 2020. Updated 9/2022. <www.gp.org>
Section II. Social Justice (<www.gp.org>):
F. Health Care
The Green Party supports single-payer universal health care and preventive care for all. …
The Green Party unequivocally supports a woman’s right to reproductive choice, no matter her marital status or age, and that contraception and safe, legal abortion procedures be available on demand and be included in all health insurance coverage in the U.S., as well as free of charge in any state where a woman’s income falls below the poverty level.
[659] Fourteenth Amendment to the Constitution of the United States. Ratified July 9, 1868. <justfacts.com>
Section 1. All persons born or naturalized in the United States, and subject to the jurisdiction thereof, are citizens of the United States and of the State wherein they reside. No State shall make or enforce any law which shall abridge the privileges or immunities of citizens of the United States; nor shall any State deprive any person of life, liberty, or property, without due process of law; nor deny to any person within its jurisdiction the equal protection of the laws.
[660] Search performed on September 20, 2023 at <www.congress.gov>. Just Facts searched bill texts from the 101st to 118th Congresses for: “amendment to the Constitution of the United States with respect to the right to life.” Sample result:
H. J. Res. 23
Proposing an amendment to the Constitution of the United States with respect to the right to life.
In the House of Representatives
January 4, 1995
Mr. Volkmer [Harold L. Volkmer (Democrat – Missouri)] introduced the following joint resolution; which was referred to the Committee on the Judiciary
Joint Resolution
Proposing an amendment to the Constitution of the United States with respect to the right to life.
Resolved by the Senate and House of Representatives of the United States of America in Congress assembled (two-thirds of each House concurring therein), That the following article is proposed as an amendment to the Constitution of the United States, which shall be valid to all intents and purposes as part of the Constitution when ratified by the legislatures of three-fourths of the several States:
Article—
Section 1. With respect to the right to life, the word “person” as used in this article and in the fifth and fourteenth articles of amendment to the Constitution of the United States applies to all human beings irrespective of age, health, function, or condition of dependency, including their unborn offspring at every state of their biological development.
Section 2. No unborn person shall be deprived of life by any person: Provided, however, That nothing in this article shall prohibit a law permitting only those medical procedures required to prevent the death of the mother.
Section 3. The Congress and the several States shall have the power to enforce this article by appropriate legislation.
Section 4. This article shall be inoperative unless it shall have been ratified as an amendment to the Constitution by the legislatures of three-fourths of the several States, within ten years of the date of its submission to the States by the Congress.
NOTE: A file containing the search results is available upon request.
[661] Search performed on September 20, 2023 at <www.congress.gov>. Just Facts searched bill texts from the 101st to 118th Congresses for: “amendment to the Constitution of the United States with respect to the right to life.” Sample result:
H. J. Res. 9
Proposing an amendment to the Constitution of the United States with respect to the right to life.
In the House of Representatives
January 7, 2003
Mrs. Emerson [Jo Ann Emerson (Republican – Missouri)] introduced the following joint resolution; which was referred to the Committee on the Judiciary
Joint Resolution
Proposing an amendment to the Constitution of the United States with respect to the right to life.
Resolved by the Senate and House of Representatives of the United States of America in Congress assembled (two-thirds of each House concurring therein), That the following article is proposed as an amendment to the Constitution of the United States, which shall be valid only when ratified by the legislatures of three-fourths of the several States within seven years after the date of final passage of this joint resolution:
Article—
Section 1. With respect to the right to life, the word “person” as used in this article and in the fifth and fourteenth articles of amendment applies to all human beings irrespective of age, health, function, or condition of dependency, including their unborn offspring at every state of their biological development.
Section 2. No unborn person shall be deprived of life by any person: Provided, however, That nothing in this article shall prohibit a law permitting only those medical procedures required to prevent the death of the mother of an unborn person: Provided further, That nothing in this article shall limit the liberty of a mother with respect to the unborn offspring of the mother conceived as a result of rape or incest.
Section 3. The Congress and the several States shall have power to enforce this article by appropriate legislation.
NOTE: A file containing the search results is available upon request.
[662] Press release: “National Right to Life Endorses President Trump for Re-Election.” National Right to Life Committee. July 4, 2019. <www.nrlc.org>
On the eve of its 49th annual convention, the National Right to Life Committee, the federation of state right-to-life affiliates and local chapters, today endorsed pro-life President Donald Trump for his re-election.
“As our nation celebrates Independence Day, we are proud to endorse the only presidential candidate who stands for the unalienable right to life,” said Carol Tobias, president of the National Right to Life Committee. “From his first day in office, President Trump and his Administration have been dedicated to advancing policies that protect the fundamental right to life for the unborn, the elderly, and the medically dependent and disabled.”
[663] Press release: “Joe Biden: ‘I Am the Democratic Party’–the Democratic Party Equals Abortion on Demand.” National Right to Life Committee. September 30, 2020. <www.nrlc.org>
During last night’s first presidential debate, Joe Biden declared that he was the Democratic Party:
My party is me. Right now, I am the Democratic Party. I am the Democratic Party, right now. The platform of the Democratic Party is what I, in fact, approved of.
“The Democratic Party and its leadership want abortion at any time, anywhere, and under any circumstances,” said Carol Tobias, president of National Right to Life. “In his own words, it means that Joe Biden wants abortion at any time, anywhere, and under any circumstances.”
[664] Article: “Reproductive Freedom for All.” Encyclopedia Britannica, September 20, 2023. <www.britannica.com>
“Reproductive Freedom for All, formerly (1969–73) National Association for the Repeal of Abortion Laws (NARAL), (1973–2003) National Abortion Rights Action League, and (2003–2023) NARAL Pro-Choice America, American organization, founded in 1969….”
[665] Press release: “NARAL Pro-Choice America Endorses Vice President Joe Biden for President.” NARAL Pro-Choice America, July 27, 2020. <www.prochoiceamerica.org>
NARAL Pro-Choice America today announced its endorsement of Vice President Joe Biden in his campaign for president of the United States.
“The choice is clear: In his four years in the White House, Donald Trump has exhibited unprecedented cruelty and put lives and freedom on the line time and time again—and this November, we have the opportunity to elect Vice President Joe Biden, a deeply compassionate and thoughtful leader who knows that fighting for reproductive freedom for every body is part and parcel of a just society,” said Ilyse Hogue, president of NARAL Pro-Choice America. “NARAL Pro-Choice America and our 2.5 million members are committed to powering Vice President Biden to victory this November and working with his administration to protect and expand access to abortion care and birth control. Joe Biden will stand for freedom over Donald Trump’s desire to control women. He will put a stop to Trump’s dangerous anti-choice political agenda when so much hangs in the balance. As we continue to face a public health crisis, a national reckoning with entrenched white supremacy, and attacks on reproductive freedom, another four years under Trump would be devastating—to our rights, our families, and our democracy. Vice President Biden will lead our nation forward with dignity and vision at a time when our freedoms are under unprecedented assault.”
Joe Biden has outlined his commitment to protecting and expanding reproductive freedom by vowing to work to safeguard Roe v. Wade, only appoint judges who will respect Roe, support the repeal of the racist and discriminatory Hyde Amendment, and use executive action to protect and expand access to abortion and contraception, including reversing Trump’s rules gutting reproductive freedom, like the global and domestic gag rules. These commitments are critical given the threat Donald Trump poses to our fundamental rights and everything our nation holds dear.
[666] Constitution of the United States. Signed September 17, 1787. Enacted June 21, 1788. <www.justfacts.com>
Article 2, Section 2, Clause 2: “[The President] with the Advice and Consent of the Senate, shall appoint Ambassadors, other public Ministers and Consuls, Judges of the supreme Court….”
[667] Constitution of the United States. Signed September 17, 1787. Enacted June 21, 1788. <www.justfacts.com>
Article III, Section 1: “The Judges, both of the supreme and inferior Courts, shall hold their Offices during good Behaviour….”
Article II, Section 4: “The President, Vice President and all civil Officers of the United States, shall be removed from Office on Impeachment for, and Conviction of, Treason, Bribery, or other high Crimes and Misdemeanors.”
Article I, Section 2, Clause 5: “The House of Representatives shall chuse their Speaker and other Officers; and shall have the sole Power of Impeachment.”
Article I, Section 3, Clause 6: “The Senate shall have the sole Power to try all Impeachments. … And no Person shall be convicted without the Concurrence of two thirds of the Members present.”
[668] Letter: “Dear Delawarean.” By Joseph R. Biden, Jr. U.S. Senate, December 26, 1977. <www.documentcloud.org>
Since the Congress has again taken up the question of federal funding for abortions, I thought you would be interested in a summary of these recent actions.
As you probably already know, the Senate and the House of Representatives finally agreed on language dealing with the problem of Medicaid-covered abortions December 15. The 1977 fiscal year appropriations bill prohibited the use of federal funds to pay for abortions, “… unless the life of the mother is in danger.” This is the position which I have consistently supported.
During consideration of the 1978 fiscal year appropriation bill for the Department of Health, Education and Welfare, the House again passed this same language. The Senate, however, passed a broader definition of the circumstances under which medicaid funds could be used to pay for an abortion. I did not support this version.
The language that the Senate and House finally agreed to (after five months of debate] will protect both the woman and her unborn child. The agreement prohibits the use of any funds in the bill to pay for abortions unless continued pregnancy would endanger the mother’s life, or in the opinion of two doctors, cause “severe and long lasting physical health damage.”
[669] Article: “Joe Biden’s Long Evolution on Abortion Rights Still Holds Surprises.” By Heidi Przybyla. NBC News, June 5, 2019. <www.nbcnews.com>
As a U.S. senator from Delaware, Biden voted against a 1977 compromise that allowed Medicaid to fund abortions that included exceptions for victims of rape and incest in addition to concerns for the life of the mother. While the rape and incest exceptions passed in that case, Biden voted in 1981 to again remove them, in what was the most far-reaching ban on federal funds ever enacted by Congress.
Biden also voted several times, including in 1983, to prohibit federal workers from using health insurance on abortion services, with the only exception being to save the life of the mother. …
In a 1994 letter to constituents—written during negotiations over health care during the Clinton administration—Biden noted he had “on no fewer than 50 occasions” voted against federal funding for abortions. “Those of us who are opposed to abortions should not be compelled to pay for them,” Biden wrote on April 7, 1994.
[670] Article: “Joe Biden Denounces Hyde Amendment, Reversing His Position.” By Katie Glueck. New York Times, June 6, 2019. <www.nytimes.com>
After two days of intense criticism, Joseph R. Biden Jr. reversed himself Thursday night on one of the issues most important to Democratic voters, saying he no longer supports a measure that bans federal funding for most abortions.
As recently as Wednesday, Mr. Biden’s campaign had said he supported the measure, known as the Hyde Amendment. His decision to change positions illustrates the intense pressure he faces as the presumed front-runner for the Democratic nomination for president. …
“If I believe health care is a right, as I do, I can no longer support an amendment that makes that right dependent on someone’s ZIP code,” Mr. Biden said.
[671] Video: “Planned Parenthood Action Fund: 2020 Election Membership Forum.” June 22, 2019. <www.youtube.com>
Time marker 2:36:56:
Kelley Robinson
I think that it’s true right, that you’ve stated yourself that you’ve evolved on some issues including those related to sexual and reproductive healthcare. One of the most recent was a couple of weeks ago when you came out as a champion for women’s health when you spoke out against the Hyde amendment which we all know disproportionately impacts and discriminates against low-income people who need abortion care. So my question for you is: As president, how would you put forward a federal budget that eliminates Hyde?
Joe Biden
Well first of all, the way I’d do that is—let me explain what happened. I laid out a healthcare plan that is going to provide federally funded healthcare for all women and women who now are denied even Medicare in their home states, across the board you’d be automatically sign up under the Obamacare light provision we have because I provide for a Medicaid and Medicare type policy that is in fact going to provide all the same services. So, it became really clear to me that although the Hyde amendment was designed to try to split the difference here to make sure women still had access, you can’t have access if in fact everyone is covered by a federal policy. And so that’s why I at the same time I announced that policy, I announced that I can no longer continue to abide by the Hyde amendment. That’s the reason.
[672] Letter from U.S. Senator Joseph R. Biden, Jr. to Mr. Michael Gregg, April 7, 1994. <www.documentcloud.org>
Thank you for your postcard on health care reform and abortion services. You say in your postcard that most Americans don’t want to pay for abortion services and ask, “Please don’t force me to pay for abortions against my conscience.” I agree with you.
At this time, with a number of health care reform proposals on the table and a long debate ahead, there is no way to know the form that the final legislation will take, or what amendments may be offered. However, I will continue to abide by the same principle that has guided me throughout my 21 years in the Senate: those of us who are opposed to abortion should not be compelled to pay for them. As you may know, I have consistently—on no fewer than 50 occasions—voted against federal funding of abortions.
The present debate over health care reform raises for the first time the question of whether the federal government should decide for everyone that they must buy insurance that includes abortion services, or whether individuals should have the option not to. Just as the federal government should not be business of telling people that they can no longer use their own money to purchase such services, the government should not tell those with strong convictions against abortion, such as you and I, that we must pay for them.
[673] Twitter post: “Our Volunteer Nina Asked Joe Biden Whether, as President, He Would Lift the Hyde Amendment, Which Bans Federal Insurance Coverage of Abortion.” ACLU [American Civil Liberties Union], May 8, 2019. <twitter.com>
Our volunteer Nina asked Joe Biden whether, as president, he would lift the Hyde amendment, which bans federal insurance coverage of abortion.
He said yes. #RightsForAll
ACLU volunteer Nina: I’m an ACLU rights for all voter and I have one quick question for you, and that is: will you commit to abolishing the Hyde amendment which hurts poor women and, and …
Joe Biden: Yes.
ACLU volunteer Nina: … women of color.
Joe Biden: Yes, and by the way, ACLU member, I got a near perfect voting record my entire career.
ACLU volunteer Nina: I heard you did. But I’m glad you just said you would commit to abolishing the Hyde amendment.
Joe Biden: No, no. Right now it has to be—it can’t stay.
ACLU volunteer Nina: Thank you. Thank you sir.
[674] Article: “Joe Biden’s Long Evolution on Abortion Rights Still Holds Surprises.” By Heidi Przybyla. NBC News, June 5, 2019. <www.nbcnews.com>
“Yet his presidential campaign confirmed to NBC News that Biden still supports the Hyde Amendment, a four-decade-old ban on using federal funds for abortion services, except in cases of rape, incest or to save the life of the woman.”
[675] Article: “Biden Still Backs Hyde Amendment, Which Bans Federal Funds for Abortions.” By Katie Glueck. New York Times, June 5, 2019. <www.nytimes.com>
Former Vice President Joseph R. Biden Jr., who has shunned today’s Democratic Party orthodoxy on issues from crime to compromising with Republicans, again broke with his party’s base and many of his campaign rivals on Wednesday when his campaign confirmed that he still backs the Hyde Amendment, a measure that prohibits the use of federal funds for abortion with exceptions for cases involving rape, incest and when the life of the mother is in danger.
[676] Article: “Joe Biden Denounces Hyde Amendment, Reversing His Position.” By Katie Glueck. New York Times, June 6, 2019. <www.nytimes.com>
After two days of intense criticism, Joseph R. Biden Jr. reversed himself Thursday night on one of the issues most important to Democratic voters, saying he no longer supports a measure that bans federal funding for most abortions.
As recently as Wednesday, Mr. Biden’s campaign had said he supported the measure, known as the Hyde Amendment. His decision to change positions illustrates the intense pressure he faces as the presumed front-runner for the Democratic nomination for president. …
“If I believe health care is a right, as I do, I can no longer support an amendment that makes that right dependent on someone’s ZIP code,” Mr. Biden said.
[677] Video: “Planned Parenthood Action Fund: 2020 Election Membership Forum.” June 22, 2019. <www.youtube.com>
Time marker 2:36:56:
Kelley Robinson
I think that it’s true right, that you’ve stated yourself that you’ve evolved on some issues including those related to sexual and reproductive healthcare. One of the most recent was a couple of weeks ago when you came out as a champion for women’s health when you spoke out against the Hyde amendment which we all know disproportionately impacts and discriminates against low-income people who need abortion care. So my question for you is: As president, how would you put forward a federal budget that eliminates Hyde?
Joe Biden
Well first of all, the way I’d do that is—let me explain what happened. I laid out a healthcare plan that is going to provide federally funded healthcare for all women and women who now are denied even Medicare in their home states, across the board you’d be automatically sign up under the Obamacare light provision we have because I provide for a Medicaid and Medicare type policy that is in fact going to provide all the same services. So, it became really clear to me that although the Hyde amendment was designed to try to split the difference here to make sure women still had access, you can’t have access if in fact everyone is covered by a federal policy. And so that’s why I at the same time I announced that policy, I announced that I can no longer continue to abide by the Hyde amendment. That’s the reason.
[678] Webpage: “The Biden Agenda for Women.” Biden For President. Accessed August 29, 2020 at <bit.ly>
“Stop state laws violating Roe v. Wade. Biden will work to codify Roe v. Wade, and his Justice Department will do everything in its power to stop the rash of state laws that so blatantly violate Roe v. Wade.”
[679] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] VIII:
Specific and direct harm medically diagnosable even in early pregnancy may be involved. Maternity, or additional offspring, may force upon the woman a distressful life and future. Psychological harm may be imminent. Mental and physical health may be taxed by child care. There is also the distress, for all concerned, associated with the unwanted child, and there is the problem of bringing a child into a family already unable, psychologically and otherwise, to care for it. In other cases, as in this one, the additional difficulties and continuing stigma of unwed motherhood may be involved. All these are factors the woman and her responsible physician necessarily will consider in consultation.
[Section] XI:
For the stage subsequent to viability the State, in promoting its interest in the potentiality of human life, may, if it chooses, regulate, and even proscribe, abortion except where necessary, in appropriate medical judgment, for the preservation of the life or health of the mother. …
In Doe v. Bolton, post, p. 179, procedural requirements contained in one of the modern abortion statutes are considered. That opinion and this one, of course, are to be read together.
[680] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority: …
[Section] IV: “[T]he medical judgment may be exercised in the light of all factors—physical, emotional, psychological, familial, and the woman’s age—relevant to the wellbeing of the patient. All these factors may relate to health.”
[681] Ruling: Planned Parenthood of Southeastern PA v. Casey. United States Supreme Court. June 29, 1992. <caselaw.findlaw.com>
Majority:
It must be stated at the outset and with clarity that Roe’s essential holding, the holding we reaffirm, has three parts. First is a recognition of the right of the woman to choose to have an abortion before viability and to obtain it without undue interference from the State. Before viability, the State’s interests are not strong enough to support a prohibition of abortion or the imposition of a substantial obstacle to the woman’s effective right to elect the procedure. Second is a confirmation of the State’s power to restrict abortions after fetal viability if the law contains exceptions for pregnancies which endanger the woman’s life or health. And third is the principle that the State has legitimate interests from the outset of the pregnancy in protecting the health of the woman and the life of the fetus that may become a child.
[682] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority: …
[Section] IV: …
D. The appellants next argue that the District Court should have declared unconstitutional three procedural demands of the Georgia statute: (1) that the abortion be performed in a hospital accredited by the Joint Commission on Accreditation of Hospitals:11 (2) that the procedure be approved by the hospital staff abortion committee; and (3) that the performing physician’s judgment be confirmed by the independent examinations of the patient by two other licensed physicians. …
We hold that the JCAH-accreditation [Joint Commission on Accreditation of Hospitals] requirement does not withstand constitutional scrutiny in the present context. …
We conclude that the interposition of the hospital abortion committee is unduly restrictive of the patient’s rights and needs that, at this point, have already been medically delineated and substantiated by her personal physician. …
There remains, however, the required confirmation by two Georgia-licensed physicians in addition to the recommendation of the pregnant woman’s own consultant (making under the statute, a total of six physicians involved, including the three on the hospital’s abortion committee). We conclude that this provision, too, must fall.
The statute’s emphasis, as has been repetitively noted, is on the attending physician’s “best clinical judgment that an abortion is necessary.” That should be sufficient. The reasons for the presence of the confirmation step in the statute are perhaps apparent, but they are insufficient to withstand constitutional challenge. … If a physician is licensed by the State, he is recognized by the State as capable of exercising acceptable clinical judgment.
[683] Article: “Daschle Bill May Not Ban Anything; Abortionists Could Use Own Judgment.” By Frank J. Murray. Washington Times, May 15, 1997. <www.washingtontimes.com>
… Dr. Warren Hern, who literally wrote the textbook on “Abortion Practice.”
The Denver gynecologist said the fact of occasional death in childbearing can justify any abortion, no matter how late it is done.
“I will certify that any pregnancy is a threat to a woman’s life and could cause ‘grievous injury’ to her ‘physical health,’ ” Dr. Hern said, using key words from the Daschle bill….
[684] Webpage: “Health Care.” Biden For President. Accessed October 7, 2020 at <bit.ly>
“As president, Biden will work to codify Roe v. Wade, and his Justice Department will do everything in its power to stop the rash of state laws that so blatantly violate the constitutional right to an abortion, such as so-called TRAP [targeted restrictions on abortion] laws, parental notification requirements, mandatory waiting periods, and ultrasound requirements.”
[685] Vote 263: “Motion to Invoke Cloture on the Motion to Concur in House Amendment to S.403.” U.S. Senate, September 29, 2006. <www.senate.gov>
“Biden (D-DE), Nay”
[686] House of Representatives Amendment to Senate Bill 403: “Child Interstate Abortion Notification Act.” 109th Congress (2005–2006), September 26, 2006. <www.congress.gov>
Sec. 2431. Transportation of Minors in Circumvention of Certain Laws Relating to Abortion
(a) Offense—
(1) Generally—Except as provided in subsection (b), whoever knowingly transports a minor across a State line, with the intent that such minor obtain an abortion, and thereby in fact abridges the right of a parent under a law requiring parental involvement in a minor’s abortion decision, in force in the State where the minor resides, shall be fined under this title or imprisoned not more than one year, or both.
(b) Exceptions—
(1) The prohibition of subsection (a) does not apply if the abortion was necessary to save the life of the minor because her life was endangered by a physical disorder, physical injury, or physical illness, including a life endangering physical condition caused by or arising from the pregnancy itself.
(2) A minor transported in violation of this section, and any parent of that minor, may not be prosecuted or sued for a violation of this section, a conspiracy to violate this section, or an offense under section 2 or 3 based on a violation of this section. …
Sec. 2435. Child Interstate Abortion Notification
(a) Offense—
(1) Generally—A physician who knowingly performs or induces an abortion on a minor in violation of the requirements of this section shall be fined under this title or imprisoned not more than one year, or both.
(2) Parental Notification—A physician who performs or induces an abortion on a minor who is a resident of a State other than the State in which the abortion is performed must provide, or cause his or her agent to provide, at least 24 hours actual notice to a parent of the minor before performing the abortion. If actual notice to such parent is not possible after a reasonable effort has been made, 24 hours constructive notice must be given to a parent.
(b) Exceptions—The notification requirement of subsection (a)(2) does not apply if
(1) the abortion is performed or induced in a State that has, in force, a law requiring parental involvement in a minor’s abortion decision and the physician complies with the requirements of that law;
(2) the physician is presented with documentation showing with a reasonable degree of certainty that a court in the minor’s State of residence has waived any parental notification required by the laws of that State, or has otherwise authorized that the minor be allowed to procure an abortion;
(3) the minor declares in a signed written statement that she is the victim of sexual abuse, neglect, or physical abuse by a parent, and, before an abortion is performed on the minor, the physician notifies the authorities specified to receive reports of child abuse or neglect by the law of the State in which the minor resides of the known or suspected abuse or neglect;
(4) the abortion is necessary to save the life of the minor because her life was endangered by a physical disorder, physical injury, or physical illness, including a life endangering physical condition caused by or arising from the pregnancy itself, or because in the reasonable medical judgment of the minor’s attending physician, the delay in performing an abortion occasioned by fulfilling the prior notification requirement of subsection (a)(2) would cause a substantial and irreversible impairment of a major bodily function of the minor arising from continued pregnancy, not including psychological or emotional conditions, but an exception under this paragraph does not apply unless the attending physician or an agent of such physician, within 24 hours after completion of the abortion, notifies a parent in writing that an abortion was performed on the minor and of the circumstances that warranted invocation of this paragraph; or
(5) the minor is physically accompanied by a person who presents the physician or his agent with documentation showing with a reasonable degree of certainty that he or she is in fact the parent of that minor.
[687] Calculated with data from vote 479: “Child Custody Protection Act.” U.S. House of Representatives, September 26, 2006. <clerk.house.gov>
|
Party |
Voted “Yes” |
Voted “No” |
Voted “Present” or Did Not Vote† |
|||
|
Number |
Portion |
Number |
Portion |
Number |
Portion |
|
|
Republican |
215 |
93% |
9 |
4% |
6 |
3% |
|
Democrat |
49 |
24% |
143 |
71% |
9 |
4% |
|
Independent |
0 |
0% |
1 |
100% |
0 |
0% |
|
NOTE: †Voting “Present” is effectively the same as not voting. |
||||||
[688] “Memorandum for the Administration of the United States Agency for International Development.” By George W. Bush. White House, January 22, 2001. <www.govinfo.gov>
“The Mexico City Policy announced by President Reagan in 1984 required nongovernmental organizations to agree as a condition of their receipt of Federal funds that such organizations would neither perform nor actively promote abortion as a method of family planning in other nations.”
[689] “Presidential Memorandum Regarding the Mexico City Policy.” By Donald Trump. White House, January 23, 2017. <www.govinfo.gov>
I hereby revoke the Presidential Memorandum of January 23, 2009, for the Secretary of State and the Administrator of the United States Agency for International Development (Mexico City Policy and Assistance for Voluntary Population Planning), and reinstate the Presidential Memorandum of January 22, 2001, for the Administrator of the United States Agency for International Development (Restoration of the Mexico City Policy).
I direct the Secretary of State, in coordination with the Secretary of Health and Human Services, to the extent allowable by law, to implement a plan to extend the requirements of the reinstated Memorandum to global health assistance furnished by all departments or agencies.
I further direct the Secretary of State to take all necessary actions, to the extent permitted by law, to ensure that U.S. taxpayer dollars do not fund organizations or programs that support or participate in the management of a program of coercive abortion or involuntary sterilization.
[690] “Memorandum on Protecting Women’s Health at Home and Abroad.” By Joseph R. Biden Jr. White House, January 28, 2021. <www.govinfo.gov>
Sec. 2. Revocations and Other Actions.
(b) The Presidential Memorandum of January 23, 2017 (The Mexico City Policy), is revoked.
[691] “Interview with Donald Trump.” By Tim Russert. Meet the Press, NBC, October 24, 1999. <www.nbcnews.com>
Tim Russert: Partial birth abortion, the eliminating of abortion in the third trimester: big issue in Washington. Would President Trump ban partial birth abortion?
Donald Trump: Well, look, I’m very pro-choice. I hate the concept of abortion. I hate it. I hate everything it stands for. I cringe when I listen to people debating the subject. But you still I just believe in choice. And, again, it may be a little bit of a New York background, because there is some different attitude in different parts of the country. And, you know, I was raised in New York, and grew up and work and everything else in New York City. But I am strongly for choice and, yet, I hate the concept of abortion.
Tim Russert: But you would not ban it?
Donald Trump: No.
Tim Russert: Or ban partial birth abortion?
Donald Trump: No. I am pro-choice in every respect and as far as it goes, but I just hate it.
[692] Book: The America We Deserve. By Donald Trump and Dave Shiftlett. Renaissance Books, 2000.
Page 31: “I support a woman’s right to choose, but I am uncomfortable with the procedures. When Tim Russert asked me on Meet the Press if I would ban partial-birth abortion, my pro-choice instincts led me to say no. After the show, I consulted two doctors I respect and, upon learning more about this procedure, I have concluded that I would support a ban.”
[693] Speech: “Donald Trump Before Conservative Political Action Conference.” C-SPAN, February 10, 2011. <www.c-span.org>
Time marker 16:22: “I’m pro-life.”
[694] Transcript: “Fox News Republican Party Primary Debate” Moderated by Bret Baier, Megyn Kelly, and Chris Wallace. Fox News, August 6, 2015. <www.washingtonpost.com>
Kelly: Mr. Trump, in 1999, you said you were, quote, “very pro-choice.” Even supporting partial-birth abortion. You favored an assault weapons ban as well. In 2004, you said in most cases you identified as a Democrat. Even in this campaign, your critics say you often sound more like a Democrat than a Republican, calling several of your opponents on the stage things like clowns and puppets. When did you actually become a Republican?
Trump: I don’t think they like me very much. I’ll tell you what. I’ve evolved on many issues over the years. And you know who else has? Is Ronald Reagan evolved on many issues.
And I am pro-life. And if you look at the question, I was in business. They asked me a question as to pro-life or choice. And I said if you let it run, that I hate the concept of abortion. I hate the concept of abortion. And then since then, I’ve very much evolved.
And what happened is friends of mine years ago were going to have a child, and it was going to be aborted. And it wasn’t aborted. And that child today is a total superstar, a great, great child. And I saw that. And I saw other instances.
And I am very, very proud to say that I am pro-life.
As far as being a Republican is concerned, I come from a place, New York City, which is virtually, I mean, it is almost exclusively Democrat. And I have really started to see some of the negatives—as an example, and I have a lot of liking for this man, but the last number of months of his brother’s administration were a catastrophe. And unfortunately, those few months gave us President Obama. And you can’t be happy about that.
[695] Transcript: Meet the Press. NBC News, August 16, 2015. <www.nbcnews.com>
Chuck Todd: Should some form of abortion always be legal?
Donald Trump: Well, to me, I have exceptions. Rape, incest, if the mother is going to die. And Ronald Reagan had those same exceptions. And many Republicans have those same exceptions. But I say rape, incest—
Chuck Todd: You said life of the mother. What about health of the mother?
Donald Trump: Well, I said actually if the mother’s close to death. And I’m talking about death. You know, because then you sort of say, like, “Well, maybe she’s not feeling so well—”
Chuck Todd: Well, that’s the line here. What is the constitutional right—
Donald Trump: Well—
Chuck Todd: —between the mother and the unborn child? Whose—
Donald Trump: My—
Chuck Todd: —constitutional rights matter more?
Donald Trump: Right. My statement on that happens to be, you know, if the mother will die. And you’re going to know that. And the problem with the life: If you say life, what does life mean? You have a cold and you’re going to end up having an abortion. So I have the three exceptions and pretty much the standard three exceptions that many Republicans have.
[696] Video: “Town Hall with Donald Trump.” Moderated by Chris Matthews. MSNBC, March 30, 2016. <www.youtube.com>
Time marker 30:18: “The answer is that there has to be some form of punishment.”
Time marker 31:22: “I have not determined what the punishment would be.”
[697] Article: “Trump Backtracks On Comments About Abortion And ‘Punishment’ For Women.” Brian Naylor. National Public Radio, March 30, 2016. <www.npr.org>
If Congress were to pass legislation making abortion illegal and the federal courts upheld this legislation, or any state were permitted to ban abortion under state and federal law, the doctor or any other person performing this illegal act upon a woman would be held legally responsible, not the woman. The woman is a victim in this case as is the life in her womb. My position has not changed—like Ronald Reagan, I am pro-life with exceptions.
[698] Transcript: “The Final 2016 U.S. Presidential Debate.” Moderated by Chris Wallace. Commission on Presidential Debates, October 19, 2016. <www.washingtonpost.com>
Wallace: Mr. Trump, you’re pro-life. But I want to ask you specifically: Do you want the court, including the justices that you will name, to overturn Roe v. Wade, which includes—in fact, states—a woman’s right to abortion?
Trump: Well, if that would happen, because I am pro-life, and I will be appointing pro-life judges, I would think that that will go back to the individual states.
Wallace: But I’m asking you specifically. Would you like to…
Trump: If they overturned it, it will go back to the states.
Wallace: But what I’m asking you, sir, is, do you want to see the court overturn—you just said you want to see the court protect the Second Amendment. Do you want to see the court overturn Roe v. Wade?
Trump: Well, if we put another two or perhaps three justice on, that’s really what’s going to be—that will happen. And that’ll happen automatically, in my opinion, because I am putting pro-life justices on the court. I will say this: It will go back to the states, and the states will then make a determination.
[699] Transcript: “President-Elect Trump Speaks to a Divided Country on 60 Minutes.” CBS News, November 13, 2016. <www.cbsnews.com>
Lesley Stahl: During the campaign, you said that you would appoint justices who were against abortion rights. Will you appoint—are you looking to appoint a justice who wants to overturn Roe v. Wade?
Donald Trump: So look, here’s what’s going to happen—I’m going to—I’m pro-life. The judges will be pro-life. They’ll be very—
Lesley Stahl: But what about overturning this law—
Donald Trump: Well, there are a couple of things. They’ll be pro-life, they’ll be—in terms of the whole gun situation, we know the Second Amendment and everybody’s talking about the Second Amendment and they’re trying to dice it up and change it, they’re going to be very pro-Second Amendment. But having to do with abortion if it ever were overturned, it would go back to the states. So it would go back to the states and—
[700] “Memorandum for the Administration of the United States Agency for International Development.” By George W. Bush. White House, January 22, 2001. <georgewbush-whitehouse.archives.gov>
“The Mexico City Policy announced by President Reagan in 1984 required nongovernmental organizations to agree as a condition of their receipt of Federal funds that such organizations would neither perform nor actively promote abortion as a method of family planning in other nations.”
[701] “Presidential Memorandum Regarding the Mexico City Policy.” By Donald Trump. White House, January 23, 2017. <www.govinfo.gov>
I hereby revoke the Presidential Memorandum of January 23, 2009, for the Secretary of State and the Administrator of the United States Agency for International Development (Mexico City Policy and Assistance for Voluntary Population Planning), and reinstate the Presidential Memorandum of January 22, 2001, for the Administrator of the United States Agency for International Development (Restoration of the Mexico City Policy).
I direct the Secretary of State, in coordination with the Secretary of Health and Human Services, to the extent allowable by law, to implement a plan to extend the requirements of the reinstated Memorandum to global health assistance furnished by all departments or agencies.
I further direct the Secretary of State to take all necessary actions, to the extent permitted by law, to ensure that U.S. taxpayer dollars do not fund organizations or programs that support or participate in the management of a program of coercive abortion or involuntary sterilization.
[702] “Executive Order on Protecting Vulnerable Newborn and Infant Children.” By Donald Trump. White House, September 25, 2020. <www.federalregister.gov>
Section 1. Purpose. Every infant born alive, no matter the circumstances of his or her birth, has the same dignity and the same rights as every other individual and is entitled to the same protections under Federal law. Such laws include the Emergency Medical Treatment and Labor Act (EMTALA), 42 U.S.C. 1395dd, which guarantees, in hospitals that have an emergency department, each individual’s right to an appropriate medical screening examination and to either stabilizing treatment or an appropriate transfer. They also include section 504 of the Rehabilitation Act (Rehab Act), 29 U.S.C. 794, which prohibits discrimination against individuals with disabilities by programs and activities receiving Federal funding. In addition, the Born-Alive Infants Protection Act, 1 U.S.C. 8, makes clear that all infants born alive are individuals for purposes of these and other Federal laws and are therefore afforded the same legal protections as any other person. Together, these laws help protect infants born alive from discrimination in the provision of medical treatment, including infants who require emergency medical treatment, who are premature, or who are born with disabilities. Such infants are entitled to meaningful and non-discriminatory access to medical examination and services, with the consent of a parent or guardian, when they present at hospitals receiving Federal funds.
Despite these laws, some hospitals refuse the required medical screening examination and stabilizing treatment or otherwise do not provide potentially lifesaving medical treatment to extremely premature or disabled infants, even when parents plead for such treatment. Hospitals might refuse to provide treatment to extremely premature infants—born alive before 24 weeks of gestation—because they believe these infants may not survive, may have to live with long-term disabilities, or may have a quality-of-life deemed to be inadequate. Active treatment of extremely premature infants has, however, been shown to improve their survival rates. And the denial of such treatment, or discouragement of parents from seeking such treatment for their children, devalues the lives of these children and may violate Federal law.
Sec. 2. Policy. It is the policy of the United States to recognize the human dignity and inherent worth of every newborn or other infant child, regardless of prematurity or disability, and to ensure for each child due protection under the law.
Sec. 3. (a) The Secretary of Health and Human Services (Secretary) shall ensure that individuals responsible for all programs and activities under his jurisdiction that receive Federal funding are aware of their obligations toward infants, including premature infants or infants with disabilities, who have an emergency medical condition in need of stabilizing treatment, under EMTALA and section 504 of the Rehab Act, as interpreted consistent with the Born-Alive Infants Protection Act. In particular, the Secretary shall ensure that individuals responsible for such programs and activities are aware that they are not excused from complying with these obligations, including the obligation to provide an appropriate medical screening examination and stabilizing treatment or transfer, when extremely premature infants are born alive or infants are born with disabilities. The Secretary shall also ensure that individuals responsible for such programs and activities are aware that they may not unlawfully discourage parents from seeking medical treatment for their infant child solely because of their infant child’s disability. The Secretary shall further ensure that individuals responsible for such programs and activities are aware of their obligations to provide stabilizing treatment that will allow the infant patients to be transferred to a more suitable facility if appropriate treatment is not possible at the initial location.
(b) The Secretary shall, as appropriate and consistent with applicable law, ensure that Federal funding disbursed by the Department of Health and Human Services is expended in full compliance with EMTALA and section 504 of the Rehab Act, as interpreted consistent with the Born-Alive Infants Protection Act, as reflected in the policy set forth in section 2 of this order.
(i) The Secretary shall, as appropriate and to the fullest extent permitted by law, investigate complaints of violations of applicable Federal laws with respect to infants born alive, including infants who have an emergency medical condition in need of stabilizing treatment or infants with disabilities whose parents seek medical treatment for their infants. The Secretary shall also clarify, in an easily understandable format, the process by which parents and hospital staff may submit such complaints for investigation under applicable Federal laws.
(ii) The Secretary shall take all appropriate enforcement action against individuals and organizations found through investigation to have violated applicable Federal laws, up to and including terminating Federal funding for non-compliant programs and activities.
(c) The Secretary shall, as appropriate and consistent with applicable law, prioritize the allocation of Department of Health and Human Services discretionary grant funding and National Institutes of Health research dollars for programs and activities conducting research to develop treatments that may improve survival — especially survival without impairment — of infants born alive, including premature infants or infants with disabilities, who have an emergency medical condition in need of stabilizing treatment.
(d) The Secretary shall, as appropriate and consistent with applicable law, prioritize the allocation of Department of Health and Human Services discretionary grant funding to programs and activities, including hospitals, that provide training to medical personnel regarding the provision of life-saving medical treatment to all infants born alive, including premature infants or infants with disabilities, who have an emergency medical condition in need of stabilizing treatment.
(e) The Secretary shall, as necessary and consistent with applicable law, issue such regulations or guidance as may be necessary to implement this order.
[703] Press release: “Senate Confirms Amy Coney Barrett to the Supreme Court.” U.S. Senate, Committee on the Judiciary, October 26, 2020. <www.judiciary.senate.gov>
Washington—Tonight, the U.S. Senate confirmed Amy Coney Barrett as an Associate Justice of the Supreme Court of the United States by a vote of 52–48.
Barrett is the 220th federal judge nominated by President Trump for a lifetime appointment and confirmed by the Republican Senate majority.
[704] Video: “Hesburgh Lecture 2016: Professor Amy Barrett at the JU Public Policy Institute.” Posted by Jacksonville University, November 3, 2016. <www.youtube.com>
Time marker 38:06:
[Amy Coney Barrett:] I don’t think that abortion, or the right to abortion, is, would change.
[Host:] You think some of the restrictions might change?
[Amy Coney Barrett:] I think some of the restrictions might change. I think that’s what we just saw last term in the case out of Texas. States, you know, after that Kermit Gosnell affair and all of that, states have imposed regulations on abortion clinics, and I think the question is, How much freedom is the court willing to let states have in regulating abortion? I think the question of, you know the court has held that in some circumstances, um, states can render partial-birth abortion illegal, very late-term abortions. I think that’s the kind of thing that would change. I don’t think that the core case, you know, Roe’s core holding that women have a right to an abortion, I don’t think that would change. But, I think the question of whether people can get very late-term abortions, you know, how many restrictions can be put on clinics, I think that would change.
[705] “Nomination of Amy Coney Barrett to the U.S. Supreme Court: Questions for the Record.” October 16, 2020. <www.judiciary.senate.gov>
Page 30:
30. During your nomination hearing, Senator Klobuchar asked whether you consider Roe v. Wade to be “super precedent.” You answered, “Roe doesn’t fall in that category” because it’s “not a case that everyone has accepted.”
a. Please state whether you have “accepted” Roe.
RESPONSE: In the exchange with Senator Klobuchar to which you are referring, I explained that the term “super precedent” is used in academic work to refer to cases that are so well settled that no political actors and no people seriously push for overruling. Roe does not fall within that category, but that does not mean that Roe should be overruled. Roe is a precedent of the Supreme Court entitled to respect under the doctrine of stare decisis.
[706] Webpage: “Cosponsors of Senate Bill S.1645: Women’s Health Protection Act of 2019.” U.S. Senate, 116th Congress (2019–2020). Accessed June 4, 2019 at <www.congress.gov>
“Sponsor: Sen. Blumenthal, Richard [D-CT] … (Introduced 05/23/2019) …. Cosponsors … 43 [42 Democrats and 1 Independent (Bernie Sanders)] … Harris, Kamala [D-CA]”
[707] Webpage: “S.1645: Women’s Health Protection Act of 2019.” U.S. Senate, 116th Congress (2019–2020). Accessed October 30, 2020 at <www.congress.gov>
Introduced in Senate (05/23/2019) …
(2) Health Care Provider.—The term “health care provider” means any entity or individual (including any physician, certified nurse-midwife, nurse practitioner, and physician assistant) that is—
(A) engaged in the delivery of health care services, including abortion services; and
(B) if required by law or regulation to be licensed or certified to engage in the delivery of such services, is so licensed or certified.
[708] Webpage: “S.1645: Women’s Health Protection Act of 2019.” U.S. Senate, 116th Congress (2019–2020). Accessed October 30, 2020 at <www.congress.gov>
Introduced in Senate (05/23/2019) …
(a) General rule.—A health care provider has a statutory right under this Act to provide abortion services, and may provide abortion services, and that provider’s patient has a corresponding right to receive such services, without any of the following limitations or requirements: ….
(9) A prohibition on abortion after fetal viability when, in the good-faith medical judgment of the treating health care provider, continuation of the pregnancy would pose a risk to the pregnant patient’s life or health.
[709] Webpage: “S.1645: Women’s Health Protection Act of 2019.” U.S. Senate, 116th Congress (2019–2020). Accessed October 30, 2020 at <www.congress.gov>
Introduced in Senate (05/23/2019) …
(a) Findings.—Congress finds the following:
(1) Access to safe, legal abortion services is essential to women’s health and central to women’s ability to participate equally in the economic and social life of the United States.
(2) Since 1973, the Supreme Court repeatedly has recognized the constitutional right of a woman to decide to terminate her pregnancy before fetal viability, and to terminate her pregnancy after fetal viability where it is necessary, in the good-faith medical judgment of the treating health care professional, for the preservation of her life or health.
(3) Nonetheless, access to safe, legal abortion services has been hindered across the United States in various ways, including blockades of health care facilities and associated violence, prohibitions of and restrictions on insurance coverage, restrictions which shame and stigmatize women seeking abortion services, and medically unnecessary regulations which neither confer any health benefit nor further the safety of abortion services, but which harm women by delaying access to, and reducing the availability of, services. Since 2010, States and local governments have passed more than 400 such restrictions singling out health care providers who offer abortion services and interfering with health care providers’ ability to provide reproductive health care services and the ability of patients to obtain those services. …
(20) Congressional action is necessary to put an end to harmful restrictions, to federally protect access to abortion services for all women regardless of where they live, and to protect the ability of reproductive health care providers to provide these services in a safe and accessible manner.
(b) Purpose.—It is the purpose of this Act—
(1) to permit health care providers to provide abortion services without limitations or requirements that single out the provision of abortion services for restrictions that are more burdensome than those restrictions imposed on medically comparable procedures, do not significantly advance women’s health or the safety of abortion services, and make abortion services more difficult to access….
Sec. 4. Permitted Services.
(a) General rule.—A health care provider has a statutory right under this Act to provide abortion services, and may provide abortion services, and that provider’s patient has a corresponding right to receive such services, without any of the following limitations or requirements:
(1) A requirement that a health care provider perform specific tests or medical procedures in connection with the provision of abortion services, unless generally required for the provision of medically comparable procedures.
(2) A requirement that the same health care provider who provides abortion services also perform specified tests, services, or procedures prior to or subsequent to the abortion.
(3) A requirement that a health care provider offer or provide the patient seeking abortion services medically inaccurate information in advance of or during abortion services.
(4) A limitation on a health care provider’s ability to prescribe or dispense drugs based on current evidence-based regimens or the provider’s good-faith medical judgment, other than a limitation generally applicable to the medical profession.
(5) A limitation on a health care provider’s ability to provide abortion services via telemedicine, other than a limitation generally applicable to the provision of medical services via telemedicine.
(6) A requirement or limitation concerning the physical plant, equipment, staffing, or hospital transfer arrangements of facilities where abortion services are provided, or the credentials or hospital privileges or status of personnel at such facilities, that is not imposed on facilities or the personnel of facilities where medically comparable procedures are performed.
(7) A requirement that, prior to obtaining an abortion, a patient make one or more medically unnecessary in-person visits to the provider of abortion services or to any individual or entity that does not provide abortion services.
(8) A prohibition on abortion prior to fetal viability, including a prohibition or restriction on a particular abortion procedure.
(9) A prohibition on abortion after fetal viability when, in the good-faith medical judgment of the treating health care provider, continuation of the pregnancy would pose a risk to the pregnant patient’s life or health.
(10) A limitation on a health care provider’s ability to provide immediate abortion services when that health care provider believes, based on the good-faith medical judgment of the provider, that delay would pose a risk to the patient’s health.
(11) A requirement that a patient seeking abortion services prior to fetal viability state the patient’s reasons for seeking abortion services, or a limitation on the provision of abortion services prior to fetal viability based on the patient’s reasons or perceived reasons for obtaining abortion services.
[710] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] VIII:
Specific and direct harm medically diagnosable even in early pregnancy may be involved. Maternity, or additional offspring, may force upon the woman a distressful life and future. Psychological harm may be imminent. Mental and physical health may be taxed by child care. There is also the distress, for all concerned, associated with the unwanted child, and there is the problem of bringing a child into a family already unable, psychologically and otherwise, to care for it. In other cases, as in this one, the additional difficulties and continuing stigma of unwed motherhood may be involved. All these are factors the woman and her responsible physician necessarily will consider in consultation.
[Section] XI:
For the stage subsequent to viability the State, in promoting its interest in the potentiality of human life, may, if it chooses, regulate, and even proscribe, abortion except where necessary, in appropriate medical judgment, for the preservation of the life or health of the mother. …
In Doe v. Bolton, post, p. 179, procedural requirements contained in one of the modern abortion statutes are considered. That opinion and this one, of course, are to be read together.
[711] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] IV: “[T]he medical judgment may be exercised in the light of all factors—physical, emotional, psychological, familial, and the woman’s age—relevant to the wellbeing of the patient. All these factors may relate to health.”
[712] Ruling: Planned Parenthood of Southeastern PA v. Casey. United States Supreme Court. June 29, 1992. <caselaw.findlaw.com>
Majority:
It must be stated at the outset and with clarity that Roe’s essential holding, the holding we reaffirm, has three parts. First is a recognition of the right of the woman to choose to have an abortion before viability and to obtain it without undue interference from the State. Before viability, the State’s interests are not strong enough to support a prohibition of abortion or the imposition of a substantial obstacle to the woman’s effective right to elect the procedure. Second is a confirmation of the State’s power to restrict abortions after fetal viability if the law contains exceptions for pregnancies which endanger the woman’s life or health. And third is the principle that the State has legitimate interests from the outset of the pregnancy in protecting the health of the woman and the life of the fetus that may become a child.
[713] Article: “We Asked Democrat Senators if Abortion is Ever Immoral. Here’s What They Said.” By Henry Rodgers. Daily Caller, February 27, 2019. <dailycaller.com>
Democratic senators on Capitol Hill had mixed responses—from saying it’s a woman’s choice to dodging the question altogether—about whether they were comfortable with calling abortion immoral in any circumstance.
The Daily Caller News Foundation asked nearly 10 Democratic senators about abortion and if there was a point at which it would be considered immoral Tuesday and Wednesday after the Republican-led Senate failed to pass a bill, which would mandate medical care and legal protections to infants born alive after an attempted abortion. Doctors who don’t comply would be punished. …
Democratic California Sen. Kamala Harris, a 2020 hopeful who voted against Republican Nebraska Sen. Ben Sasse’s bill, would not say if abortion was ever immoral.
“I think it’s up to a woman to make that decision, and I will always stand by that,” she told TheDCNF. [Daily Caller News Foundation] “I think she needs to make that decision with her doctor, with her priest, with her spouse. I would leave that decision up to them.”
[714] Senate Bill 311: “Born-Alive Abortion Survivors Protection Act.” U.S. Senate, 116th Congress (2019–2020). Accessed July 6, 2019 at <www.congress.gov>
Sponsor: Sen. Sasse, Ben [R–NE] (Introduced 01/31/2019) …
(a) Requirements for health care practitioners.—In the case of an abortion or attempted abortion that results in a child born alive:
(1) Degree of Care Required; Immediate Admission to a Hospital.—Any health care practitioner present at the time the child is born alive shall—
(A) exercise the same degree of professional skill, care, and diligence to preserve the life and health of the child as a reasonably diligent and conscientious health care practitioner would render to any other child born alive at the same gestational age; and
(B) following the exercise of skill, care, and diligence required under subparagraph (A), ensure that the child born alive is immediately transported and admitted to a hospital.
(2) Mandatory Reporting of Violations.—A health care practitioner or any employee of a hospital, a physician’s office, or an abortion clinic who has knowledge of a failure to comply with the requirements of paragraph (1) shall immediately report the failure to an appropriate State or Federal law enforcement agency, or to both.
(b) Penalties.—
(1) In General.—Whoever violates subsection (a) shall be fined under this title, imprisoned for not more than 5 years, or both.
(2) Intentional Killing of Child Born Alive.—Whoever intentionally performs or attempts to perform an overt act that kills a child born alive described under subsection (a), shall be punished as under section 1111 of this title for intentionally killing or attempting to kill a human being.
(c) Bar to prosecution.—The mother of a child born alive described under subsection (a) may not be prosecuted for a violation of this section, an attempt to violate this section, a conspiracy to violate this section, or an offense under section 3 or 4 of this title based on such a violation.
[715] Calculated with data from vote 27: “Cloture on the Motion to Proceed: Born-Alive Abortion Survivors Protection Act.” U.S. Senate, February 25, 2019. <www.senate.gov>
Required For Majority: 3/5 … Vote Result: Cloture on the Motion to Proceed Rejected … Nays … Harris (D–CA) …
|
Party |
Voted “Yes” |
Voted “No” |
Voted “Present” or Did Not Vote † |
|||
|
Number |
Portion |
Number |
Portion |
Number |
Portion |
|
|
Republican |
50 |
94% |
0 |
0% |
3 |
6% |
|
Democrat |
3 |
7% |
42 |
93% |
0 |
0% |
|
Independent |
0 |
0% |
2 |
100% |
0 |
0% |
|
NOTE: † Voting “Present” is effectively the same as not voting. |
||||||
[716] Webpage: “Reproductive Rights Act.” Kamala Harris for the People. Accessed June 4, 2019 at <bit.ly>
Similar to the preclearance requirement of the Voting Rights Act, Harris will require, for the first time, that states and localities with a history of violating Roe v. Wade obtain approval from her Department of Justice before any abortion law or practice can take effect. …
No abortion law or practice will take effect until the Department of Justice certifies it comports with Roe v. Wade.
• Under the plan, any change with respect to abortion in a covered jurisdiction will remain legally unenforceable until DOJ [Department of Justice] determines it comports with the standards laid out by the Supreme Court in Roe v. Wade, as applied in Whole Woman’s Health v. Hellerstedt, and the Women’s Health Protection Act, which Harris co-sponsors in the Senate.
• More than just codifying every woman’s federal right to an abortion, this will shift the burden to jurisdictions with a pattern of violating Roe to prove any new law or practice does not deny or abridge the fundamental right to access abortion.
• Jurisdictions will be required to submit any proposed change to DOJ. If the jurisdiction is unable to prove the change comports with Roe and the Women’s Health Protection Act, DOJ must object to the change.
[717] Webpage: “Cosponsors of House Joint Resolution 20: Proposing an Amendment to the Constitution of the United States with Respect to the Right to Life.” U.S. House of Representatives, 107th Congress (2001–2002). Accessed October 28, 2020 at <www.congress.gov>
“Sponsor: Rep. Oberstar, James L. [D-MN-8]; Cosponsor statistics: 34 current … Cosponsor … Rep. Pence, Mike [R-IN-2]”
[718] House Joint Resolution 20: “Proposing an Amendment to the Constitution of the United States with Respect to the Right to Life.” U.S. House of Representatives, 107th Congress (2001–2002). Accessed October 28, 2020 at <www.congress.gov>
Proposing an amendment to the Constitution of the United States with respect to the right to life.
Resolved by the Senate and House of Representatives of the United States of America in Congress assembled (two-thirds of each House concurring therein), That the following article is proposed as an amendment to the Constitution of the United States, to be valid only if ratified by the legislatures of three-fourths of the several States within seven years after the date of final passage of this joint resolution:
Article —
Section 1. With respect to the right to life, the word “person” as used in this article and in the fifth and fourteenth articles of amendment to the Constitution of the United States applies to all human beings irrespective of age, health, function, or condition of dependency, including their unborn offspring at every stage of their biological development.
Section 2. No unborn person shall be deprived of life by any person: Provided, however, That nothing in this article shall prohibit a law permitting only those medical procedures required to prevent the death of the mother.
Section 3. The Congress and the several States shall have power to enforce this article by appropriate legislation.
[719] Vote on House Resolution 4965: “Partial-Birth Abortion Ban Act.” U.S. House of Representatives, 107th Congress (2001–20002), July 24, 2002. <clerk.house.gov>
“Pence … Yea”
[720] Webpage: “Summary of House Resolution 4965: Partial-Birth Abortion Ban Act of 2002.” U.S. House of Representatives, 107th Congress (2001–2002). Accessed October 3, 2020 at <www.congress.gov>
Reported to House Without Amendment (07/23/2002)
Partial-Birth Abortion Ban Act of 2002 – Amends the Federal criminal code to prohibit any physician or other individual from knowingly performing a partial-birth abortion, except when necessary to save the life of a mother that is endangered by a physical disorder, illness, or injury.
Defines a “partial-birth abortion” as an abortion in which: (1) the person performing the abortion deliberately and intentionally vaginally delivers a living fetus until, in the case of a head-first presentation, the entire fetal head is outside the mother’s body; or in the case of a breech presentation, any part of the fetal trunk past the naval is outside the mother’s body for the purpose of performing an overt act that the person knows will kill the partially delivered living fetus; and (2) performs the overt act, other than completion of delivery, that kills the partially delivered living fetus.
Authorizes the father, if married to the mother at the time of the abortion, and the maternal grandparents of the fetus, if the mother is under 18 years of age, to obtain specified relief in a civil action, unless the pregnancy resulted from the plaintiff’s criminal conduct or the plaintiff consented to the abortion.
Authorizes a defendant accused of an offense under this Act to seek a hearing before the State Medical Board on whether the physician’s conduct was necessary to save the life of the mother.
Prohibits the prosecution of a woman upon whom a partial-birth abortion is performed for conspiracy to violate this Act or under provisions regarding punishment as a principal or an accessory or for concealment of a felony.
[721] Vote on House Resolution 760: “Partial-Birth Abortion Ban Act.” U.S. House of Representatives, 108th Congress (2003–2004), June 4, 2003. <clerk.house.gov>
“Pence … Yea”
[722] Webpage: “Summary of House Resolution 760: Partial-Birth Abortion Ban Act of 2003.” U.S. House of Representatives, 108th Congress (2003–2004). Accessed October 3, 2020 at <www.congress.gov>
Passed House Without Amendment (06/04/2003)
(This measure has not been amended since it was introduced on February 13, 2003. The summary of that version is repeated here.)
Partial-Birth Abortion Ban Act of 2003 – Amends the Federal criminal code to prohibit any physician or other individual from knowingly performing a partial-birth abortion, except when necessary to save the life of a mother that is endangered by a physical disorder, illness, or injury.
Defines a “partial-birth abortion” as an abortion in which the person performing the abortion: (1) deliberately and intentionally vaginally delivers a living fetus until, in the case of a head-first presentation, the entire fetal head is outside the mother’s body, or, in the case of a breech presentation, any part of the fetal trunk past the navel is outside the mother’s body; and (2) performs the overt act, other than completion of delivery, that kills the partially delivered living fetus.
Authorizes the father, if married to the mother at the time of the abortion, and the maternal grandparents of the fetus, if the mother is under 18 years of age, to obtain specified relief in a civil action, unless the pregnancy resulted from the plaintiff’s criminal conduct or the plaintiff consented to the abortion.
Authorizes a defendant accused of an offense under this Act to seek a hearing before the State Medical Board on whether the physician’s conduct was necessary to save the life of the mother.
Prohibits the prosecution of a woman upon whom a partial-birth abortion is performed for conspiracy to violate this Act or under provisions regarding punishment as a principal or an accessory or for concealment of a felony.
[723] Calculated with data from:
a) Vote 530: “Partial-Birth Abortion Ban Act of 2003.” U.S. House of Representatives, October 2, 2003. <clerk.house.gov>
b) Vote 402: “Partial-Birth Abortion Ban Act of 2003.” U.S. Senate, October 21, 2003. <www.senate.gov>
Combined vote totals from both Houses of Congress:
|
Party |
Voted “Yes” |
Voted “No” |
Voted “Present” or Did Not Vote† |
|||
|
Number |
Portion |
Number |
Portion |
Number |
Portion |
|
|
Republican |
265 |
95% |
7 |
3% |
8 |
3% |
|
Democrat |
80 |
32% |
167 |
66% |
6 |
2% |
|
Independent |
0 |
0% |
2 |
100% |
0 |
0% |
|
NOTE: †Voting “Present” is effectively the same as not voting. |
||||||
[724] Webpage: “Actions on Senate Bill 3: Partial-Birth Abortion Ban Act of 2003.” U.S. Senate, 108th Congress (2003–2004). Accessed April 21, 2017 at <www.congress.gov>
|
Date |
Action |
|
2/14/2003 |
Introduced in Senate |
|
3/13/2003 |
Passed Senate with an amendment by Yea–Nay Vote. 64–33. Record Vote Number: 51 |
|
10/2/2003 |
Conference report agreed to in House: On agreeing to the conference report Agreed to by the Yeas and Nays: 281–142 (Roll no. 530). |
|
10/21/2003 |
Conference report agreed to in Senate: Senate agreed to conference report by Yea–Nay Vote. 64–34. Record Vote Number: 402. |
|
11/5/2003 |
Signed by President. Became Public Law No: 108-105. |
[725] Webpage: “Cosponsors of House Resolution 2175: Born-Alive Infants Protection Act of 2002.” U.S. House of Representatives, 107th Congress (2001–2002). Accessed October 3, 2020 at <www.congress.gov>
“Sponsor: Rep. Chabot, Steve [R-OH-1] … Cosponsor statistics: 105 current … Rep. Pence, Mike [R-IN-2]”
[726] House Resolution 2175: Born-Alive Infants Protection Act of 2002.” U.S. House of Representatives 107th Congress (2001–2002). Accessed October 28, 2020 at <www.congress.gov>
An Act to protect infants who are born alive. …
(a) In determining the meaning of any Act of Congress, or of any ruling, regulation, or interpretation of the various administrative bureaus and agencies of the United States, the words “person”, “human being”, “child”, and “individual”, shall include every infant member of the species homo sapiens who is born alive at any stage of development.
(b) As used in this section, the term “born alive”, with respect to a member of the species homo sapiens, means the complete expulsion or extraction from his or her mother of that member, at any stage of development, who after such expulsion or extraction breathes or has a beating heart, pulsation of the umbilical cord, or definite movement of voluntary muscles, regardless of whether the umbilical cord has been cut, and regardless of whether the expulsion or extraction occurs as a result of natural or induced labor, cesarean section, or induced abortion.
(c) Nothing in this section shall be construed to affirm, deny, expand, or contract any legal status or legal right applicable to any member of the species homo sapiens at any point prior to being “born alive” as defined in this section.
[727] Born-Alive Infants Protection Act of 2001. Congressional Record, March 12, 2002. Pages 792–797. <www.govinfo.gov>
Page 796:
The SPEAKER pro tempore (Mr. STEARNS). The question is on the motion offered by the gentleman from Wisconsin (Mr. SENSENBRENNER) that the House suspend the rules and pass the bill, H.R. 2175 [Born-Alive Infants Protection Act].
The question was taken.
The SPEAKER pro tempore. In the opinion of the Chair, two-thirds of those present have voted in the affirmative.
[728] Born-Alive Infants Protection Act of 2001. Congressional Record, July 18, 2002. Page 7084. <www.gpo.gov>
Page 7084:
There being no objection, the Senate proceeded to consider the bill.
Mr. REID. Mr. President, I ask unanimous consent that the bill be read the third time and passed, the motion to reconsider be laid upon the table, and that any statements relating to the bill be printed in the RECORD.
The PRESIDING OFFICER. Without objection, it is so ordered.
The bill (H.R. 2175) was read the third time and passed.
[729] Public Law 107-207: “Born-Alive Infants Protection Act of 2002.” 107th United States Congress. Signed into law by President George W. Bush on August 5, 2002. <www.congress.gov>
An Act
To protect infants who are born alive. [H.R. 2175] …
(a) In determining the meaning of any Act of Congress, or of any ruling, regulation, or interpretation of the various administrative bureaus and agencies of the United States, the words “person”, “human being”, “child”, and “individual”, shall include every infant member of the species homo sapiens who is born alive at any stage of development.
(b) As used in this section, the term “born alive”, with respect to a member of the species homo sapiens, means the complete expulsion or extraction from his or her mother of that member, at any stage of development, who after such expulsion or extraction breathes or has a beating heart, pulsation of the umbilical cord, or definite movement of voluntary muscles, regardless of whether the umbilical cord has been cut, and regardless of whether the expulsion or extraction occurs as a result of natural or induced labor, cesarean section, or induced abortion.
(c) Nothing in this section shall be construed to affirm, deny, expand, or contract any legal status or legal right applicable to any member of the species homo sapiens at any point prior to being “born alive” as defined in this section.
[730] Webpage: “Cosponsors of House Resolution 5939: No Taxpayer Funding for Abortion Act.” U.S. House of Representatives, 111th Congress (2009–2010). Accessed October 5, 2020 at <www.congress.gov>
“Sponsor: Rep. Smith, Christopher H. [R-NJ-4] … Cosponsor statistics: 186 current … Rep. Pence, Mike [R-IN-6]”
[731] Webpage: “Summary of House Resolution 5939: No Taxpayer Funding for Abortion Act.” U.S. House of Representatives, 111th Congress (2009–2010). Accessed October 5, 2020 at <www.congress.gov>
Introduced in House (07/29/2010)
No Taxpayer Funding for Abortion Act – Prohibits: (1) the expenditure of funds authorized or appropriated by federal law or funds in any trust fund to which funds are authorized or appropriated by federal law for any abortion or for health benefits coverage that includes coverage of abortion; (2) any tax benefits for amounts paid or incurred for an abortion or for a health benefits plan (including premium assistance) that includes coverage of abortion; and (3) the inclusion of abortion in any health care service furnished by a federal health care facility or by any physician or other individual employed by the federal government. Exempts from such prohibitions an abortion if the pregnancy is the result of rape or incest with a minor, or if the woman suffers from a physical disorder, injury, or illness that would, as certified by a physician, place the women in danger of death unless an abortion is performed, including a life-endangering physical condition caused by or arising from the pregnancy itself. Makes such prohibitions applicable to federal funding within the budget of the District of Columbia.
Prohibits federal agencies or programs and states and local governments that receive federal financial assistance from discriminating against any individual or institutional health care entity on the basis that such entity does not provide, pay for, provide coverage of, or refer for abortions. Designates the Office for Civil Rights of the Department of Health and Human Services (HHS) to receive, and coordinate the investigation of, discrimination complaints.
[732] Webpage: “Cosponsors of House Resolution 356: Unborn Child Pain Awareness Act of 2005.” U.S. House of Representatives, 109th Congress (2005–2006). Accessed October 5, 2020 at <www.congress.gov>
“Sponsor: Rep. Smith, Christopher H. [R-NJ-4] … Cosponsor statistics: 142 current … Rep. Pence, Mike [R-IN-6]”
[733] Webpage: “Summary of House Resolution 356: Unborn Child Pain Awareness Act of 2005.” U.S. House of Representatives, 109th Congress (2005–2006). Accessed October 5, 2020 at <www.congress.gov>
Introduced in House (01/25/2005)
Unborn Child Pain Awareness Act of 2005 – Amends the Public Health Service Act to require an abortion provider, before beginning any abortion of a pain-capable unborn child (defined as an unborn child who has reached a probable stage of development of 20 weeks after fertilization), to: (1) make a specified statement to the pregnant woman that Congress has determined that there is substantial evidence that the process will cause the unborn child pain, and that the mother has the option of having pain-reducing drugs administered directly to the child; (2) provide to the woman an Unborn Child Pain Awareness Brochure (unless she waives receipt) or information on accessing such brochure on the Internet; (3) provide to the woman an Unborn Child Pain Awareness Decision Form; and (4) obtain on the form the woman’s signature and her explicit request for or refusal of the administration of drugs to the child.
Creates an exception for certified medical emergencies.
Establishes penalties for willfully failing to comply with this Act, including civil penalties, medical license suspension, or both. Authorizes: (1) specified officials to bring suit in Federal court; and (2) private rights of action by a parent or guardian of a woman who is an unemancipated minor.
Requires each State and State medical licensing authority to promulgate procedures for the revocation or suspension of a provider’s license upon a court finding that the provider has violated this Act. Subjects a State that fails to implement such procedures to loss of Medicaid funding.
[734] Webpage: “Cosponsors of House Resolution 2805: Post-Abortion Depression Research and Care Act.” U.S. House of Representatives, 107th Congress (2001–2002). Accessed October 5, 2020 at <www.congress.gov>
“Sponsor: Rep. Pitts, Joseph R. [R-PA-16] … Cosponsor statistics: 18 current … Rep. Pence, Mike [R-IN-2]”
[735] Webpage: “Summary of House Resolution 2805: Post-Abortion Depression Research and Care Act.” U.S. House of Representatives, 107th Congress (2001–2002). Accessed October 5, 2020 at <www.congress.gov>
Introduced in House (08/02/2001)
Post-Abortion Depression Research and Care Act – Requires the Secretary of Health and Human Services, acting through the Director of the National Institutes of Health and the Director of the National Institute of Mental Health, to expand and intensify research and related activities of the Institute with respect to post-abortion depression and post-abortion psychosis.
Requires the Director of the National Institute of Mental Health to: (1) conduct or support research to expand the understanding of the causes of, and to find a cure for, post-abortion conditions; and (2) conduct a national longitudinal study to determine the incidence and prevalence of cases of post-abortion conditions, and the symptoms, severity, and duration of such cases, toward the goal of more fully identifying the characteristics of such cases and developing diagnostic techniques.
Requires the Secretary to make grants of up to $100,000 per fiscal year, under specified conditions, to provide for projects for the establishment, operation, and coordination of effective and cost-efficient systems for the delivery of essential services to individuals with post-abortion depression or post-abortion psychosis.
[736] Webpage: “Cosponsors of House Resolution 482: RU-486 Patient Health and Safety Protection Act.” U.S. House of Representatives, 107th Congress (2001–2002). Accessed October 3, 2020 at <www.congress.gov>
“Sponsor: Rep. Vitter, David [R-LA-1] … Cosponsor statistics: 37 current … Rep. Pence, Mike [R-IN-2]”
[737] Webpage: “Summary of House Resolution 482: RU-486 Patient Health and Safety Protection Act.” U.S. House of Representatives, 107th Congress (2001–2002). Accessed October 3, 2020 at <www.congress.gov>
Introduced in House (02/06/2001)
RU-486 Patient Health and Safety Protection Act – Restricts the prescribing of the drug mifepristone (commonly referred to as RU-486, to be marketed as Mifeprex) to physicians who meet specified requirements.
[738] Webpage: “Cosponsors of House Resolution 195: Informed Choice Act.” U.S. House of Representatives, 108th Congress (2003–2004). Accessed October 5, 2020 at <www.congress.gov>
“Sponsor: Rep. Stearns, Cliff [R-FL-6] … Cosponsor statistics: 53 current … Rep. Pence, Mike [R-IN-6]”
[739] Webpage: “Summary of House Resolution 195: Informed Choice Act.” U.S. House of Representatives, 108th Congress (2003–2004). Accessed October 5, 2020 at <www.congress.gov>
Introduced in House (01/07/2003)
Informed Choice Act – Allows the Secretary of Health and Human Services to make grants to free community based pregnancy help medical clinics for the purchase of ultrasound equipment, which shall be used to provide free ultrasound examinations to pregnant women. Requires each grant recipient to undertake certain actions, including to: (1) provide to each woman receiving services a visual image of the fetus from the ultrasound examination and a general anatomical and physiological description of the characteristics of the fetus; and (2) provide information on abortion and alternatives to abortion such as childbirth and adoption, and information concerning public and private agencies that will assist in those alternatives. Limits each grant to a maximum amount of 50 percent of the purchase price cost of the ultrasound machine involved or $20,000, whichever is less.
[740] Webpage: “Cosponsors of House Resolution 3192: Pregnant Women Support Act.” U.S. House of Representatives, 110th Congress (2007–2008). Accessed October 5, 2020 at <www.congress.gov>
“Sponsor: Rep. Davis, Lincoln [R-TN-4] … Cosponsor statistics: 142 current … Rep. Pence, Mike [R-IN-6]”
[741] Webpage: “Summary of House Resolution 3192: Pregnant Women Support Act.” U.S. House of Representatives, 110th Congress (2007–2008). Accessed October 5, 2020 at <www.congress.gov>
Introduced in House (07/26/2007)
Pregnant Women Support Act – Allows the Secretary of Health and Human Services, acting through the Director of the Centers for Disease Control and Prevention (CDC), to make grants to states for collecting and reporting abortion surveillance data.
Requires health facilities that perform abortions to obtained informed consent from a pregnant woman seeking an abortion.
Amends title XXI (State Children’s Health Insurance Program) (SCHIP) of the Social Security Act to allow states to extend health care coverage to an unborn child.
Amends the Public Health Service Act to prohibit a health insurance issuer offering individual coverage from imposing a preexisting condition exclusion or a waiting period or otherwise discriminating against a woman on the basis that she is pregnant.
Allows the Secretary to make grants for the purchase of ultrasound equipment for examinations of pregnant women.
Provides for the collection and dissemination of information on Down syndrome and other prenatally diagnosed conditions.
[742] Webpage: “Cosponsors of House Resolution 217: Title X Abortion Provider Prohibition Act.” U.S. House of Representatives, 112th Congress (2011–2012). Accessed October 5, 2020 at <www.congress.gov>
“Sponsor: Rep. Pence, Mike [R-IN-6] … Cosponsor statistics: 178 current”
[743] Webpage: “Summary of House Resolution 217: Title X Abortion Provider Prohibition Act.” U.S. House of Representatives, 112th Congress (2011–2012). Accessed October 5, 2020 at <www.congress.gov>
Introduced in House (01/07/2011)
Title X Abortion Provider Prohibition Act – Amends the Public Health Service Act to prohibit the Secretary of Health and Human Service (HHS) from providing any federal family planning assistance to an entity unless the entity certifies that, during the period of such assistance, the entity will not perform, and will not provide any funds to any other entity that performs, an abortion. Excludes an abortion where: (1) the pregnancy is the result of an act of rape or an act of incest against a minor; or (2) a physician certifies that the woman suffered from a physical disorder, injury, or illness that would place the woman in danger of death unless an abortion is performed, including a condition caused by or arising from the pregnancy. Excludes hospitals from such requirement so long as the hospital does not provide funds to any non-hospital entity that performs an abortion.
Requires the Secretary to annually provide Congress: (1) information on grantees who performed abortions under the exceptions; and (2) a list of entities to which grant funds are made available.
[744] Webpage: “Indiana Governor History.” State of Indiana. Accessed October 6, 2020 at <www.in.gov>
“Michael R. Pence – Governor of Indiana – January 14, 2013–January 9, 2017”
[745] Webpage: “Senate Bill 0371.” State of Indiana, 118th General Assembly (2013). <archive.iga.in.gov>
DIGEST OF SB 371 (Updated April 11, 2013 11:41 am – DI 84)
Abortion inducing drugs and abortion clinics. Amends the definition of “abortion” to include abortions by surgical procedures and by abortion inducing drugs. Amends the definition of “abortion clinic” to, beginning January 1, 2014, include facilities that provide abortion inducing drugs. Prohibits the state department of health (state department) from exempting an abortion clinic seeking licensure after December 31, 2013 from licensure requirements. Specifies that an abortion inducing drug may not be dispensed, prescribed, administered, or otherwise given to a pregnant woman after nine weeks of postfertilization age unless the Food and Drug Administration has approved the drug to be used later than nine weeks. Requires a physician to examine a pregnant woman in person before prescribing or dispensing an abortion inducing drug. Requires that the written certification required of a pregnant woman before undergoing an abortion be on a form developed by the state department. Requires the state department to develop an informed consent brochure and post the brochure on the state department’s web site. Requires the abortion provider to distribute the brochure to a patient in color and with specified information included on the back cover. Requires the abortion provider to be the one to perform pre-abortion fetal ultrasound imaging and auscultation of the fetal heart tone. Provides that if the pregnant woman does not want to listen to the auscultation of the fetal heart tone, the woman must certify to that in writing and on a form developed by the state department.
[746] Webpage: “Action List: Senate Bill 0371.” State of Indiana, 118th General Assembly (2013). <archive.iga.in.gov>
“05/01/2013 … Signed by the Governor”
[747] Webpage: “Senate Bill 292: Abortion Providers.” State of Indiana, 118th General Assembly (2014). <iga.in.gov>
Authorizes the state department of health (state department) to inspect an abortion clinic at least one time per year and to conduct complaint inspections as needed. Requires a pregnant woman to be informed orally and in writing at least 18 hours before the abortion of an emergency telephone number for the facility that is available and answered 24 hours a day, seven days a week. Requires a physician who is performing an abortion to have hospital admitting privileges in writing. Requires the abortion clinic to keep at the clinic a copy of the admitting privileges of certain physicians and to provide a copy of the admitting privileges to the state department. Requires the state department to: (1) verify the validity of the admitting privileges documents; (2) remove any identifying information from the admitting privileges document before releasing the document; and (3) confirm to a member of the public, upon request, that admitting privileges have been received by the state department.
[748] Webpage: “Actions for Senate Bill 292.” State of Indiana, 118th General Assembly (2014). <iga.in.gov>
“03/25/2014 … Signed by the Governor”
[749] Webpage: “Senate Bill 329: Disposition of Aborted Remains.” State of Indiana, 119th General Assembly (2015). <iga.in.gov>
Defines “fetus”. Establishes a right, beginning January 1, 2016, for a pregnant woman who has an abortion to determine the final disposition of the aborted fetus. Requires that a pregnant woman be informed orally and in writing before an abortion: (1) that the pregnant woman has a right to determine the final disposition of the remains of the aborted fetus; (2) of available options for disposition of the aborted fetus; and (3) of available counseling services. Requires the state department of health to: (1) adopt rules concerning the disposal methods to be used for aborted fetuses; and (2) develop the forms for certain information that is to be provided to the pregnant woman.
[750] Webpage: “Actions for Senate Bill 329.” State of Indiana, 119th General Assembly (2015). <iga.in.gov>
“05/04/2015 … Signed by the Governor”
[751] Webpage: “House Bill 1337: Abortion.” State of Indiana, 119th General Assembly (2016). <iga.in.gov>
Requires the state department of health to develop certain information concerning perinatal hospice care. Requires physicians to provide information about perinatal hospice care to a pregnant woman who is considering an abortion because the unborn child has been diagnosed with a lethal fetal anomaly. Requires documentation as a matter of informed consent to an abortion that the pregnant woman received the required information about perinatal hospice care. Provides that the gender of the fetus and the medical indication by diagnosis code for the fetus and the mother must be reported on the pregnancy termination form for an early pre-viability termination. Prohibits a person from performing an abortion if the person knows that the pregnant woman is seeking the abortion solely because of: (1) the race, color, national origin, ancestry, or sex of the fetus; or (2) a diagnosis or potential diagnosis of the fetus having Down syndrome or any other disability. Provides for disciplinary sanctions and civil liability for wrongful death if a person knowingly or intentionally performs a sex selective abortion or an abortion conducted because of a diagnosis or potential diagnosis of Down syndrome or any other disability. Provides that informed consent for an abortion must be obtained in a private setting. Provides that a pregnant woman considering an abortion must be given the opportunity to view the fetal ultrasound imaging and hear the auscultation of the fetal heart tone at least 18 hours before the abortion is performed and at the same time that informed consent is obtained. Provides that a written agreement between a physician performing an abortion and a physician who has written admitting privileges at a hospital in the county or contiguous county concerning the management of possible complications of the services must be renewed annually. Requires the state department of health (state department) to submit copies of admitting privileges and written agreements between physicians to other hospitals in the county and contiguous counties where abortions are performed. Requires that certain forms must include lines for the signature of the physician or other provider and the professional credentials of the physician or other provider. Provides that a person who knowingly transports an aborted fetus into, or out of, Indiana commits a Class A misdemeanor, unless the aborted fetus is transported for the sole purpose of final disposition. Provides that a miscarried or aborted fetus must be interred or cremated by a facility having possession of the remains. Requires a person or facility having possession of a miscarried or aborted fetus to ensure that the miscarried fetus or aborted fetus is preserved until final disposition occurs. Specifies that: (1) a person is not required to designated a name for the miscarried or aborted fetus; and (2) information submitted with respect to the disposition of a miscarried or aborted fetus that may be used to identify the parent or parents of a miscarried fetus or a pregnant who had an abortion is confidential and must be redacted from any public records maintained under the burial permit law. Specifies that miscarried and aborted fetuses may be cremated by simultaneous cremation. Excludes the final disposition of a miscarried or aborted fetus from the law governing the treatment of infectious or pathological waste. Makes conforming changes. Provides that the performance of an abortion solely because of the race, color, sex, disability, national origin, or ancestry of the fetus or a violation of certain statutes protecting the right of conscience regarding abortion is a discriminatory practice for purposes of the civil rights law. Defines fetal tissue. Prohibits an individual from acquiring, receiving, selling, or transferring fetal tissue. Makes it a Level 5 felony to unlawfully: (1) transfer; and (2) collect fetal tissue. Establishes an exemption for the criminal penalty of unlawful use of an embryo if the transfer or receipt of a fetus was requested in writing by a biological parent for purposes of an autopsy.
[752] Webpage: “Actions for House Bill 1337.” State of Indiana, 119th General Assembly (2016). <iga.in.gov>
“03/24/2016 … Signed by the Governor”
[753] Statement: “Congressional Action to Protect Choice.” By Elizabeth Warren. May 17, 2019. <medium.com>
Congress should pass new federal laws that protect access to reproductive care from right-wing ideologues in the states. Federal laws that ensure real access to birth control and abortion care for all women. Federal laws that will stand no matter what the Supreme Court does. …
Create Federal, Statutory Rights That Parallel the Constitutional Right in Roe V. Wade. … Congress should do its job and protect their constituents from these efforts by establishing affirmative, statutory rights that parallel Roe vs. Wade.
[754] Statement: “Congressional Action to Protect Choice.” By Elizabeth Warren. May 17, 2019. <medium.com>
Congress should pass new federal laws that protect access to reproductive care from right-wing ideologues in the states. Federal laws that ensure real access to birth control and abortion care for all women. Federal laws that will stand no matter what the Supreme Court does. …
Guarantee Reproductive Health Coverage as Part of All Health Coverage. All women—no matter where they live, where they’re from, how much money they make, or the color of their skin—are entitled to access the high-quality, evidence-based reproductive health care that is envisioned by Roe. Making that a reality starts with repealing the Hyde Amendment, which blocks abortion coverage for women under federally funded health care programs like Medicaid, the VA [Department of Veteran Affairs], and the Indian Health Service. Congress should also expand culturally- and linguistically-appropriate services and information and include immigrant women in conversations about coverage and access. Congress must also pass the EACH [Equal Access to Abortion Coverage in Health Insurance] Woman Act, which would also prohibit abortion restrictions on private insurance. And we should ensure that all future health coverage—including Medicare for All—includes contraception and abortion coverage.
[755] Statement: “Congressional Action to Protect Choice.” By Elizabeth Warren. May 17, 2019. <medium.com>
Congress should pass new federal laws that protect access to reproductive care from right-wing ideologues in the states. Federal laws that ensure real access to birth control and abortion care for all women. Federal laws that will stand no matter what the Supreme Court does. …
Pass Federal Laws to Preempt State Efforts That Functionally Limit Access to Reproductive Health Care. States have passed countless Targeted Regulations on Abortion Providers (TRAP) laws, which are designed to functionally limit and eliminate women’s access to abortion care while not technically contravening Roe. … A bill already proposed in Congress, The Women’s Health Protection Act, would provide the mechanism to block these kinds of schemes concocted to deny women access to care. Congress should pass it.
[756] Webpage: “Summary of Senate Bill S.510: Women’s Health Protection Act of 2017.” U.S. Senate, 115th Congress (2017–2018). Accessed May 28, 2019 at <www.congress.gov>
Introduced in Senate (03/02/2017)
Women’s Health Protection Act of 2017
This bill prohibits any government from imposing on abortion services:
• a requirement that a medical professional perform specific tests or medical procedures;
• a requirement that the same clinician who performs a patient’s abortion also perform additional tests, services or procedures;
• a limitation on an abortion provider’s ability to prescribe or dispense drugs or provide services via telemedicine;
• a requirement or limitation concerning the physical plant, equipment, staffing, or hospital transfer arrangements of facilities where abortions are performed, or the credentials, hospital privileges, or status of personnel at those facilities;
• a requirement that, prior to obtaining an abortion, a patient make medically unnecessary in-person visits to any individual or entity;
• a limitation on medical training for abortion procedures;
• a prohibition prior to fetal viability, including a prohibition on a particular abortion procedure;
• a prohibition after fetal viability when continuation of the pregnancy would pose a risk to the woman’s life or health;
• a restriction on a woman’s ability to obtain an immediate abortion when a delay would pose a risk to the woman’s health; or
• a restriction on obtaining an abortion prior to fetal viability based on a woman’s reasons or perceived reasons or that requires her to state her reasons before obtaining an abortion.
A measure or action that is similar to a requirement or limitation listed above is prohibited if it singles out abortion services or makes abortion services more difficult to access and does not significantly advance women’s health or the safety of abortion services.
[757] Statement: “Congressional Action to Protect Choice.” By Elizabeth Warren. May 17, 2019. <medium.com>
Congress should pass new federal laws that protect access to reproductive care from right-wing ideologues in the states. Federal laws that ensure real access to birth control and abortion care for all women. Federal laws that will stand no matter what the Supreme Court does. …
Guarantee Reproductive Health Coverage as Part of All Health Coverage. … Congress must also pass the EACH [Equal Access to Abortion Coverage in Health Insurance] Woman Act, which would also prohibit abortion restrictions on private insurance.
[758] Webpage: “Summary of House Resolution 771: Equal Access to Abortion Coverage in Health Insurance (EACH Woman) Act of 2017.” U.S. House of Representatives, 115th Congress (2017–2018). Accessed May 28, 2019 at <www.congress.gov>
Introduced in House (01/31/2017)
Equal Access to Abortion Coverage in Health Insurance (EACH Woman) Act of 2017
This bill requires the federal government: (1) to ensure coverage for abortion care in public health insurance programs including Medicaid, Medicare, and the Children’s Health Insurance Program (CHIP); (2) as an employer or health plan sponsor, to ensure coverage for abortion care for participants and beneficiaries; and (3) as a provider of health services, to ensure that abortion care is made available to individuals who are eligible to receive services.
The federal government may not prohibit, restrict, or otherwise inhibit insurance coverage of abortion care by state or local governments or by private health plans. State and local governments may not prohibit, restrict, or otherwise inhibit insurance coverage of abortion care by private health plans.
[759] Statement: “Congressional Action to Protect Choice.” By Elizabeth Warren. May 17, 2019. <medium.com>
Congress should pass new federal laws that protect access to reproductive care from right-wing ideologues in the states. Federal laws that ensure real access to birth control and abortion care for all women. Federal laws that will stand no matter what the Supreme Court does. …
Ensure Equal Access and Reproductive Justice. Securing a federal right to Roe and ensuring that reproductive health care is available to every woman in America is just the beginning. We must undo the current Administration’s efforts to undermine women’s access to reproductive health care—including ending Trump’s gag rule and fully support Title X family planning funding.
[760] Final rule: “Compliance With Statutory Program Integrity Requirements.” Federal Register, March 4, 2019. <www.govinfo.gov>
The Office of Population Affairs (OPA), in the Office of the Assistant Secretary for Health, issues this final rule to revise the regulations that govern the Title X family planning program (authorized by Title X of the Public Health Service Act) to ensure compliance with, and enhance implementation of, the statutory requirement that none of the funds appropriated for Title X may be used in programs where abortion is a method of family planning and related statutory requirements. Accordingly, OPA amends the Title X regulations to clarify grantee responsibilities under Title X, to remove the requirement for nondirective abortion counseling and referral, to prohibit referral for abortion, and to clarify compliance obligations with state and local laws.
[761] Senate Bill 311: “Born-Alive Abortion Survivors Protection Act.” U.S. Senate, 116th Congress (2019–2020). Accessed July 6, 2019 at <www.congress.gov>
Sponsor: Sen. Sasse, Ben [R–NE] (Introduced 01/31/2019) …
(a) Requirements for health care practitioners.—In the case of an abortion or attempted abortion that results in a child born alive:
(1) Degree of Care Required; Immediate Admission to a Hospital.—Any health care practitioner present at the time the child is born alive shall—
(A) exercise the same degree of professional skill, care, and diligence to preserve the life and health of the child as a reasonably diligent and conscientious health care practitioner would render to any other child born alive at the same gestational age; and
(B) following the exercise of skill, care, and diligence required under subparagraph (A), ensure that the child born alive is immediately transported and admitted to a hospital.
(2) Mandatory Reporting of Violations.—A health care practitioner or any employee of a hospital, a physician’s office, or an abortion clinic who has knowledge of a failure to comply with the requirements of paragraph (1) shall immediately report the failure to an appropriate State or Federal law enforcement agency, or to both.
(b) Penalties.—
(1) In General.—Whoever violates subsection (a) shall be fined under this title, imprisoned for not more than 5 years, or both.
(2) Intentional Killing of Child Born Alive.—Whoever intentionally performs or attempts to perform an overt act that kills a child born alive described under subsection (a), shall be punished as under section 1111 of this title for intentionally killing or attempting to kill a human being.
(c) Bar to prosecution.—The mother of a child born alive described under subsection (a) may not be prosecuted for a violation of this section, an attempt to violate this section, a conspiracy to violate this section, or an offense under section 3 or 4 of this title based on such a violation.
[762] Calculated with data from vote 27: “Cloture on the Motion to Proceed: Born-Alive Abortion Survivors Protection Act.” U.S. Senate, February 25, 2019. <www.senate.gov>
Required For Majority: 3/5 … Vote Result: Cloture on the Motion to Proceed Rejected … Nays … Warren (D–MA) …
|
Party |
Voted “Yes” |
Voted “No” |
Voted “Present” or Did Not Vote † |
|||
|
Number |
Portion |
Number |
Portion |
Number |
Portion |
|
|
Republican |
50 |
94% |
0 |
0% |
3 |
6% |
|
Democrat |
3 |
7% |
42 |
93% |
0 |
0% |
|
Independent |
0 |
0% |
2 |
100% |
0 |
0% |
|
NOTE: † Voting “Present” is effectively the same as not voting. |
||||||
[763] Article: “Google Hearing to Preview Democrats’ Strategy on Big Tech.” By Cecilia Kang and Daisuke Wakabayashi. New York Times, December 7, 2018. <www.nytimes.com>
“Senators Elizabeth Warren of Massachusetts, a Democrat, and Bernie Sanders of Vermont, an independent who caucuses with Democrats, have warned that Amazon and other tech giants aren’t paying fair wages.”
[764] Vote on House Resolution 1833: “Partial-Birth Abortion Ban Act.” U.S. House of Representatives, 104th Congress, September 19, 1996. <clerk.house.gov>
“Nays 137 … Sanders”
[765] Vote on House Resolution 1122: “Partial-Birth Abortion Ban Act.” U.S. House of Representatives, 105th Congress, July 23, 1998. <clerk.house.gov>
“Nays 132 … Sanders”
[766] Vote on Agreeing to the Conference Report, Senate Bill S.3: “Partial-Birth Abortion Ban Act.” U.S. House of Representatives, 108th Congress, October 2, 2003. <clerk.house.gov>
“Nays 142 … Sanders”
[767] Webpage: “Cosponsors of S.1173: Freedom of Choice Act.” U.S. Senate, 110th Congress (2007–2008). Accessed June 3, 2019 at <www.congress.gov>
“Cosponsor Sen. Sanders, Bernard [I-VT] … Date Cosponsored 04/25/2007”
[768] Senate Bill 1173: “Freedom of Choice Act.” U.S. Senate, 110th Congress (2007–2008). Accessed June 5, 2019. <www.congress.gov>
Sec. 4. Interference with Reproductive Health Prohibited. …
(b) Prohibition of Interference—A government may not—
(1) deny or interfere with a woman’s right to choose—
(A) to bear a child;
(B) to terminate a pregnancy prior to viability; or
(C) to terminate a pregnancy after viability where termination is necessary to protect the life or health of the woman; or
(2) discriminate against the exercise of the rights set forth in paragraph (1) in the regulation or provision of benefits, facilities, services, or information. …
Sec. 6. Retroactive Effect.
This Act applies to every Federal, State, and local statute, ordinance, regulation, administrative order, decision, policy, practice, or other action enacted, adopted, or implemented before, on, or after the date of enactment of this Act.
[769] Vote on Senate Amendment 2707 to House Resolution 2764: “Department of State, Foreign Operations, and Related Programs Appropriations Act, 2008.” U.S. Senate, 110th Congress, September 6, 2007. <www.senate.gov>
“Grouped by Vote Position … Nays 45 … Sanders (I-VT)”
[770] Statement of U.S. Senator Sam Brownback (R-KS). Congressional Record, September 6, 2007. Page 11180. <www.congress.gov>
It has been the policy of the United States since 1985, and consistently been the policy of the United States through Republican and Democratic Congresses, through Republican and Democratic administrations. It is commonly referred to as the Kemp–Kasten legislation. It would require the reinsertion of what is known as the Kemp–Kasten law into this legislation. This law helps to ensure that American taxpayers do not subsidize groups and organizations with ties to coercive abortions and forced sterilizations. So this is a narrower subset of the past amendment, the last amendment that I put forward. I would like to read it to my colleagues. It is a short amendment. It is well-known language. I would hope it would get near unanimous support in this body. We would put this language in the bill:
That none of the funds made available in this Act nor any unobligated balances from prior appropriations may be made available to any organization or program which, as determined by the President, supports, or participates in the management of, a program of coercive abortion or involuntary sterilization.
Coerced abortion. Involuntary sterilization. It says you cannot support groups or organizations that participate in each of those. Now, I don’t know of anybody in the Congress who I have ever run into at all that supports coerced abortion or involuntary sterilization.
[771] Senate Bill 311: “Born-Alive Abortion Survivors Protection Act.” U.S. Senate, 116th Congress (2019–2020). Accessed July 6, 2019 at <www.congress.gov>
Sponsor: Sen. Sasse, Ben [R–NE] (Introduced 01/31/2019) …
(a) Requirements for health care practitioners.—In the case of an abortion or attempted abortion that results in a child born alive:
(1) Degree of Care Required; Immediate Admission to a Hospital.—Any health care practitioner present at the time the child is born alive shall—
(A) exercise the same degree of professional skill, care, and diligence to preserve the life and health of the child as a reasonably diligent and conscientious health care practitioner would render to any other child born alive at the same gestational age; and
(B) following the exercise of skill, care, and diligence required under subparagraph (A), ensure that the child born alive is immediately transported and admitted to a hospital.
(2) Mandatory Reporting of Violations.—A health care practitioner or any employee of a hospital, a physician’s office, or an abortion clinic who has knowledge of a failure to comply with the requirements of paragraph (1) shall immediately report the failure to an appropriate State or Federal law enforcement agency, or to both.
(b) Penalties.—
(1) In General.—Whoever violates subsection (a) shall be fined under this title, imprisoned for not more than 5 years, or both.
(2) Intentional Killing of Child Born Alive.—Whoever intentionally performs or attempts to perform an overt act that kills a child born alive described under subsection (a), shall be punished as under section 1111 of this title for intentionally killing or attempting to kill a human being.
(c) Bar to prosecution.—The mother of a child born alive described under subsection (a) may not be prosecuted for a violation of this section, an attempt to violate this section, a conspiracy to violate this section, or an offense under section 3 or 4 of this title based on such a violation.
[772] Calculated with data from vote 27: “Cloture on the Motion to Proceed: Born-Alive Abortion Survivors Protection Act.” U.S. Senate, February 25, 2019. <www.senate.gov>
Required For Majority: 3/5 … Vote Result: Cloture on the Motion to Proceed Rejected … Nays … Sanders (I–VT) …
|
Party |
Voted “Yes” |
Voted “No” |
Voted “Present” or Did Not Vote † |
|||
|
Number |
Portion |
Number |
Portion |
Number |
Portion |
|
|
Republican |
50 |
94% |
0 |
0% |
3 |
6% |
|
Democrat |
3 |
7% |
42 |
93% |
0 |
0% |
|
Independent |
0 |
0% |
2 |
100% |
0 |
0% |
|
NOTE: † Voting “Present” is effectively the same as not voting. |
||||||
[773] Interview with Bernie Sanders.” By Chuck Todd. Meet the Press, NBC, May 19, 2019. <www.nbcnews.com>
Chuck Todd:
Is there any restri—, what are the restri—, Do you believe there should be any restrictions on abortion in law?
Bernie Sanders:
I think that that is a decision that is being—that should be made by the woman and her physician. And I think many of, you know, what people are doing, sadly, is creating a political issue out of a medical issue. So the decision about—women should be able to control their own body. And those decisions are made by a doctor and the woman.
[774] Transcript: “Democratic Candidates Compassion Forum at Messiah College.” CNN, April 13, 2008. <transcripts.cnn.com>
Moderator: “Senator, do you personally believe that life begins at conception? And if not, when does it begin?”
Obama: “This is something that I have not, I think, come to a firm resolution on. I think it’s very hard to know what that means, when life begins. Is it when a cell separates? Is it when the soul stirs? So I don’t presume to know the answer to that question. What I know, as I’ve said before, is that there is something extraordinarily powerful about potential life and that that has a moral weight to it that we take into consideration when we’re having these debates.”
[775] “Full Transcript of Pastor Rick Warren’s Saddleback Forum with John McCain and Barack Obama.” Los Angeles Times, August 19, 2008. <latimesblogs.latimes.com>
Warren: That was a freebie. That was a gimme. That was a gimme, OK? Now, let’s deal with abortion; 40 million abortions since Roe v. Wade. As a pastor, I have to deal with this all of the time, all of the pain and all of the conflicts. I know this is a very complex issue. Forty million abortions, at what point does a baby get human rights, in your view?
Obama: Well, you know, I think that whether you’re looking at it from a theological perspective or a scientific perspective, answering that question with specificity, you know, is above my pay grade.
[776] “Obama Statement on 35th Anniversary of Roe v. Wade Decision.” January 22, 2008. <www.presidency.ucsb.edu>
Thirty-five years after the Supreme Court decided Roe v. Wade, it’s never been more important to protect a woman’s right to choose. Last year, the Supreme Court decided by a vote of 5–4 to uphold the Federal Abortion Ban, and in doing so undermined an important principle of Roe v. Wade: that we must always protect women’s health. With one more vacancy on the Supreme Court, we could be looking at a majority hostile to a women’s fundamental right to choose for the first time since Roe v. Wade. The next president may be asked to nominate that Supreme Court justice. That is what is at stake in this election. …
This anniversary reminds us that it’s not enough to protect the gains of the past—we have to build a future that’s filled with hope and possibility for all Americans.
[777] Speech: “Barack Obama Before Planned Parenthood Action Fund.” July 17, 2007. Transcribed by Laura Echevarria. <bit.ly>
“I have worked on these issues for decades now. I put Roe at the center of my lesson plan on reproductive freedom when I taught Constitutional Law. … On this fundamental issue, I will not yield and Planned Parenthood will not yield.”
[778] Article: “Q&A: Barack Obama.” Interview by Sarah Pulliam and Ted Olsen. Christianity Today, January 23, 2008. <www.christianitytoday.com>
Ultimately, women are in the best position to make a decision at the end of the day about these issues. With significant constraints. For example, I think we can legitimately say—the state can legitimately say—that we are prohibiting late-term abortions as long as there’s an exception for the mother’s health. Those provisions that I voted against typically didn’t have those exceptions, which raises profound questions where you might have a mother at great risk.
[779] “Q&A with Barack Obama.” By Cameron Strang. Relevant Magazine, on July 1, 2008. <www.relevantmagazine.com>
Strang: Based on emails we received, another issue of deep importance to our readers is a candidate’s stance on abortion. We largely know your platform, but there seems to be some real confusion about your position on third-trimester and partial-birth abortions. Can you clarify your stance for us?
Obama: I absolutely can, so please don’t believe the emails. I have repeatedly said that I think it’s entirely appropriate for states to restrict or even prohibit late-term abortions as long as there is a strict, well-defined exception for the health of the mother. Now, I don’t think that “mental distress” qualifies as the health of the mother. I think it has to be a serious physical issue that arises in pregnancy, where there are real, significant problems to the mother carrying that child to term. Otherwise, as long as there is such a medical exception in place, I think we can prohibit late-term abortions.
[780] Article: “Obama Revisits Abortion.” By Jan Crawford Greenburg. ABC News, July 5, 2008. <bit.ly>
In clarifying his remarks, Obama said this afternoon that he has “consistently” said health exceptions are required for laws banning or seriously restricting abortion. …
Speaking to reporters on his campaign plane, Obama said mental health exceptions—which are a real battleground issue in the abortion debate—can be “rigorously” limited to only those women with “serious clinical mental health diseases.” …
“I have consistently been saying that you have to have a health exception on many significant restrictions or bans on abortions, including late-term abortions.
“In the past, there has been some fear on the part of people who—not only people who are anti-abortion, but people who may be in the middle—that that means that if a woman just doesn’t feel good then that is an exception. That’s never been the case. I don’t think that is how it has been interpreted.
“My only point is that in an area like partial birth abortion having a mental, having a health exception can be defined rigorously,” Obama continued.
“It can be defined through physical health. It can be defined by serious clinical mental health diseases. It is not just a matter of feeling blue. I don’t think that’s how pro-choice folks have interpreted it. I don’t think that’s how the courts have interpreted it and I think that’s important to emphasize and understand.”
[781] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] XI: “For the stage subsequent to viability the State, in promoting its interest in the potentiality of human life, may, if it chooses, regulate, and even proscribe, abortion except where necessary, in appropriate medical judgment, for the preservation of the life or health of the mother.”
[Section] VIII:
Specific and direct harm medically diagnosable even in early pregnancy may be involved. Maternity, or additional offspring, may force upon the woman a distressful life and future. Psychological harm may be imminent. Mental and physical health may be taxed by child care. There is also the distress, for all concerned, associated with the unwanted child, and there is the problem of bringing a child into a family already unable, psychologically and otherwise, to care for it. In other cases, as in this one, the additional difficulties and continuing stigma of unwed motherhood may be involved. All these are factors the woman and her responsible physician necessarily will consider in consultation.
[Section] XI: “In Doe v. Bolton, post, p. 179, procedural requirements contained in one of the modern abortion statutes are considered. That opinion and this one, of course, are to be read together.”
[782] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority: …
[Section] IV:
C. … the medical judgment may be exercised in the light of all factors—physical, emotional, psychological, familial, and the woman’s age—relevant to the well-being of the patient. All these factors may relate to health. …
D. The appellants next argue that the District Court should have declared unconstitutional three procedural demands of the Georgia statute: … (2) that the procedure be approved by the hospital staff abortion committee; and (3) that the performing physician’s judgment be confirmed by the independent examinations of the patient by two other licensed physicians. …
We conclude that the interposition of the hospital abortion committee is unduly restrictive of the patient’s rights and needs that, at this point, have already been medically delineated and substantiated by her personal physician. …
There remains, however, the required confirmation by two Georgia-licensed physicians in addition to the recommendation of the pregnant woman’s own consultant (making under the statute, a total of six physicians involved, including the three on the hospital’s abortion committee). We conclude that this provision, too, must fall.
The statute’s emphasis, as has been repetitively noted, is on the attending physician’s “best clinical judgment that an abortion is necessary.” That should be sufficient. The reasons for the presence of the confirmation step in the statute are perhaps apparent, but they are insufficient to withstand constitutional challenge. … If a physician is licensed by the State, he is recognized by the State as capable of exercising acceptable clinical judgment. … If a physician is licensed by the State, he is recognized by the State as capable of exercising acceptable clinical judgment.
[783] Article: “Obama Abortion Dodges Blessed by Planned Parenthood.” By Teddy Davis. ABC News, July 17, 2007. <bit.ly>
“Speaking to ABC News as Obama was preparing to … [address] Planned Parenthood’s national conference in Washington, D.C….”
[784] Speech: “Barack Obama Before Planned Parenthood Action Fund.” July 17, 2007. Transcribed by Laura Echevarria. <bit.ly>
“I have worked on these issues for decades now. I put Roe at the center of my lesson plan on reproductive freedom when I taught Constitutional Law. … There will always be people, many of goodwill, who do not share my view on the issue of choice. On this fundamental issue, I will not yield and Planned Parenthood will not yield.”
[785] Speech: “Barack Obama Before Planned Parenthood Action Fund.” July 17, 2007. Transcribed by Laura Echevarria. <bit.ly>
Dessa Cosma: Um, as you were talking about earlier, the recent Bush Supreme Court’s decision really took away critically important decisions from women and put them in the hands of politicians. And as a result of this, we’re expecting, and have already seen, so much anti-choice legislation at the state level. Um, what would you do at the federal level not only to ensure access to abortion but to make sure that the judicial nominees that you will inevitably be able to pick are true to the core tenets of Roe v. Wade?
Barack Obama: Well, the first thing I’d do as president is, is sign the Freedom of Choice Act. [Applause.] That’s the first thing that I’d do. Um, but the, okay, but, but your question about the federal courts is absolutely on target. I taught Constitutional Law for ten years and I have to say after reading this latest decision and the series of decisions that the Supreme Court has been putting forward that I find it baffling.
[786] Senate Bill 1173: “Freedom of Choice Act.” U.S. Senate, 110th Congress (2007–2008). Accessed June 5, 2019. <www.congress.gov>
“To protect, consistent with Roe v. Wade, a woman’s freedom to choose to bear a child or terminate a pregnancy, and for other purposes.”
NOTE: Introduced by Barbara Boxer (D-California) for herself, Patty Murray (D-Washington), Debbie Stabenow (D-Michigan), Jeff Bingaman (D-New Mexico), Robert Menendez (D-New Jersey), Frank Lautenberg (D-New Jersey), Benjamin Cardin (D-Maryland), Chuck Schumer (D-New York), Diane Feinstein (D-California), Hillary Clinton (D-New York), Barbara Mikulski (D-Maryland), Max Baucus (D-Montana), Maria Cantwell (D-Washington).
[787] Webpage: “Cosponsors of S.1173: Freedom of Choice Act.” U.S. House of Representatives, 110th Congress (2007–2008). Accessed June 5, 2019 at <www.congress.gov>
Sponsor:
Barbara [D-CA]
Cosponsors (19)
Max Baucus, Max [D-MT]
Jeff Bingaman [D-NM]
Sherrod Brown [D-OH]
Maria Cantwell [D-WA]
Benjamin Cardin [D-MD]
Hillary Clinton [D-NY]
Diane Feinstein [D-CA]
John Kerry [D-MA],
Frank Lautenberg [D-NJ]
Joseph Lieberman [D-CT]
Robert Menendez [D-NJ],
Barbara Mikulski [D-MD]
Patty Murray [D-WA]
Barack Obama [D-IL]
Bernie Sanders [I-VT]
Charles Schumer [D-NY]
Debbie Stabenow [D-MI]
Jon Tester [D-MT]
Sheldon Whitehouse [D-RI]
[788] Introduction of Bills and Joint Resolutions: S.1173. Congressional Record, May 11, 2007. Page S6017. <www.govinfo.gov>
Page S6017: “At the request of Mrs. BOXER, the name of the Senator from Illinois (Mr. OBAMA) was added as a cosponsor of S. 1173, a bill to protect, consistent with Roe v. Wade, a woman’s freedom to choose to bear a child or terminate a pregnancy, and for other purposes.”
[789] Senate Bill S.1173: “Freedom of Choice Act.” U.S. Senate, 110th Congress (2007–2008). Accessed June 5, 2019. <www.congress.gov>
Sec. 4. Interference with Reproductive Health Prohibited. …
(b) Prohibition of Interference—A government may not—
(1) deny or interfere with a woman’s right to choose—
(A) to bear a child;
(B) to terminate a pregnancy prior to viability; or
(C) to terminate a pregnancy after viability where termination is necessary to protect the life or health of the woman; or
(2) discriminate against the exercise of the rights set forth in paragraph (1) in the regulation or provision of benefits, facilities, services, or information. …
Sec. 6. Retroactive Effect.
This Act applies to every Federal, State, and local statute, ordinance, regulation, administrative order, decision, policy, practice, or other action enacted, adopted, or implemented before, on, or after the date of enactment of this Act.
[790] House Resolution 1964 IH: “Freedom of Choice Act.” U.S. House of Representatives, 110th Congress (2007–2008). Accessed June 6, 2019. <www.congress.gov>
Sec. 2. Findings. …
(9) Further threatening Roe, the Supreme Court recently upheld the first-ever Federal ban on abortion, which has no exception to protect a woman’s health. The majority decision in Gonzales v. Carhart and Gonzales v. Planned Parenthood Federation of America permits the government to interfere with a woman’s right to choose to terminate a pregnancy and effectively overturns a core tenet of Roe v. Wade by abandoning more than 30 years of protection for women’s health. …
Sec. 4. Interference with Reproductive Health Prohibited.
(a) Statement of Policy—It is the policy of the United States that every woman has the fundamental right to choose to bear a child, to terminate a pregnancy prior to fetal viability, or to terminate a pregnancy after fetal viability when necessary to protect the life or health of the woman.
(b) Prohibition of Interference—A government may not—
(1) deny or interfere with a woman’s right to choose—
(A) to bear a child;
(B) to terminate a pregnancy prior to viability; or
(C) to terminate a pregnancy after viability where termination is necessary to protect the life or health of the woman; or
(2) discriminate against the exercise of the rights set forth in paragraph (1) in the regulation or provision of benefits, facilities, services, or information. …
Sec. 6. Retroactive Effect.
This Act applies to every Federal, State, and local statute, ordinance, regulation, administrative order, decision, policy, practice, or other action enacted, adopted, or implemented before, on, or after the date of enactment of this Act.
NOTE: Introduced by Jerrold Nadler (New York), 56 other Democrats, and one Republican who has since withdrawn his sponsorship.
[791] Webpage: “Cosponsors of House Resolution 1964: Freedom of Choice Act.” U.S. House of Representatives, 110th Congress (2007–2008). Accessed February 9, 2017 at <www.congress.gov>
NOTE: The bill was sponsored by Jerrold Nadler and originally gained 109 cosponsors, but one of these (Republican Jon C. Porter of Nevada) withdrew 4 days later. The party of each sponsor is identified in the next note. The only Republican among them is Christopher Shays of Connecticut.
[792] Webpage: “Cosponsors of House Resolution 1964: Freedom of Choice Act.” U.S. House of Representatives, 110th Congress (2007–2008). Accessed June 5, 2019 at <www.congress.gov>
|
Cosponsor |
Date Cosponsored |
|
Rep. Abercrombie, Neil [D-HI-1]* |
4/19/2007 |
|
Rep. Ackerman, Gary L. [D-NY-5]* |
4/19/2007 |
|
Rep. Allen, Thomas H. [D-ME-1]* |
4/19/2007 |
|
Rep. Arcuri, Michael A. [D-NY-24]* |
4/19/2007 |
|
Rep. Baldwin, Tammy [D-WI-2]* |
4/19/2007 |
|
Rep. Berkley, Shelley [D-NV-1]* |
4/19/2007 |
|
Rep. Berman, Howard L. [D-CA-28]* |
4/19/2007 |
|
Rep. Blumenauer, Earl [D-OR-3]* |
4/19/2007 |
|
Rep. Boucher, Rick [D-VA-9]* |
4/19/2007 |
|
Rep. Capps, Lois [D-CA-23]* |
4/19/2007 |
|
Rep. Cohen, Steve [D-TN-9]* |
4/19/2007 |
|
Rep. Conyers, John, Jr. [D-MI-14]* |
4/19/2007 |
|
Rep. Davis, Danny K. [D-IL-7]* |
4/19/2007 |
|
Rep. Davis, Susan A. [D-CA-53]* |
4/19/2007 |
|
Rep. DeFazio, Peter A. [D-OR-4]* |
4/19/2007 |
|
Rep. Ellison, Keith [D-MN-5]* |
4/19/2007 |
|
Rep. Emanuel, Rahm [D-IL-5]* |
4/19/2007 |
|
Rep. Farr, Sam [D-CA-17]* |
4/19/2007 |
|
Rep. Fattah, Chaka [D-PA-2]* |
4/19/2007 |
|
Rep. Filner, Bob [D-CA-51]* |
4/19/2007 |
|
Rep. Frank, Barney [D-MA-4]* |
4/19/2007 |
|
Rep. Grijalva, Raul M. [D-AZ-7]* |
4/19/2007 |
|
Rep. Harman, Jane [D-CA-36]* |
4/19/2007 |
|
Rep. Hirono, Mazie K. [D-HI-2]* |
4/19/2007 |
|
Rep. Holt, Rush [D-NJ-12]* |
4/19/2007 |
|
Rep. Honda, Michael M. [D-CA-15]* |
4/19/2007 |
|
Rep. Inslee, Jay [D-WA-1]* |
4/19/2007 |
|
Rep. Jackson-Lee, Sheila [D-TX-18]* |
4/19/2007 |
|
Rep. Jackson, Jesse L., Jr. [D-IL-2]* |
4/19/2007 |
|
Rep. Kucinich, Dennis J. [D-OH-10]* |
4/19/2007 |
|
Rep. Lantos, Tom [D-CA-12]* |
4/19/2007 |
|
Rep. Larsen, Rick [D-WA-2]* |
4/19/2007 |
|
Rep. Lee, Barbara [D-CA-9]* |
4/19/2007 |
|
Rep. Loebsack, David [D-IA-2]* |
4/19/2007 |
|
Rep. Lowey, Nita M. [D-NY-18]* |
4/19/2007 |
|
Rep. Matsui, Doris O. [D-CA-5]* |
4/19/2007 |
|
Rep. McCollum, Betty [D-MN-4]* |
4/19/2007 |
|
Rep. McDermott, Jim [D-WA-7]* |
4/19/2007 |
|
Rep. Maloney, Carolyn B. [D-NY-14]* |
4/19/2007 |
|
Rep. Miller, Brad [D-NC-13]* |
4/19/2007 |
|
Rep. Moran, James P. [D-VA-8]* |
4/19/2007 |
|
Rep. Olver, John W. [D-MA-1]* |
4/19/2007 |
|
Rep. Sanchez, Linda T. [D-CA-39]* |
4/19/2007 |
|
Rep. Schakowsky, Janice D. [D-IL-9]* |
4/19/2007 |
|
Rep. Shays, Christopher [R-CT-4]* |
4/19/2007 |
|
Rep. Slaughter, Louise McIntosh [D-NY-28]* |
4/19/2007 |
|
Rep. Solis, Hilda L. [D-CA-32]* |
4/19/2007 |
|
Rep. Stark, Fortney Pete [D-CA-13]* |
4/19/2007 |
|
Rep. Sutton, Betty [D-OH-13]* |
4/19/2007 |
|
Rep. Thompson, Mike [D-CA-1]* |
4/19/2007 |
|
Rep. Towns, Edolphus [D-NY-10]* |
4/19/2007 |
|
Rep. Watson, Diane E. [D-CA-33]* |
4/19/2007 |
|
Rep. Waxman, Henry A. [D-CA-30]* |
4/19/2007 |
|
Rep. Weiner, Anthony D. [D-NY-9]* |
4/19/2007 |
|
Rep. Wexler, Robert [D-FL-19]* |
4/19/2007 |
|
Rep. Woolsey, Lynn C. [D-CA-6]* |
4/19/2007 |
|
Rep. Clay, Wm. Lacy [D-MO-1] |
4/20/2007 |
|
Rep. Norton, Eleanor Holmes [D-DC-At Large] |
4/20/2007 |
|
Rep. McGovern, James P. [D-MA-3] |
4/23/2007 |
|
Rep. Wasserman Schultz, Debbie [D-FL-20] |
4/23/2007 |
|
Rep. Moore, Gwen [D-WI-4] |
4/23/2007 |
|
Rep. Castor, Kathy [D-FL-11] |
4/23/2007 |
|
Rep. Shea-Porter, Carol [D-NH-1] |
4/23/2007 |
|
Rep. McCarthy, Carolyn [D-NY-4] |
4/23/2007 |
|
Rep. Wynn, Albert Russell [D-MD-4] |
4/23/2007 |
|
Rep. Green, Gene [D-TX-29] |
4/23/2007 |
|
Rep. Rangel, Charles B. [D-NY-15] |
4/23/2007 |
|
Rep. Israel, Steve [D-NY-2] |
4/23/2007 |
|
Rep. Wu, David [D-OR-1] |
4/23/2007 |
|
Rep. Clarke, Yvette D. [D-NY-11] |
4/23/2007 |
|
Rep. Payne, Donald M. [D-NJ-10] |
4/24/2007 |
|
Rep. Capuano, Michael E. [D-MA-8] |
4/30/2007 |
|
Rep. Rothman, Steven R. [D-NJ-9] |
4/30/2007 |
|
Rep. Murphy, Christopher [D-CT-5] |
4/30/2007 |
|
Rep. DeGette, Diana [D-CO-1] |
5/2/2007 |
|
Rep. Hastings, Alcee L. [D-FL-23] |
5/2/2007 |
|
Rep. Miller, George [D-CA-7] |
5/2/2007 |
|
Rep. Van Hollen, Chris [D-MD-8] |
5/2/2007 |
|
Rep. Sherman, Brad [D-CA-27] |
5/3/2007 |
|
Rep. Lofgren, Zoe [D-CA-16] |
5/3/2007 |
|
Rep. Lewis, John [D-GA-5] |
5/3/2007 |
|
Rep. Tierney, John F. [D-MA-6] |
5/3/2007 |
|
Rep. Eshoo, Anna G. [D-CA-14] |
5/10/2007 |
|
Rep. Welch, Peter [D-VT-At Large] |
5/21/2007 |
|
Rep. Sanchez, Loretta [D-CA-47] |
5/21/2007 |
|
Rep. Mitchell, Harry E. [D-AZ-5] |
5/23/2007 |
|
Rep. Velazquez, Nydia M. [D-NY-12] |
6/6/2007 |
|
Rep. McNerney, Jerry [D-CA-11] |
6/6/2007 |
|
Rep. Price, David E. [D-NC-4] |
6/6/2007 |
|
Rep. Johnson, Henry C. “Hank,” Jr. [D-GA-4] |
6/12/2007 |
|
Rep. Meehan, Martin T. [D-MA-5] |
6/14/2007 |
|
Rep. Tauscher, Ellen O. [D-CA-10] |
6/18/2007 |
|
Rep. Giffords, Gabrielle [D-AZ-8] |
6/21/2007 |
|
Rep. Napolitano, Grace F. [D-CA-38] |
6/21/2007 |
|
Rep. Baird, Brian [D-WA-3] |
7/11/2007 |
|
Rep. DeLauro, Rosa L. [D-CT-3] |
7/11/2007 |
|
Rep. Carnahan, Russ [D-MO-3] |
7/16/2007 |
|
Rep. Jones, Stephanie Tubbs [D-OH-11] |
9/4/2007 |
|
Rep. Schwartz, Allyson Y. [D-PA-13] |
10/15/2007 |
|
Rep. Carson, Julia [D-IN-7] |
10/22/2007 |
|
Rep. Crowley, Joseph [D-NY-7] |
12/5/2007 |
|
Rep. Pallone, Frank, Jr. [D-NJ-6] |
1/22/2008 |
|
Rep. Gutierrez, Luis V. [D-IL-4] |
1/22/2008 |
|
Rep. Kennedy, Patrick J. [D-RI-1] |
1/28/2008 |
|
Rep. Green, Al [D-TX-9] |
1/28/2008 |
|
Rep. Ruppersberger, C. A. Dutch [D-MD-2] |
1/29/2008 |
|
Rep. Tsongas, Niki [D-MA-5] |
2/12/2008 |
|
Rep. Engel, Eliot L. [D-NY-17] |
3/31/2008 |
|
Rep. Murphy, Patrick J. [D-PA-8] |
9/9/2008 |
|
* = Original cosponsor |
|
[793] Webpage: “Major Actions: H.R. 1964, Freedom of Choice Act.” U.S. House of Representative, 110th Congress (2007–2008). Accessed February 9, 2017 at <www.congress.gov>
4/19/2007: Introduced in House
4/19/2007: Referred to the House Committee on the Judiciary
5/4/2007: Referred to the Subcommittee on the Constitution, Civil Rights, and Civil Liberties.
[794] Webpage: “Cosponsors of S.1173: Freedom of Choice Act.” U.S. Senate, 110th Congress (2007–2008). Accessed June 5, 2019 at <www.congress.gov>
Sponsor:
Barbara [D-CA]
Cosponsors (19)
Max Baucus, Max [D-MT]
Jeff Bingaman [D-NM]
Sherrod Brown [D-OH]
Maria Cantwell [D-WA]
Benjamin Cardin [D-MD]
Hillary Clinton [D-NY]
Diane Feinstein [D-CA]
John Kerry [D-MA],
Frank Lautenberg [D-NJ]
Joseph Lieberman [D-CT]
Robert Menendez [D-NJ],
Barbara Mikulski [D-MD]
Patty Murray [D-WA]
Barack Obama [D-IL]
Bernie Sanders [I-VT]
Charles Schumer [D-NY]
Debbie Stabenow [D-MI]
Jon Tester [D-MT]
Sheldon Whitehouse [D-RI]
[795] Webpage: “Major Actions: Senate Bill 1173, Freedom of Choice Act.” U.S. Congress. Accessed February 9, 2010 at <www.congress.gov>
“4/19/2007: Read twice and referred to the Committee on the Judiciary.”
[796] Article: “Howard Dean’s Abortion Contortions.” By John McCormack. Weekly Standard, June 12, 2008. <www.washingtonexaminer.com>
Yesterday morning at the Christian Science Monitor breakfast meeting, Democratic National Committee Chairman Howard Dean was asked whether the Democratic platform on abortion should be amended. That will be up to Barack Obama and his delegates, Dean said, adding that the Democratic party believes “individuals have a right to make up their own minds in personal matters … but this party also believes that we ought to significantly reduce the number of abortions in this country.”
Given the latter, I asked how he could square Barack Obama’s and the Democratic party’s support for public funding for abortion—which studies show significantly increases the abortion rate.
Dean responded: “Total nonsense. It’s total nonsense that public funding” increases the abortion rate.
NOTE: This article provided the roadmap to the related facts detailed in the footnote below.
[797] Webpage: “The Guttmacher Institute’s Future.” Guttmacher Institute Board of Directors, June 23, 2005. <www.guttmacher.org>
Guiding Principles …
The Institute works to protect, expand and equalize access to information, services and rights that will enable women and men to
• avoid unplanned pregnancies;
• prevent and treat sexually transmitted infections, including HIV [human immunodeficiency virus];
• exercise the right to choose abortion;
• achieve healthy pregnancies and births; and
• have healthy, satisfying sexual relationships.
[798] Article: “Rights Without Access: Revisiting Public Funding of Abortion for Poor Women.” By Heather Boonstra and Adam Sonfield. Guttmacher Report on Public Policy, April 2000. <www.guttmacher.org>
A 1994–1995 AGI [Alan Guttmacher Institute] survey of abortion patients found that in states where Medicaid pays for abortions, women covered by Medicaid have an abortion rate 3.9 times that of women who are not covered, while in states that do not permit Medicaid funding for abortions, Medicaid recipients are only 1.6 times as likely as nonrecipients to have abortions. In explaining this finding, the researchers state that while other factors also may be at play, “the magnitude of the difference indicates that Medicaid coverage of abortion has an important effect on the ability of poor women to end unwanted pregnancies.” Meanwhile, a study published by the Journal of Health Economics in 1999 considered the effects of interruptions in abortion funding in North Carolina (which paid for abortion until 1995). In five instances between 1978 and 1993, the state’s abortion fund was depleted before the end of the fiscal year. During those times when funding was not available, the researchers found, more than one in three women (37%) who would have obtained an abortion if the state had paid for it instead carried the pregnancy to term.
[799] Webpage: “Public Funding for Abortion.” Accessed January 25, 2017 at <bit.ly>
What About Those Who Are Morally or Religiously Opposed to Abortion?
Our tax dollars fund many programs that individual people oppose. For example, those who oppose war on moral or religious grounds pay taxes that are applied to military programs. The congressional bans on abortion funding impose a particular religious or moral viewpoint on those women who rely on government-funded health care. Providing funding for abortion does not encourage or compel women to have abortions, but denying funding compels many women to carry their pregnancies to term. Nondiscriminatory funding would simply place the profoundly personal decision about how to treat a pregnancy back where it belongs—in the hands of the woman who must live with the consequences of that decision.
[800] Webpage: “Oppose Taxpayer Subsidies for Religious Schools.” American Civil Liberties Union. Accessed September 23, 2015 at <www.aclu.org>
School Voucher Schemes Would Force All Taxpayers to Support Religious Beliefs and Practices with Which They May Strongly Disagree.
At the heart of these proposals are the goals of commingling church and state in the classroom and diverting public funds to private and parochial schools. Religious schools represent 85 percent of the total private school enrollment in the United States. These schools by their nature combine proselytization with education and therefore should not be funded by taxpayer dollars.
[801] Webpage: “About the Society.” Society of Professional Journalists. Accessed February 2017 at <www.spj.org>
“The Society of Professional Journalists is the nation’s most broad-based journalism organization, dedicated to encouraging the free practice of journalism and stimulating high standards of ethical behavior.”
[802] Webpage: “Diversity Guidelines.” Society of Professional Journalists, October 6, 2001. <www.spj.org>
On Oct. 6, 2001 at its National Convention in Seattle, the Society of Professional Journalists passed a resolution urging members and fellow journalists to take steps against racial profiling in their coverage of the war on terrorism and to reaffirm their commitment to:
Use language that is informative and not inflammatory; …
When writing about terrorism, remember to include white supremacist, radical anti-abortionists and other groups with a history of such activity. …
Avoid using word combinations such as “Islamic terrorist” or “Muslim extremist” that are misleading because they link whole religions to criminal activity.
[803] Transcript: “Senator John McCain at the Republican Party of Iowa, Abraham Lincoln Unity Dinner.” Democracy in Action, George Washington University, April 14, 2007. <p2008.org>
America stands for an ideal that all people are endowed by their Creator with certain unalienable rights to life, liberty and the pursuit of happiness. I know what it’s like to live without those rights and I have an obligation to advocate them where ever they are denied. In Bosnia or in Burma in Cuba or in the Middle East and in our own country when we fail to respect the inherent dignity of all human life, born or unborn, and that’s why for 24 years, without changing, without wavering, I have a steadfast and strong advocacy and voting record in support of the rights of the unborn.
[804] Transcript: “Former Governor Mike Huckabee at the Republican Party of Iowa, Abraham Lincoln Unity Dinner.” Democracy in Action, George Washington University, April 14, 2007. <p2008.org>
“I’m not late in declaring that I believe life begins at conception and that we ought to protect human life and that’s one of the reasons that I am a Republican today, because it was the only party that gave people like me a voice and a choice.”
[805] Article: “G.O.P. Candidates Lay Into Democrats, Not One Another.” By Adam Nagourney. New York Times, April 15, 2007. <www.nytimes.com>
[A]n audience of the state’s most active Republicans listened attentively as candidates proclaimed their strong opposition to abortion rights….
Although the event was called a “Unity Dinner,” the speeches reflected divisions among the Republicans on various issues, in particular abortion. Several candidates, including Mr. McCain of Arizona and Mike Huckabee of Arkansas, presented themselves as lifelong opponents of abortion rights, drawing clear if unspoken contrasts with Mr. Giuliani, who supports abortion rights, and Mr. Romney, who once supported abortion rights but now opposes them. …
Mr. Huckabee, a former governor of Arkansas, pointedly noted that he had always been an opponent of abortion rights….
[806] Note that most all of the people described by the media as “opponents of abortion rights” are not unilaterally opposed to abortion. Nearly all think that abortion should be legal when there is a threat to the life of the mother, and some think there should be exceptions for rape and incest.† This also true of the examples that follow. The people cited are not unilaterally opposed to the “rights” in question, but think that other “rights” should take precedence. The same applies to people who think that a pre-birth human’s “right to life” should take precedence over other “rights.”
NOTE: † Since 1989, various Republicans have sponsored at least 22 resolutions proposing a Constitutional Amendment that would guarantee pre-birth humans the right to life, all of them containing an exception to protect the life of the mother. Six of these resolutions also include exceptions for cases of rape or incest. [Search performed on September 20, 2023 at <www.congress.gov>. Just Facts searched bill texts from the 101st to 118th Congresses for: “amendment to the Constitution of the United States with respect to the right to life.”]
[807] a) Second Amendment to the Constitution of the United States. Ratified December 15, 1791. <justfacts.com>
“A well regulated Militia, being necessary to the security of a free State, the right of the people to keep and bear Arms shall not be infringed.”
b) Editorial: “Lock and Load.” By the Editorial Board. New York Times, June 27, 2008. <www.nytimes.com>
“Even if there were a constitutional right to possess guns for nonmilitary uses, constitutional rights are not absolute.”
[808] a) Fifth Amendment to the Constitution of the United States. Ratified December 15, 1791. <justfacts.com>
“[N]or shall private property be taken for public use, without just compensation.”
b) Editorial: “The Limits of Property Rights.” By the Editorial Board. New York Times, June 24, 2005. <www.nytimes.com>
“The Supreme Court’s ruling yesterday that the economically troubled city of New London, Conn., can use its power of eminent domain to spur development was a welcome vindication of cities’ ability to act in the public interest. It also is a setback to the ‘property rights’ movement, which is trying to block government from imposing reasonable zoning and environmental regulations.”
[809] a) Ninth Amendment to the Constitution of the United States. Ratified December 15, 1791. <justfacts.com>
“The enumeration in the Constitution, of certain rights, shall not be construed to deny or disparage others retained by the people.”
b) Article: “Parents Protest Gay-Themed School Plays.” By Ellen Sorokin. Washington Times, February 21, 2002.
“A group of parents is suing a public school district in Novato, Calif., for allowing their elementary school-age children to see pro-homosexual plays at school without any prior notice or parental consent.”
[810] a) Fifth Amendment to the Constitution of the United States. Ratified December 15, 1791. <justfacts.com>
“No person shall … be deprived of life, liberty, or property, without due process of law….”
b) Ruling: Korematsu v. United States. U.S. Supreme Court, December 18, 1944. Decided 6–3. Majority: Black, Douglas, Reed, Rutledge, Stone. Concurring: Frankfurter. Dissenting: Roberts, Murphy, Jackson. <caselaw.findlaw.com>
Majority:
It is said that we are dealing here with the case of imprisonment of a citizen in a concentration camp solely because of his ancestry, without evidence or inquiry concerning his loyalty and good disposition towards the United States. Our task would be simple, our duty clear, were this a case involving the imprisonment of a loyal citizen in a concentration camp because of racial prejudice. Regardless of the true nature of the assembly and relocation centers—and we deem it unjustifiable to call them concentration camps with all the ugly connotations that term implies—we are dealing specifically with nothing but an exclusion order. To cast this case into outlines of racial prejudice, without reference to the real military dangers which were presented, merely confuses the issue. Korematsu was not excluded from the Military Area because of hostility to him or his race. He was excluded because we are at war with the Japanese Empire, because the properly constituted military authorities feared an invasion of our West Coast and felt constrained to take proper security measures, because they decided that the military urgency of the situation demanded that all citizens of Japanese ancestry be segregated from the West Coast temporarily, and finally, because Congress, reposing its confidence in this time of war in our military leaders—as inevitably it must—determined that they should have the power to do just this. There was evidence of disloyalty on the part of some, the military authorities considered that the need for action was great, and time was short. We cannot—by availing ourselves of the calm perspective of hindsight—now say that at that time these actions were unjustified.
[811] a) Tenth Amendment to the Constitution of the United States. Ratified December 15, 1791. <justfacts.com>
“The powers not delegated to the United States by the Constitution, nor prohibited by it to the States, are reserved to the States respectively, or to the people.”
b) Eleventh Amendment to the Constitution of the United States. Ratified February 7, 1795. <justfacts.com>
“The Judicial power of the United States shall not be construed to extend to any suit in law or equity, commenced or prosecuted against one of the United States by Citizens of another State, or by Citizens or Subjects of any Foreign State.”
c) Article: “High Court Voids States’ Immunity.” By Frank J. Murray. Washington Times, May 28, 2003. <www.washingtontimes.com>
“The Supreme Court ruled yesterday that a Nevada social worker may sue the state for firing him in violation of the Family and Medical Leave Act, a decision that raised the first barrier to states’ broad 11th Amendment immunity against private lawsuits.”
[812] a) First Amendment to the Constitution of the United States. Ratified December 15, 1791. <justfacts.com>
“Congress shall make no law respecting an establishment of religion, or prohibiting the free exercise thereof….”
b) Code of Virginia, Section 22.1–203: “Daily Observance of One Minute of Silence.” Code of Virginia. Accessed July 2008 at <law.justia.com>
In order that the right of every pupil to the free exercise of religion be guaranteed within the schools and that the freedom of each individual pupil be subject to the least possible pressure from the Commonwealth either to engage in, or to refrain from, religious observation on school grounds, the school board of each school division shall establish the daily observance of one minute of silence in each classroom of the division.
During such one-minute period of silence, the teacher responsible for each classroom shall take care that all pupils remain seated and silent and make no distracting display to the end that each pupil may, in the exercise of his or her individual choice, meditate, pray, or engage in any other silent activity which does not interfere with, distract, or impede other pupils in the like exercise of individual choice.
c) Article: “Justices Uphold Moment of Silence: The Supreme Court Refuses to Hear a Challenge to a Mandatory Silent Minute in Virginia Schools.” By Anne Gearan. Associated Press, October 30, 2001. <www.greensboro.com>
“The Supreme Court turned away a challenge to Virginia’s mandatory minute of silence in schools on Monday, declining to take a closer look at the silent prayer issue it last examined 16 years ago.”
[813] Just Facts searched the New York Times and Washington Post on July 27, 2021 and the Associated Press on August 16, 2008 through LexisNexis. Note that some articles contain the quoted phrases more than once, and thus, the numbers cited may represent an undercount. Searches for “opponent(s) of states’ rights” were also performed for the spelling variant “opponent(s) of states rights.”
[814] Entry: “abortion, partial-birth.” Melloni’s Illustrated Medical Dictionary (4th edition). Parthenon Publishing Group, 2002.
Page 2: “partial-birth a. (PBA) Common term for termination of a late pregnancy with a breech presentation. Labor is induced by conventional methods; the cervix is widely dilated and delivery is expedited by evacuation the cranial contents with a suction catheter, then compressing the cranium.”
[815] Policy H-5.982: “Late-Term Pregnancy Termination Techniques.” American Medical Association. Accessed July 2008 at <www.ama-assn.org>
The term “partial birth abortion” is not a medical term. The AMA [American Medical Association] will use the term “intact dilatation and extraction” (or intact D&X) to refer to a specific procedure comprised of the following elements: deliberate dilatation of the cervix, usually over a sequence of days; instrumental or manual conversion of the fetus to a footling breech; breech extraction of the body excepting the head; and partial evacuation of the intracranial contents of the fetus to effect vaginal delivery of a dead but otherwise intact fetus. This procedure is distinct from dilatation and evacuation (D&E) procedures more commonly used to induce abortion after the first trimester. Because “partial birth abortion” is not a medical term it will not be used by the AMA.
[816] Book: AMA Manual of Style: A Guide for Authors and Editors (10th edition). Oxford University Press, 2007.
Page 295: “During an interview, authors should avoid use of medical/scientific jargon, acronyms, and too many statistics; explain commonly used jargon and acronyms and provide easily understood statistics …”
[817] Transcript: NOW with Bill Moyers. PBS, May 16, 2003. <billmoyers.com>
Breslauer: The term “partial birth abortion” was invented by the anti-abortion community to describe a procedure in which a fetus is partially delivered outside the womb. Doctors don’t even use the term. The closest medical procedure to so-called partial birth abortion, accounts for less than one quarter of one percent of all abortions in this country. So why such impassioned debate?
[818] Book: English for Journalists (2nd edition). By Wynford Hicks. Routledge, 1998.
Page 73: “Jargon is specialized vocabulary, familiar to the members of a group, trade or profession. If you write for a newspaper or general magazine you should try to translate jargon into ordinary English whenever you can. … A common source of jargon is scientific, medical, government and legal handouts.”
[819] Editorial: “Abortion and the Court.” By the Editorial Board. Chicago Tribune, July 13, 2005. Section C, Page 26.
“There is a chance of reversal, though, on certain late-term abortions. Five years ago, by a 5–4 vote, the court struck down a Nebraska law banning this procedure, also known as intact dilation and extraction, concluding that the measure imposed an undue burden on the right to abortion.”
[820] Book: The New York Public Library Writer’s Guide to Style and Usage. Edited by Andrea J. Sutcliffe. Stonesong Press/Harper Collins, 1994.
Page 586:
The word jargon originally meant a “confused, unintelligible language”; however, it has now come to mean the “technical terminology or characteristic idiom of a special activity or group.” When writing for a specialized audience—one familiar with the topic or field—a writer must use jargon; it is the common idiom. When writing for a lay audience or the general public, a writer should use jargon only when necessary and define it carefully. Where plain English serves equally well, it should be used instead
[821] Book: The New Oxford Guide to Writing. By Thomas S. Kane. Oxford University Press, 1988.
Page 199: “Jargon is technical language misused. Technical language, the precise diction demanded by any specialized trade or profession, is necessary when experts communicate with one another. It becomes jargon when it is applied outside the limits of technical discourse.”
[822] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] VIII:
Specific and direct harm medically diagnosable even in early pregnancy may be involved. Maternity, or additional offspring, may force upon the woman a distressful life and future. Psychological harm may be imminent. Mental and physical health may be taxed by child care. There is also the distress, for all concerned, associated with the unwanted child, and there is the problem of bringing a child into a family already unable, psychologically and otherwise, to care for it. In other cases, as in this one, the additional difficulties and continuing stigma of unwed motherhood may be involved. All these are factors the woman and her responsible physician necessarily will consider in consultation.
[Section] XI:
For the stage subsequent to viability the State, in promoting its interest in the potentiality of human life, may, if it chooses, regulate, and even proscribe, abortion except where necessary, in appropriate medical judgment, for the preservation of the life or health of the mother. …
In Doe v. Bolton, post, p. 179, procedural requirements contained in one of the modern abortion statutes are considered. That opinion and this one, of course, are to be read together.
[823] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority: …
[Section] IV:
C. … the medical judgment may be exercised in the light of all factors—physical, emotional, psychological, familial, and the woman’s age—relevant to the well-being of the patient. All these factors may relate to health. …
D. The appellants next argue that the District Court should have declared unconstitutional three procedural demands of the Georgia statute: … (2) that the procedure be approved by the hospital staff abortion committee; and (3) that the performing physician’s judgment be confirmed by the independent examinations of the patient by two other licensed physicians. …
We conclude that the interposition of the hospital abortion committee is unduly restrictive of the patient’s rights and needs that, at this point, have already been medically delineated and substantiated by her personal physician. …
There remains, however, the required confirmation by two Georgia-licensed physicians in addition to the recommendation of the pregnant woman’s own consultant (making under the statute, a total of six physicians involved, including the three on the hospital’s abortion committee). We conclude that this provision, too, must fall.
The statute’s emphasis, as has been repetitively noted, is on the attending physician’s “best clinical judgment that an abortion is necessary.” That should be sufficient. The reasons for the presence of the confirmation step in the statute are perhaps apparent, but they are insufficient to withstand constitutional challenge. … If a physician is licensed by the State, he is recognized by the State as capable of exercising acceptable clinical judgment.
[824] Ruling: Planned Parenthood of Southeastern PA v. Casey. United States Supreme Court. June 29, 1992. <caselaw.findlaw.com>
Majority:
[825] Article: “Public Opinion About Abortion—An In-Depth Review: The Pro-Choice/Pro-Life Divide.” By Lydia Saad. Gallup, January 22, 2002. <www.gallup.com>
Page 2:
The following chart illustrates the wide range of attitudes toward abortion recorded across a diverse set of questions about the subject. The figures in the chart are based on 146 survey questions asked by 18 different polling organizations over the past five years. …
For the most part, attitudes pertaining to particular aspects of abortion are consistent across differently worded questions. But in a few cases, particularly with respect to Roe v. Wade, the responses vary widely, depending on the information provided in the question.
Page 3:
Most survey questions about Roe v. Wade provide the respondent with information about the case, and these details appear to have a major impact on the answers.
… If Roe v. Wade is presented only as legalizing abortion in the first three months, support for the decision is much higher than if it is characterized as making abortion legal throughout pregnancy or for any reason.
[826] Webpage: “Abortion and Birth Control.” PollingReport.com. Accessed July 2008 at <bit.ly>
The Harris Poll. Oct. 16–23, 2007. … “In 1973, the U.S. Supreme Court decided that states laws which made it illegal for a woman to have an abortion up to three months of pregnancy were unconstitutional, and that the decision on whether a woman should have an abortion up to three months of pregnancy should be left to the woman and her doctor to decide.”
NBC News/Wall Street Journal Poll…. Dec. 9–12, 2005. … “The Supreme Court’s 1973 Roe versus Wade decision established a woman’s constitutional right to an abortion, at least in the first three months of pregnancy.”
Pew Research Center/Pew Forum on Religion & Public Life survey…. Nov. 3–6, 2005. … “In 1973 the Roe versus Wade decision established a woman’s constitutional right to an abortion, at least in the first three months of pregnancy. Would you like to see the Supreme Court completely overturn its Roe versus Wade decision, or not?”
Quinnipiac University Poll. Dec. 7–12, 2004. … “The 1973 Supreme Court ruling called Roe. v. Wade made abortion in the first three months of pregnancy legal. Do you think President Bush should nominate Supreme Court justices who would uphold the Roe. v. Wade decision, or nominate Supreme Court justices who would overturn the Roe v. Wade decision?”
Associated Press-Ipsos poll conducted by Ipsos-Public Affairs. Nov. 19–21, 2004. … “The 1973 Supreme Court ruling called Roe v. Wade made abortion in the first three months of pregnancy legal.”
[827] There are other Associated Press articles that used the same verbiage. The three listed below are exemplars:
a) Article: “Vatican Pushing Mexico in Abortion Fight.” Associated Press, March 24, 2007. <www.ctvnews.ca>
“Most Latin American countries, including Mexico, allow abortion if the woman’s life is in danger or in cases of rape or incest. In November, Nicaragua passed a law banning abortion in all cases. Cuba permits abortions within the first 12 weeks of pregnancy, as does the United States.”
b) Article: “Mexicans March to Legalize Abortion.” Associated Press, March 30, 2007. <www.nbcnews.com>
“Most Latin American countries, including Mexico, allow abortion if the woman’s life is in danger or in cases of rape or incest. In November, Nicaragua passed a law banning abortion in all cases. Cuba permits abortions within the first 12 weeks of pregnancy, as does the United States.”
c) Article: “Mexico Court Shows Support for Abortion Law.” Associated Press, August 27, 2008. <www.nbcnews.com>
“Most Latin American countries allow abortion if the woman’s life is in danger or in cases of rape or incest. In 2006, Nicaragua banned abortion in all cases. Cuba permits abortions within the first 12 weeks of pregnancy, as does the United States.”
[828] Search performed August 27, 2008 via <www.google.com>. Results include:
|
baltimoresun.com |
bellinghamherald.com |
boston.com |
|
breitbart.com |
cbsnews.com |
centredaily.com |
|
chron.com |
cleveland.com |
cnsnews.com |
|
comcast.net |
contracostatimes.com |
daytondailynews.com |
|
denverpost.com |
duluthnewstribune.com |
elpasotimes.com |
|
examiner.com |
federalnewsradio.com |
fortmilltimes.com |
|
foxnews.com |
gjsentinel.com |
greenwichtime.com |
|
guardian.co.uk |
ibtimes.com |
iht.com |
|
inyork.com |
journalgazette.net |
kansascity.com |
|
khou.com |
ktar.com |
latimes.com |
|
ledger-enquirer.com |
lehighvalleylive.com |
madison.com |
|
metrobostonnews.com |
miamiherald.com |
msnbc.com |
|
my.freeze.com |
mymotherlode.com |
news.aol.com |
|
news.yahoo.com |
newstimes.com |
newsvine.com |
|
nola.com |
nydailynews.com |
nypost.com |
|
ohio.com |
onenewsnow.com |
oregonlive.com |
|
palmbeachpost.com |
philly.com |
pressofatlanticcity.com |
|
pr-inside.com |
publicopiniononline.com |
realclearworld.com |
|
realtime.com |
rockymounttelegram.com |
sacbee.com |
|
salon.com |
sanluisobispo.com |
santacruzsentinel.com |
|
sfgate.com |
signonsandiego.com |
silive.com |
|
southernledger.com |
sunherald.com |
syracuse.com |
|
thenewstribune.com |
twincities.com |
usatoday.com |
|
victoriaadvocate.com |
washingtonpost.com |
washingtontimes.com |
|
wor710.com |
wtop.com |
[829] Ruling: Roe v. Wade. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Burger, Brennan, Douglas, Stewart, Marshall, Powell. Concurring: Burger, Douglas, Stewart. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority:
[Section] VIII:
Specific and direct harm medically diagnosable even in early pregnancy may be involved. Maternity, or additional offspring, may force upon the woman a distressful life and future. Psychological harm may be imminent. Mental and physical health may be taxed by child care. There is also the distress, for all concerned, associated with the unwanted child, and there is the problem of bringing a child into a family already unable, psychologically and otherwise, to care for it. In other cases, as in this one, the additional difficulties and continuing stigma of unwed motherhood may be involved. All these are factors the woman and her responsible physician necessarily will consider in consultation.
[Section] XI:
For the stage subsequent to viability the State, in promoting its interest in the potentiality of human life, may, if it chooses, regulate, and even proscribe, abortion except where necessary, in appropriate medical judgment, for the preservation of the life or health of the mother. …
In Doe v. Bolton, post, p. 179, procedural requirements contained in one of the modern abortion statutes are considered. That opinion and this one, of course, are to be read together.
[830] Ruling: Doe v. Bolton. U.S. Supreme Court, January 22, 1973. Decided 7–2. Majority: Blackmun, Brennan, Stewart, Marshall, Powell. Concurring: Burger, Douglas. Dissenting: White, Rehnquist. <caselaw.findlaw.com>
Majority: …
[Section] IV: “[T]he medical judgment may be exercised in the light of all factors—physical, emotional, psychological, familial, and the woman’s age—relevant to the wellbeing of the patient. All these factors may relate to health.”
[831] Ruling: Planned Parenthood of Southeastern PA v. Casey. United States Supreme Court. June 29, 1992. <caselaw.findlaw.com>
Majority:
It must be stated at the outset and with clarity that Roe’s essential holding, the holding we reaffirm, has three parts. First is a recognition of the right of the woman to choose to have an abortion before viability and to obtain it without undue interference from the State. Before viability, the State’s interests are not strong enough to support a prohibition of abortion or the imposition of a substantial obstacle to the woman’s effective right to elect the procedure. Second is a confirmation of the State’s power to restrict abortions after fetal viability if the law contains exceptions for pregnancies which endanger the woman’s life or health. And third is the principle that the State has legitimate interests from the outset of the pregnancy in protecting the health of the woman and the life of the fetus that may become a child.
[832] Webpage: “Nina Totenberg, NPR Biography.” National Public Radio. Accessed March 11, 2019 at <archive2.mrc.org>
“Nina Totenberg is NPR’s award-winning legal affairs correspondent. Her reports air regularly on NPR’s critically acclaimed newsmagazines All Things Considered, Morning Edition, and Weekend Edition.”
[833] Webpage: “CyberAlert.” Media Research Center, July 6, 2000. <archive2.mrc.org>
Nina Totenberg: “You know, there’s a very interesting thing about so-called ‘partial birth abortion,’ and that’s not a medical term, that’s a political term, as all the courts have said, and that is that both the pro-life and pro-choice forces have conspired in an odd sort of way to make the public totally misunderstand what this is all about. These are not late-term abortions. Those are banned in every state. Third-trimester abortions are banned in every state except to save the life and the health of the mother. These are by and large second trimester abortions, and the important thing here that Justice O’Connor said is if a doctor thinks a procedure is necessary to, for the life of the mother, he or she can use that procedure, and any law that interferes with that is gonna be unconstitutional.”
[834] Editorial: “Play Doctor—and Judge.” By the Editorial Board. Washington Post, October 27, 2003. Page A18. <www.washingtonpost.com>
The measure prohibits one form of abortion, performed in the late second trimester or third trimester of pregnancy; it is gruesome, as indeed are all abortions this late in pregnancy. But most states already bar abortions after the point of viability, unless the procedure is necessary to preserve the life or health of the mother, and Congress could have done likewise.
[835] Article: “Fact Check: New York’s Abortion Law Doesn’t Allow Any Abortion ‘Up Until Birth,’ as Claimed.” By Adrienne Dunn. USA Today, April 30, 2020. Updated 5/6/2020. <www.usatoday.com>
The claim: New York’s Gov. Andrew Cuomo signed a bill legalizing abortion up until birth …
New York’s Reproductive Health Act allows practitioners to perform an abortion on a patient who is 24 weeks or more away from the start of a pregnancy if the fetus is not viable or the abortion is necessary “to protect the patient’s life or health.”
The law does not define “health” or viability of a fetus. The determination of these factors must be made by a “health care practitioner licensed, certified, or authorized” under state law, “acting within his or her lawful scope of practice.”
Before Cuomo signed the legislation, abortions after 24 weeks were allowed only when the mother’s life was at risk. They otherwise were criminalized. …
While it is true that New York’s abortion law allows procedures after 24 weeks, there are rules guiding that procedure: if the fetus is not viable or if the health or life of the mother is at risk. If medical practitioners determine that either of these factors are present, the mother can choose to have an abortion.
It is false to state or imply that any abortion can occur in New York “up until birth” as the social posts claims. That is misleading. Additionally, no state in the U.S. allows abortion “up until birth.”
[836] Article: “Fact-Checking Donald Trump’s 2020 RNC Speech.” PolitiFact, August 27, 2020. <www.politifact.com>
[Donald Trump]: “Joe Biden claims he has empathy for the vulnerable, yet the party he leads supports the extreme late-term abortion of defenseless babies right up to the moment of birth.”
This mischaracterizes the Democratic Party’s stance on abortion and Biden’s position.
Biden has said he would codify the Supreme Court’s ruling in Roe v. Wade and related precedents. This would generally limit abortions to the first 20 to 24 weeks of gestation. States are allowed under court rulings to ban abortion after the point at which the fetus can sustain life, usually considered to be between 24 and 28 weeks from the mother’s last menstrual period — and 43 states do. But the rulings require states to make exceptions “to preserve the life or health of the mother.” Late-term abortions are very rare, about 1%.
The Democratic Party platform holds that “every woman should have access to quality reproductive health care services, including safe and legal abortion—regardless of where she lives, how much money she makes, or how she is insured.” It does not address late-term abortion.
[837] Article: “Fact-Checking Trump’s Speech and More: Night 4 of the Republican National Convention.” By Sheryl Gay Stolberg. New York Times, September 30, 2020. <www.nytimes.com>
The proposed legislation prompted Senator Ted Cruz, Republican of Texas, to falsely claim that Democrats support “abortion up until the moment of birth and even, horrifically, after that.” Other Republicans have echoed the claim.
Democrats support codifying Roe v. Wade, the landmark 1973 decision that held states could prohibit abortion after fetal viability—the point at which fetuses can sustain life outside the womb. The current Supreme Court standard holds that states may prohibit abortion after fetal viability so long as there are exceptions for the life and health of the mother.
[838] Article: “Fact Check: Pence Echoes Trump’s False Claims at Vice Presidential Debate.” By Caroline Kelly. CNN, October 8, 2020. <www.cnn.com>
But “late-term” is not a medical term, and no candidate in either political party supports abortion “up to the moment of birth.”
Asked last month about the Democratic nominee’s stance on abortion and Pence’s frequent “up to birth” claim, a Biden campaign official told CNN that Biden supports Roe v. Wade….
Harris has expressed support for allowing post-viability abortions in some cases. In 2019, she co-sponsored the Women’s Health Protection Act, which would prevent “a prohibition on abortion after fetal viability when, in the good-faith medical judgment of the treating health care provider, continuation of the pregnancy would pose a risk to the pregnant patient’s life or health.”
[839] Full Text of Letter
[840] Full Text of Letter
[841] Report: “MediaWatch: February 1989.” Media Research Center, February 1989. <archive2.mrc.org>
On January 9 Surgeon General C. Everett Koop filed a report with the President on the health effects of abortion. Here’s what the network anchors told viewers that night: ABC’s Peter Jennings said “a new report by the Surgeon General concludes that abortion causes little if any physical or emotional harm to women.” Dan Rather of CBS announced that “Surgeon General C. Everett Koop … reportedly concluded that a woman who has an abortion suffers little if any physical or emotional harm from the experience.” NBC’s Tom Brokaw declared that “Koop reports he has not found conclusive evidence that abortions have harmful psychological effects on the women who have them,” but Koop “found that there is a whole segment of the population that says, quote, ‘the best thing that happened to me was my abortion.’ ”
[842] Article: “The Times Poll Public and Press—Two Viewpoints Series: First of Two Parts.” By David Shaw. Los Angeles Times, Aug 11, 1985. <www.latimes.com>
On the issue of “allowing women to have an abortion” … the newspaper journalists say they favor allowing women to have an abortion—by an almost 6–1 margin… (Readers also approve allowing women to have an abortion, though by a much narrower margin—51% to 42%.) …
… [M]embers of the press (at least the 3,165 newspaper reporters and editors from 621 newspapers interviewed for this story)….
[843] Transcript: Talkback Live. Hosted by Tucker Carlson. CNN, December 19, 2001. <transcripts.cnn.com>
Carlson: Well, Hal Bruno, let ask me you this. And honestly, what percentage of—of the news media—the network news media—how about just ABC News—is pro-choice? It’s got to be above 80, don’t you think?
Bruno: Well, we have a tremendous number of women that have come into journalism in the last 20 years…
Carlson: But not all women…
Bruno: …and most women tend to be pro-choice. So I would have to say—obviously, I’d say a majority of the people who work in the news—not just at ABC, but who work in the news—are pro-choice. But I think the majority of the country probably is pro-choice too.
[844] Article: “Public Opinion About Abortion—An In-Depth Review: Gender, Religion and Other Group Attitudes Toward Abortion.” By Lydia Saad. Gallup, January 22, 2002. <www.gallup.com>
NOTE: The poll was conducted in May 2001.
[845] Article: “Poll: Abortion Is Manslaughter.” Newsmax, January 8, 2001. <www.newsmax.com>
When asked to choose between two statements: “Abortion destroys a human life and is manslaughter” or “Abortion does not destroy a life and is not manslaughter,” 51 percent of respondents of the Zogby “American Values” poll believed the first statement. Thirty-five percent of 1,005 likely voters believed that abortion does not destroy a life and is not manslaughter. …
Men and women’s responses were statistically the same, with 51 percent of men and women agreeing that abortion destroys a human life. Thirty-seven percent of men and 33 percent of women said abortion does not destroy life and is not manslaughter.
[846] Transcript: Talkback Live. Hosted by Tucker Carlson. CNN, December 19, 2001. <transcripts.cnn.com>
“[A]nd most women tend to be pro-choice. So I would have to say—obviously, I’d say a majority of the people who work in the news—not just at ABC, but who work in the news—are pro-choice. But I think the majority of the country probably is pro-choice too.”
[847] Article: “Public Opinion About Abortion—An In-Depth Review: Gender, Religion and Other Group Attitudes Toward Abortion.” By Lydia Saad. Gallup, January 22, 2002. <www.gallup.com>
NOTE: The poll was conducted in May 2001. Percentages do not add up to 100% because some agreed with neither statement or were unsure.






















